
Abstract
Background
Statins have several effects beyond their well-known antihyperlipidemic activity, which include immunomodulatory, antioxidative and anticoagulant effects. In this study, we have tested the possible antimicrobial activity of statins against a range of standard bacterial strains and bacterial clinical isolates.
Methods
Minimum inhibitory concentrations (MIC) values were evaluated and compared among three members of the statins drug (atorvastatin, simvastatin, and rosuvastatin).
Results
It was revealed that statins are able to induce variable degrees of antibacterial activity with atorvastatin, and simvastatin being the more potent than rosuvastatin. Methicillin-sensitive staphylococcus aureus (MSSA), methicillin-resistant staphylococcus aureus (MRSA), vancomycin-susceptible enterococci (VSE), vancomycin-resistant enterococcus (VRE), acinetobacter baumannii, staphylococcus epidermidis, and enterobacter aerogenes, were more sensitive to both atorvastatin, and simvastatin compared to rosuvastatin. On the other hand, escherichia coli, proteus mirabilis, and enterobacter cloacae were more sensitive to atorvastatin compared to both simvastatin and rosuvastatin. Furthermore, most clinical isolates were less sensitive to statins compared to their corresponding standard strains.
Conclusion
Our findings might raise the possibility of a potentially important antibacterial class effect for statins especially, atorvastatin and simvastatin.
Similar content being viewed by others


Background
Statins, also known as 3-hydroxy-3-methyl-glutaryl (HMG)-CoA reductase inhibitors, are a potent antihyperlipidemic drug group that is widely used for the treatment of hyperlipidemia. The HMG-CoA reductase is the enzyme responsible for the rate-limiting step in the cholesterol synthesis mevalonate pathway [1]. HMG-CoA inhibition results in a reduction of cholesterol synthesis and an increase in the synthesis of low-density-lipoprotein receptors. This, results in increased clearance of LDL cholesterol from the blood stream [2].
HMG-CoA reductase inhibitors are known to have effects beyond their lipid lowering effects, collectively known as pleiotropic effects [3]. These pleiotropic effects result in improvement of endothelial function, modulation of inflammatory responses and antioxidant effects, maintenance of plaque stability, and prevention of thrombus formation [4–6]. The area of pleiotropic effects of statins is promising and several such effects are being speculated.
Statins have also been investigated for their antibacterial action. In one study of the role of statins in community acquired pneumonia, [7] statins were shown to have immunomodulatory, and antioxidative actions, and a significant effect on the concentrations systemic cytokine [8–12]. Several animal studies [9, 13–17] and observational studies in humans [18–22] have shown that individuals treated with statins are less prone to bacterial infection and present better outcomes. The antibacterial and anti-inflammatory effects of statins were investigated in a meta-analysis, which suggested that statin use may be associated with useful outcomes in the treatment and prevention of different infections in recipients of solid-organ transplants [23, 24]. This study aims to further investigate the antibacterial action of statins and identify their spectrum of action.
Methods
Microbial culture and growth conditions
Antibacterial activity of statins was evaluated against different reference bacteria including E. coli ATTC 35218, Pseudomonas aeruginosa ATTC 9027, MSSA ATTC 25213, MRSA ATTC 43300, Streptococcus pneumoniae ATTC 25923, VSE ATTC 19433, VRE ATTC 51299, A. baumannii ATTC 17978, P. mirabilis ATTC 12459, Klebsiella pneumoniae ATTC 13883, Streptococcus pyogenes ATTC 19615, Haemophilus influenzae ATTC 29247, S. epidermidis ATTC 12228, E. aerogenes ATTC 29751, Citrobacter freundii ATTC 8090, E. cloacae ATTC 13047, and against clinical isolates. Eighty clinical isolates were used in this study, comprising 14 different bacterial species. They were obtained from non-duplicate clinical specimens, including ear swab, throat swab, vaginal swab, sputum, urine, and blood culture, from the Microbiology Laboratory at King Abdullah University Hospital (KAUH) in north of Jordan, between April and September of 2010.
The organisms were stored at −70°C in trypticase-soy broth and 20% glycerol (BBL Microbiology Systems, Md, USA). When ready for batch susceptibility testing, samples were thawed. To ensure purity and viability, samples were, then, passed 3 times. Minimum inhibitory concentrations (MICs) were determined in accordance with the Clinical and Laboratory Standards Institute (CLSI) [25].
Determination of minimum inhibitory concentration (MIC)
The MIC was determined by serial dilution method according to the National Committee for Clinical Laboratory Standards [26]. Briefly, statins were serially diluted, and added to plates containing molten BBL Muller-Hinton Gold II agar (BBL Microbiology Systems). Thereafter, plates were slightly cooled and dried. Then, using an a steer replicator, aliquots containing about 5 × 104 colony forming units per drop of different bacterial strains were placed in each plate. After an 18-hour incubation period at 37°C, plates were read. MIC was defined as the lowest concentration at which no growth, a faint haze or fewer than 3 discrete colonies were detected. Plates were read in duplicate, and the highest MIC value was recorded. The breakpoints indicated in the tables of the National Committee for CLSI [26] were used to determine susceptibility and resistance.
Chemicals
Simvastatin atorvastatin and Rosuvastatin were a generous gift from Advanced Pharmaceutical Industries (Amman, Jordan). Drugs (simvastatin, atorvastatin and rosuvastatin) were dissolved in DMSO to a stock concentration of 1 mg/ml, and they were used for MIC determination. All drugs were used as raw materials. DMSO was used to help in dissolving the drugs used. As DMSO is known for possessing no antibacterial activity of its own, DMSO/no statin served as a negative control.
Statistics
Analysis was performed using GraphPad Prism software (version 4.0, GraphPad software, LA jolle, CA). One-way ANOVA followed by Tukey’s post-test were used to determine if there was any statistically significant difference. P-values <0.05 was considered significant.
Results
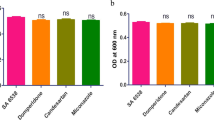
The antibacterial activity of atorvastatin, simvastatin, and rosuvastatin were investigated against 16 standard bacterial strains. Results shown in Table 1 revealed that statins are able to induce variable degrees of antibacterial activity, where atorvastatin and simvastatin are the most potent. MSSA, MRSA, VSE, VRE, A. baumannii, S. epidermidis, and E. aerogenes, were more sensitive to both atorvastatin, and simvastatin compared to rosuvastatin (P < 0-05). On the other hand, E. coli, P. mirabilis, and E. cloacae were more sensitive to atorvastatin compared to both simvastatin and rosuvastatin (P < 0.05).
We next studied the antibacterial activity of statins against 16 clinical isolates of bacteria by measuring MIC values. Most clinical isolates were less sensitive to statins compared to their corresponding standard strains (Table 2). In addition, when compared for their antibacterial activity atorvastatin and simvastatin were significantly more potent compared to Rosuvastatin. For example, P. aeruginosa, MSSA, MRSA, S. pneumonia, VRE, A. baumannii, H. influenza, S. epidermidis, E. aerogenes, C. freundii, and E. cloacae were more sensitive to atorvastatin and simvastatin compared to rosuvastatin (P < 0-05, Table2). Additionally, VSE and VRE isolates were significantly more sensitive to atorvastatin compared to simvastatin (P < 0-05, Table 2).
Discussion
The emergence of drug resistance with patient’s poor compliance, drugs adverse effects and the higher cost of therapy combinations, indicates a strong need for a therapy regimens with similar or higher antibiotics beneficial properties but with better adverse effects profiles. Results of the current study suggest a class effect antibacterial activity for statins, and indicate the superiority of the antibacterial activity of atorvastatin and simvastatin against several standard bacterial strains and clinical isolates as compared to rosuvastatin.
Statins were demonstrated to have pharmacological actions beyond their antihyperlipdimic properties including immunomodulatory, antioxidative and anticoagulant effects. A recent study indicated a direct antimicrobial effect of simvastatin and to a lesser extent fluvastatin against MSSA and MRSA[27]. Another study showed the antibacterial effect of atorvastatin and rosuvastatin in Gram + and Gram– bacteria [28]. Results of the present study extend those of previous studies to include more agents of the statins family and test these agents against a wide range of standard bacterial strains and clinical isolates.
A very recent study has reported MIC values for simvastatin against S. pneumoniae and M. catarrhalis that are similar to the ones reported in this study [29]. These MIC values reflect concentrations of statins that are higher than regular concentrations detected in human blood during statins therapy [30]. However, since multiple dose statins are known for their favorable effect on the course of bacterial infections [18–22], it is possible that statins undergoes accumulation at target human tissues upon multiple dosing, or there could a formation of relevant breakdown products in vivo. Alternatively, statins could aid the action of other antibacterial agent during the treatment of infections in human through their reported pleiotropic actions [31–33].
Statins induce their antihyperlipdimic, via inhibition of HMG-CoA reductase. In bacterial cells, HMG-CoA reductase is essential, where it is required for the biosynthesis of isoprenes [34]. However, bacterial HMG-CoA reductase is of a different structural class with an affinity for statins that is 10 000 times weaker than the enzyme found in eukaryotes [34]. Thus, it is unlikely that antibacterial activity of statins can be attributed to the known mechanism of action (i.e. inhibition of HMG-CoA reductase). Other possible mechanisms could be related to the pleiotropic properties of statins. For example, multiple statins including atorvastatin and simvastatin, were shown to be cytotoxic, to suppress cells growth, and to promote apoptosis [31–33]. It is possible that the currently reported antibacterial activity of statins is related to such effects.
Results of the current study showed the superiority of the antibacterial effcets of atorvastatin or simvastatin to that of rosuvastatin. Previous studies have reported distinct effects, other than the antibacterial activity, for atorvastatin and simvastatin, compared to other members of statins [35, 36]. Additionally, our results show that atrovastatin was superior to simvastatin against VSE and VRE clinical isolates. These distinct effects could also be related to the differences in chemical structure among statins. For example, simvastatin is naturally product of fungal fermentation, whereas atorvastatin is a chemically synthesized derivative. Additionally, satins differ in their lipids affinity, thus, they could have different intrinsic activities. However, these points need more study, and could be a matter of future work.
Conclusion
In summary, results of the current study raise the possibility of a potentially important class effect and future studies are recommended to elucidate mechanism (s) by which atorvastatin and simvastatin are inducing their antibacterial effects.
References
Chatzizisis YS, Koskinas KC, Misirli G, Vaklavas C, Hatzitolios A, Giannoglou GD: Risk factors and drug interactions predisposing to statin-induced myopathy: implications for risk assessment, prevention and treatment. Drug Saf. 2010, 33: 171-187. 10.2165/11319380-000000000-00000
Schneck DW, Knopp RH, Ballantyne CM, McPherson R, Chitra RR, Simonson SG: Comparative effects of rosuvastatin and atorvastatin across their dose ranges in patients with hypercholesterolemia and without active arterial disease. Am J Cardiol. 2003, 91: 33-41.
Kostapanos MS, Milionis HJ, Elisaf MS: An overview of the extra-lipid effects of rosuvastatin. J Cardiovasc Pharmacol Ther. 2008, 13: 157-174. 10.1177/1074248408318628
Nissen SE, Nicholls SJ, Sipahi I, Libby P, Raichlen JS, Ballantyne CM, Davignon J, Erbel R, Fruchart JC, Tardif JC, Schoenhagen P, Crowe T, Cain V, Wolski K, Goormastic M, Tuzcu EM: Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. JAMA. 2006, 295: 1556-1565. 10.1001/jama.295.13.jpc60002
Furberg CD: Natural statins and stroke risk. Circulation. 1999, 99: 185-188. 10.1161/01.CIR.99.2.185
Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ: Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008, 359: 2195-2207. 10.1056/NEJMoa0807646
Viasus D, Garcia-Vidal C, Gudiol F, Carratala J: Statins for community-acquired pneumonia: current state of the science. Eur J Clin Microbiol Infect Dis. 2010, 29: 143-152. 10.1007/s10096-009-0835-0
Bielinska A, Gluszko P: Statins–are they potentially useful in rheumatology?. Pol Arch Med Wewn. 2007, 117: 420-425.
Undas A, Brummel-Ziedins KE, Mann KG: Statins and blood coagulation. Arterioscler Thromb Vasc Biol. 2005, 25: 287-294.
Novack V, Eisinger M, Frenkel A, Terblanche M, Adhikari NK, Douvdevani A, Amichay D, Almog Y: The effects of statin therapy on inflammatory cytokines in patients with bacterial infections: a randomized double-blind placebo controlled clinical trial. Intensive Care Med. 2009, 35: 1255-1260. 10.1007/s00134-009-1429-0
Liao JK, Laufs U: Pleiotropic effects of statins. Annu Rev Pharmacol Toxicol. 2005, 45: 89-118. 10.1146/annurev.pharmtox.45.120403.095748
Terblanche M, Almog Y, Rosenson RS, Smith TS, Hackam DG: Statins and sepsis: multiple modifications at multiple levels. Lancet Infect Dis. 2007, 7: 358-368. 10.1016/S1473-3099(07)70111-1
Merx MW, Liehn EA, Janssens U, Lutticken R, Schrader J, Hanrath P, Weber C: HMG-CoA reductase inhibitor simvastatin profoundly improves survival in a murine model of sepsis. Circulation. 2004, 109: 2560-2565. 10.1161/01.CIR.0000129774.09737.5B
Merx MW, Liehn EA, Graf J, van de Sandt A, Schaltenbrand M, Schrader J, Hanrath P, Weber C: Statin treatment after onset of sepsis in a murine model improves survival. Circulation. 2005, 112: 117-124. 10.1161/CIRCULATIONAHA.104.502195
Chaudhry MZ, Wang JH, Blankson S, Redmond HP: Statin (cerivastatin) protects mice against sepsis-related death via reduced proinflammatory cytokines and enhanced bacterial clearance. Surg Infect (Larchmt). 2008, 9: 183-194. 10.1089/sur.2006.077.
Souza Neto JL, Araujo Filho I, Rego AC, Dominici VA, Azevedo IM, Egito ES, Brandao-Neto J, Medeiros AC: Effects of simvastatin in abdominal sepsis in rats. Acta Cir Bras. 2006, 21 (Suppl 4): 8-12.
Chen CH, Lee RP, Wu WT, Liao KW, Hsu N, Hsu BG: Fluvastatin ameliorates endotoxin induced multiple organ failure in conscious rats. Resuscitation. 2007, 74: 166-174. 10.1016/j.resuscitation.2006.12.002
Hackam DG, Mamdani M, Li P, Redelmeier DA: Statins and sepsis in patients with cardiovascular disease: a population-based cohort analysis. Lancet. 2006, 367: 413-418. 10.1016/S0140-6736(06)68041-0
Almog Y, Shefer A, Novack V, Maimon N, Barski L, Eizinger M, Friger M, Zeller L, Danon A: Prior statin therapy is associated with a decreased rate of severe sepsis. Circulation. 2004, 110: 880-885. 10.1161/01.CIR.0000138932.17956.F1
Liappis AP, Kan VL, Rochester CG, Simon GL: The effect of statins on mortality in patients with bacteremia. Clin Infect Dis. 2001, 33: 1352-1357. 10.1086/323334
Thomsen RW, Hundborg HH, Johnsen SP, Pedersen L, Sorensen HT, Schonheyder HC, Lervang HH: Statin use and mortality within 180 days after bacteremia: a population-based cohort study. Crit Care Med. 2006, 34: 1080-1086. 10.1097/01.CCM.0000207345.92928.E4
Kruger P, Fitzsimmons K, Cook D, Jones M, Nimmo G: Statin therapy is associated with fewer deaths in patients with bacteraemia. Intensive Care Med. 2006, 32: 75-79. 10.1007/s00134-005-2859-y
Sun HY, Singh N: Antimicrobial and immunomodulatory attributes of statins: relevance in solid-organ transplant recipients. Clin Infect Dis. 2009, 48: 745-755. 10.1086/597039
Tleyjeh IM, Kashour T, Hakim FA, Zimmerman VA, Erwin PJ, Sutton AJ, Ibrahim T: Statins for the prevention and treatment of infections: a systematic review and meta-analysis. Arch Intern Med. 2009, 169: 1658-1667. 10.1001/archinternmed.2009.286
Clinical and Laboratory Standards Institute (CLSI): Performance standards for antimicrobial susceptibility testing. M100-S20. 2010, Available from: [http://www.clsi.org/source/orders/free/m100-s20.pdf]. Accessed 14 September 2011. 2010, Villanova, PA, Available from:. Accessed 14 September 2011. 2010
CLSI: Methods for dilution antimicrobial susceptibility test for bacteria that grow aerobically. Approved standard. 2009, Available from [http://www.clsi.org/source/orders/free/m07-a8.pdf]. Accessed 14 September 2011. 2009, Villanova, PA, Eighth, Available from. Accessed 14 September 2011. 2009
Jerwood S, Cohen J: Unexpected antimicrobial effect of statins. J Antimicrob Chemother. 2008, 61: 362-364.
Welsh AM, Kruger P, Faoagali J: Antimicrobial action of atorvastatin and rosuvastatin. Pathology. 2009, 41: 689-691. 10.3109/00313020903305860
Bergman P, Linde C, Putsep K, Pohanka A, Normark S, Henriques-Normark B, Andersson J, Bjorkhem-Bergman L: Studies on the antibacterial effects of statins–in vitro and in vivo. PLoS One. 2011, 6: e24394- 10.1371/journal.pone.0024394
Bjorkhem-Bergman L, Lindh JD, Bergman P: What is a relevant statin concentration in cell experiments claiming pleiotropic effects?. Br J Clin Pharmacol. 2011, 72: 164-165. 10.1111/j.1365-2125.2011.03907.x
Yamazaki H, Suzuki M, Aoki T, Morikawa S, Maejima T, Sato F, Sawanobori K, Kitahara M, Kodama T, Saito Y: Influence of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors on ubiquinone levels in rat skeletal muscle and heart: relationship to cytotoxicity and inhibitory activity for cholesterol synthesis in human skeletal muscle cells. J Atheroscler Thromb. 2006, 13: 295-307. 10.5551/jat.13.295
Muck AO, Seeger H, Wallwiener D: Class-specific pro-apoptotic effect of statins on human vascular endothelial cells. Z Kardiol. 2004, 93: 398-402. 10.1007/s00392-004-0081-5
Tapia-Perez JH, Kirches E, Mawrin C, Firsching R, Schneider T: Cytotoxic effect of different statins and thiazolidinediones on malignant glioma cells. Cancer Chemother Pharmacol. 2011, 67: 1193-1201. 10.1007/s00280-010-1535-2
Friesen JA, Rodwell VW: The 3-hydroxy-3-methylglutaryl coenzyme-A (HMG-CoA) reductases. Genome Biol. 2004, 5: 248- 10.1186/gb-2004-5-11-248
Tesfamariam B, Frohlich BH, Gregg RE: Differential effects of pravastatin, simvastatin, and atorvastatin on Ca2+ release and vascular reactivity. J Cardiovasc Pharmacol. 1999, 34: 95-101. 10.1097/00005344-199907000-00016
Ishikawa M, Okajima F, Inoue N, Motomura K, Kato T, Takahashi A, Oikawa S, Yamada N, Shimano H: Distinct effects of pravastatin, atorvastatin, and simvastatin on insulin secretion from a beta-cell line, MIN6 cells. J Atheroscler Thromb. 2006, 13: 329-335. 10.5551/jat.13.329
Acknowledgment
We would like to acknowledge Jordan University of Science & Technology, Irbid; Jordan, for the financial support (grant number 73–2006 & 226–2009).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
MM carried out MIC determination studies, and participated in drafting the manuscript. NM participated in MIC determination studies, and study design, and helped in drafting the manuscript. KA participated in the design of the study, performed the statistical analysis, and drafted the manuscript. SA conceived of the study, and participated in its design and coordination and helped to draft the manuscript. ZA participated in the design of the study, prepared clinical isolates, and helped to draft the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Masadeh, M., Mhaidat, N., Alzoubi, K. et al. Antibacterial activity of statins: a comparative study of Atorvastatin, Simvastatin, and Rosuvastatin. Ann Clin Microbiol Antimicrob 11, 13 (2012). https://doi.org/10.1186/1476-0711-11-13
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-0711-11-13