
Abstract
Current day concentrations of ambient air pollution have been associated with a range of adverse health effects, particularly mortality and morbidity due to cardiovascular and respiratory diseases. In this review, we summarize the evidence from epidemiological studies on long-term exposure to fine and coarse particles, nitrogen dioxide (NO2) and elemental carbon on mortality from all-causes, cardiovascular disease and respiratory disease. We also summarize the findings on potentially susceptible subgroups across studies. We identified studies through a search in the databases Medline and Scopus and previous reviews until January 2013 and performed a meta-analysis if more than five studies were available for the same exposure metric.
There is a significant number of new studies on long-term air pollution exposure, covering a wider geographic area, including Asia. These recent studies support associations found in previous cohort studies on PM2.5. The pooled effect estimate expressed as excess risk per 10 μg/m3 increase in PM2.5 exposure was 6% (95% CI 4, 8%) for all-cause and 11% (95% CI 5, 16%) for cardiovascular mortality. Long-term exposure to PM2.5 was more associated with mortality from cardiovascular disease (particularly ischemic heart disease) than from non-malignant respiratory diseases (pooled estimate 3% (95% CI −6, 13%)). Significant heterogeneity in PM2.5 effect estimates was found across studies, likely related to differences in particle composition, infiltration of particles indoors, population characteristics and methodological differences in exposure assessment and confounder control. All-cause mortality was significantly associated with elemental carbon (pooled estimate per 1 μg/m3 6% (95% CI 5, 7%)) and NO2 (pooled estimate per 10 μg/m3 5% (95% CI 3, 8%)), both markers of combustion sources. There was little evidence for an association between long term coarse particulate matter exposure and mortality, possibly due to the small number of studies and limitations in exposure assessment. Across studies, there was little evidence for a stronger association among women compared to men. In subjects with lower education and obese subjects a larger effect estimate for mortality related to fine PM was found, though the evidence for differences related to education has been weakened in more recent studies.
Similar content being viewed by others
Review
Background
There is growing evidence of mortality effects related to long-term exposure (i.e., exposures of a year or more) to ambient air pollution [1–3]. Cardiovascular effects of short- and long-term exposure to particulate matter air pollution focusing on PM2.5 have recently been comprehensively reviewed [4, 5]. Experimental and epidemiological studies in the recent decade have significantly increased our knowledge of mechanisms that could plausibly explain the associations observed in epidemiological studies between ambient air pollution and mortality [4].
Most studies have reported associations linked to particulate matter, often represented by the mass concentration of particles smaller than 10 μm (PM10) or 2.5 μm (PM2.5). In many urban areas, motorized traffic emissions are an important source of ambient particles and gaseous pollutants such as nitrogen oxides (NO2 and NO). Exposure contrasts related to traffic emissions are usually poorly represented by the concentration of PM10 or PM2.5, because of the high regional background concentration of these particle metrics from other sources [6, 7]. However, there are more specific markers for traffic related air pollution, which include elemental carbon and ultrafine particles number [7–10]. Janssen and co-workers recently demonstrated that health impact assessments of traffic-related pollutants based upon PM2.5 seriously underestimated the health risks compared to an assessment based upon elemental carbon [7]. There is also growing evidence of health effects related to ultrafine particles [8, 9]. Finally, the effects of coarse particles (the particle fraction between 2.5 and 10 μm) have attracted renewed attention [11]. Emission controls for road traffic have now substantially reduced tailpipe emissions, and therefore non-tailpipe emissions including engine crankcase emissions (combusted lubricating oil), road, tire and brake wear are becoming increasingly important. A recent study in the Netherlands found similar increases of concentrations in major roads compared to urban background for metals related to break and tire wear (Cu, Zn) as for soot and ultrafine particles which are due to tailpipe emissions [10] . In a review of the limited literature, coarse particles were associated with short-term effects on mortality and hospital admissions, but no evidence was found for long-term exposure effects [11]. The number of studies on long-term coarse particle exposure reviewed was small however at the time.
The aim of the current review is to evaluate the epidemiological evidence for cardiovascular and respiratory mortality effects of long-term exposure to fine particulate matter, including a meta-analysis. We focused on epidemiological studies of mortality, as experimental studies and mechanisms of effect have been discussed in detail previously [4]. The American Heart Association review [4] is updated with a significant number of new studies published in 2009 – 2012. We further include more pollutants in the review, specifically NO2, elemental carbon and coarse particles. We evaluated the findings on potentially susceptible subgroups across studies of PM2.5. In addition, we have included the studies on more specific cardiovascular causes of death, especially fatal myocardial infarction and stroke.
Methods
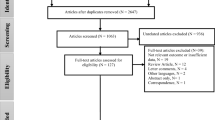
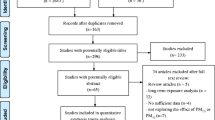
We performed a search in the databases Medline and Scopus with the search terms air pollution, cohort, and mortality until January 2013. We supplemented the search with studies included in the review by Brook and co-worker [4] and by browsing the reference lists of identified papers. In case more than five studies were identified, we performed a meta-analysis. We tested for heterogeneity of cohort-specific effect estimates and obtained combined effects estimates, using random effects methods of DerSimonian and Laird [12]. The I2 statistic was calculated as a measure of the degree of heterogeneity across studies [13]. I2 ranges from 0 to 100% and can be interpreted as the variability of study-specific effect estimates attributable to true between study effects. From some studies multiple papers were available such as the Six Cities study [14–16]. In the meta-analysis we used only the most recent paper, which had longer follow-up. We only included studies in the quantitative meta-analysis that directly provided PM2.5 exposure estimates. For NO2 we only included studies which accounted for intra-urban spatial variation using e.g. dispersion models, land use regression models or spatial interpolation. We used STATA version 10 (Stata Corp, College Station, Texas) for meta-analysis. Effect estimates are presented as excess risks expressed per 10 μg/m3 contrast in exposure, except elemental carbon for which risks were expressed per 1 μg/m3.
PM2.5 and all-cause and cardiovascular mortality
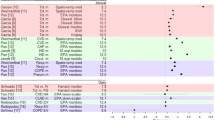
Table 1 and Figures 1 and 2 summarize the studies on long-term air pollution exposure and all-cause and cardiovascular mortality using PM2.5 or PM10 as exposure metric [14–39]. Most but not all studies report significant associations between PM2.5 and all-cause mortality. Since the publication of the authoritative American Heart Association Scientific Statement, sixteen new cohort studies were published between 2009 and January 2013. These studies were often performed in more selected groups e.g. female teachers [27, 36] or male truck drivers [32]. The geographic range has also been expanded significantly with several new studies from Japan and China now published. Another tendency is the publication of large studies based upon large population samples (e.g. census), with often less information on confounding variables such as individual smoking habits. Large cohort studies have used neighborhood socio-economic status and co-morbidities strongly associated with smoking as proxies for actual smoking data [26, 38]. Effect estimates differed substantially across studies, with most studies showing less than 10% increase in mortality for an increment of 10 μg/m3 PM2.5. The random effects summary estimate for the percent excess risk per 10 μg/m3 PM2.5 for all-cause mortality was 6.2% (95% CI: 4.1 – 8.4%). A formal test of heterogeneity was statistically significant, with an I2 value of 65% indicating moderate heterogeneity. I2 can be interpreted as the variability in effect estimates due to true between study variability and not chance [13]. The random effects summary effect estimate for cardiovascular mortality was 10.6% (95% CI 5.4, 16.0%) per 10 μg/m3. Thus, the overall effect estimates were larger for cardiovascular than for all-cause mortality. This pattern was found in most of the individual studies, with the exceptions being the Dutch cohort study [23], the US trucking industry cohort study [32] and a national cohort study from New Zealand [35]. Significant and large heterogeneity of effects was found across studies, with an I2 statistic of 61%. After excluding the Miller study [22], moderate heterogeneity remained (I2 = 40%). Overall, the new studies have supported an association between PM2.5 and mortality first identified in the US Six City and ACS studies. It is of interest to note that the weight of the ACS study in the combined effect estimate is 12% for all-cause mortality, documenting that the combined estimate does not rely on one or two studies. Furthermore, effect estimates from the three large population cohorts without individual smoking data [26, 34, 38] were not higher than those from the individual cohort studies. An important question is what the explanation is for the observed heterogeneity of effect estimates. Differences in study population, exposure assessment, pollution mixture, study period, outcome assessment, and confounder control could have contributed to these differences.

Meta-analysis of the association between PM 2.5 and all-cause mortality (Relative risk per 10 μg/m 3 ). Overall uses random effects.

Meta-analysis of the association between PM 2.5 and cardiovascular mortality (Relative Risk per 10 μg/m 3 ). Overall uses random effects.
Effect modification
Differences in the fraction of susceptible subjects may have contributed to the observed differences. Brook [4] suggested that women might be more susceptible to ambient air pollution. The studies with higher PM effect estimates, particularly the WHI-study have indeed been performed in women only. However, it is problematic to draw conclusions about susceptible subgroups based upon between-study comparisons as multiple factors differ between studies. A comparison of PM effect estimates between men and women within studies does not provide clear evidence that women have a stronger response (Table 2). The findings from the AHSMOG are difficult to interpret, with higher effects in men in the larger earlier study [40] and larger effects in women in the smaller cohort with longer follow-up [41]. The larger effect estimate for BC for men in a Canadian study [30] has to be interpreted with care, because of the lack of data on a variety of important covariates, including individual smoking data, though the authors argue that smoking likely has not confounded the associations with mortality. In the French PAARC study, effect estimates for the evaluated pollutants (TSP, BS and NO2) were similar among men and women [42]. There is also only weak evidence that effect estimates are larger among never-smokers, though in all evaluated studies a (borderline) significant association was found in never-smokers (Table 2). Associations in current smokers were more variable across the studies, consistent with the larger ‘noise’ generated by smoking. In all four studies, PM2.5 effect estimates were higher for those with the lowest education and there was little indication of an association in those with higher education. The absence of an association in the (highly educated) Health professionals study [29] is consistent with this observation. In contrast, in the French PAARC study, effect estimates for Black Smoke were very similar across educational strata, with significant effect also found in those with a university degree [42]. Furthermore the PM2.5 effect estimates (excess risks) in an extended analysis of the ACS differed less than originally reported: 8.2%, 7.2 and 5.5% per 10 μg/m3 for subjects with low, medium and high education respectively [43]. If confirmed in further studies, it is likely that multiple life style related factors may play a role in the stronger effects observed in less-educated subjects. These may include dietary factors such as lower fruit and anti-oxidant intake [23], higher risk of obesity or other pre-existing diseases, higher actual exposures than assumed in the studies, lack of air conditioning and possibly interaction with other risk factors such as poorer housing conditions e.g. moisture.
In two studies, PM2.5 effect estimates were substantially higher among subjects with high body mass index [22, 24].
It is likely that subject characteristics might explain part of the variability of air pollution effect estimates across studies where subgroup analyses are limited by power to detect differences. Hence, further research is required to study the effects of air pollution on women, smokers, obese participants, and diabetes mellitus with better measurement of the exposures. Gene-environment interactions have been shown for the (short-term) air pollution effects on inflammation markers [44, 45] Inflammation likely plays an important role in the mechanism of cardiovascular events [3, 4]. Gene-environment interactions have not yet been studied in the framework of mortality cohort studies.
Exposure issues
One of the important sources of variability of effect estimates between studies is likely related to exposure definition and misclassification. While the most important environmental predictor to consider is actual individual-level exposure to ambient particles, which presumably drives the health effects, most studies have used outdoor concentrations at sites distant to the participant’s precise location. The use of outdoor exposures leads to exposure misclassification. In the cohort studies, exposure has been characterized by the outdoor concentration at the city level based upon central site monitoring or the nearest monitor, or modeling at the individual address. Table 1 shows that the spatial scale of assessment and exposure assessment method varied significantly across studies, probably contributing to differences in effect estimates. Differences in pollution range across studies (Table 1) may have contributed as well. These exposure estimates do not take into account time activity patterns such as time spent in the home or in traffic and factors affecting infiltration of particles indoors. There is a large literature documenting the importance of air exchange rate on infiltration of particles indoors. Importantly, these factors may differ between homes within a study area and between study areas in different climates. In a study of short-term effects, PM10 effects on hospital admissions were larger in US cities with lower% of air conditioning, related to higher particle infiltration rates [46]. The impact of air conditioning use has not been investigated yet in the framework of cohort studies. In the Multiethnic study of Atherosclerosis Air study, indoor-outdoor measurements have been performed to adjust the exposure estimates [47, 48] and each participant provides time-activity information to weight exposures between time spent indoors and outdoors. Evidence for the importance of time activity patterns was obtained in the US truckers study, showing higher ambient PM2.5 effect estimates in the population excluding long-haul drivers who spend more time away from home [32]. Other factors could however also explain the higher effect estimated after excluding long-haul drivers. In the WHI study, effect estimates tended to be higher for subjects spending more than 30 minutes outdoors [22]. In a validation study in the Netherlands, the contrast of personal soot exposure for adults living on a major road compared to those living at a background location, was larger for those spending more time at home [49]. Because of the reliance on ambient exposure estimates, it is not surprising that some heterogeneity in effect estimates across studies is found.
Differences in particle composition or contributing sources very likely explain some of the heterogeneity in effect estimates, as was observed for short-term mortality and hospital admission studies of PM2.5 and PM10[50–53]. For a comprehensive review we refer to the recent evaluation made by the World Health Organization (http://www.euro.who.int/en/what-we-do/health-topics/environment-and-health/air-quality/publications/2013/review-of-evidence-on-health-aspects-of-air-pollution-revihaap). Particle composition effects have not been systematically investigated in cohort studies with the exception of the California teacher’s study [27]. In a recent review it was shown that on a per microgram per m3 basis, mortality effect estimates were about 10 times larger for EC than for PM2.5[7]. Hence, in locations with higher levels of primary combustion particles we could expect higher PM2.5 effects. In the next section, evidence on EC is further discussed.
A further important issue is for which period exposure is characterized. Air pollution data may not be available for the entire follow-up period. As an example in the ACS study, PM2.5 data were available at the start and end of follow-up [18]. When significant (often downward) trends in pollution occur with changing (often decreasing) spatial contrasts in the study, bias may occur in the estimated association between pollution and mortality. The follow-up study from the Harvard Six City study [14] and two studies in potentially at-risk populations [54, 55] suggested that the relevant exposure for cardiovascular effects may be the exposure in the past few years. These authors conclude that it does not take decades to bridge the gap between the short- and long-term exposure effect estimates, consistent with the effect of intervention studies showing reductions in mortality in the year after the intervention [54, 55]. These studies [54, 55] have made use of long-term temporal contrast within cities adjusting for secular trends. PM effect estimates were similar to the previously discussed studies exploiting spatial contrasts.
A further temporal issue in studies that use land use regression models for exposure assessment is that these models often are based upon current measurement campaigns and linked to health outcomes that occurred in the past. Three studies in the Netherlands, Rome (Italy) and Vancouver (Canada) have shown that for periods of about 10 years current LUR models predicted historic spatial contrasts well [56–58]. Even when concentrations have decreased over time, spatial contrasts often remain stable. Spatial contrasts may not be stable in areas with rapid economic development as indicated in one of the Chinese cohort studies in which the ranking of study areas changed during follow-up [33, 59]. Even when the ranking of subjects is not changed, the quantitative spatial contrast in a study area may have changed, e.g. because the difference between major roads and background locations has decreased in time. Changed spatial contrasts will affect the estimated slope of the mortality pollution association [18, 56]. Moving of subjects may further complicate the assessment.
An important question to address for the traffic pollution studies is potential confounding by road traffic noise, which has been shown to be related to cardiovascular disease including MI as well. A few studies have attempted to disentangle traffic-related air pollution and noise [60–62]. These studies found moderate correlations between air pollution and noise. The three studies differed somewhat in their findings of independent air pollution and noise effects. More work is needed in this area.
Coarse particles and elemental carbon
Table 3 presents studies that have used elemental carbon or coarse PM as the exposure metric. Table 3 illustrates that there is no evidence that long-term exposure to coarse PM is related to mortality. In three of the four cohort studies that reported no significant association with coarse PM, significant associations with PM2.5 were found [18, 25, 63]. However, exposure assessment for coarse particles is more challenging than for PM2.5 because of the influence of local sources, hence central site monitors are likely to have greater errors in representing residential concentrations. It is therefore possible that with more spatially resolved exposure assessment methods such as land use regression models or dispersion models, potential long-term exposure effects will be detected. The California Teacher’s study did not evaluate coarse PM and did not find significant associations between all-cause mortality and elemental concentrations of Si, Fe and Zn, elements abundant in coarse particles, but did report an association between Si and ischemic heart disease [27].
Consistently, the summary estimate for PM10 was smaller than for PM2.5 with a summary effect estimate per 10 μg/m3 of 3.5% (95% CI 0.4%, 6.6%) with significant heterogeneity (I2 = 69%) of the studies included in Table 1, excluding the because of changing spatial patterns difficult to interpret Chinese retrospective study [33]. The PM10 analysis was added as several studies only report PM10.
Effect estimates for EC were very consistent across studies [23, 27, 30, 42, 64–67]. The random effects summary estimate for all-cause mortality per 1 μg/m3 EC was 6.1% (95% CI 4.9%, 7.3%), with highly non-significant heterogeneity of effect estimates (I2 = 0%). Most of the included studies assessed EC exposure at the city-scale [27, 64] which represents variation in city background but does not account for small-scale variation related to proximity to major roads. Many studies have documented significant intra-urban contrasts for EC, related to especially major roads [7]. Most likely EC and NO2 should be considered representatives of the complex mixture of traffic-related air pollution, rather than the only components causally associated with mortality.
There is fairly consistent evidence of associations of mortality with nitrogen dioxide (Table 4). The random effects summary estimate for all-cause mortality per 10 μg/m3 for NO2 was 5.5% (95% CI 3.1%, 8.0%), with significant and large heterogeneity of effect estimates (I2 = 73%). In this analysis, the Chinese study [33] was not included as exposure was assessed at the district level. Inclusion of the essentially null findings of the ACS study-excess risk of 0.3% (95% CI −0.8, 1.3%)- resulted in an only slightly smaller combined estimate of 4.7% (95% CI 2.4, 7.1%). In the ACS study, intra-urban variation was also not accounted for. As traffic-related air pollution varies on a small spatial scale, it is even more critical to assess exposure on a fine spatial scale such as the residential address than for PM2.5.
Specific cardiovascular causes of death
Table 5 shows associations between ambient air pollution and mortality from ischemic heart disease or myocardial infarction (MI), including studies based upon death certificates, more detailed studies using registry data, or ideally cohort studies with epidemiological review of medical records, allowing more precise identification of disease incidence. Several case–control studies based upon M.I. registries or epidemiological studies with clinical review have found associations between NO2 and fatal M.I. but not non-fatal M.I. [72–74]. Thus far, the finding of associations for fatal MI only was interpreted as an evidence that air pollution particularly affects the frail, or acts to aggravate a disease progression caused by other factors. On the other hand, it is also possible that the outcomes of ischemic heart diseases are misclassified and combined as composite outcomes, where fatal outcomes are captured more precisely [75]. Although there is increasing evidence that air pollution is associated with markers of early atherosclerosis, it is possible that air pollution will affect the underlying biological processes that predispose to atherothrombosis (which leads to MI and stroke) compared to atherosclerosis [76, 77]. Another explanation is that the type of outcomes affected by pollution are those that have higher case-fatality rates (e.g., arrhythmic sudden death has higher case-fatality rate than overall MI).
Fewer studies have evaluated cerebrovascular mortality. In the Dutch cohort study and in the Women’s Health Initiative Study, a strong association was found [22, 23]. In contrast, in the ACS study, the Norwegian cohort, and the Swiss national cohort study no association was found [28, 39, 68]. It is possible that poorer recording of cerebrovascular mortality on death certificates has contributed to these inconsistencies. There is also some evidence from ecological studies that air pollution may contribute to stroke mortality [78, 79].
Two studies have reported significant associations between particulate matter air pollution and dysrhythmia, heart failure and cardiac arrest combined [39, 60]. These results are based upon smaller numbers of events, and require large cohort studies for further verification. The results are consistent with several studies documenting significant associations between short-term PM or NO2 exposure and mortality due to heart failure and dysrhythmia and defibrillator discharges [4, 80].
Air pollution and respiratory mortality
Table 6 shows the effect estimates for respiratory mortality. In the two first US cohort studies, no association between PM2.5 and respiratory mortality was found [15, 17]. In contrast to the findings of these US studies, strong associations were found in the Dutch cohort study [23], a Norwegian study [68] and a Chinese study [59]. The random effect pooled estimate per 10 μg/m3 for PM2.5 was 2.9% (95%CI −5.9, 12.6%), highly non-significant. The heterogeneity across studies was statistically significant with an I2 statistic of 59%, indicating moderate heterogeneity. Associations for PM were weaker in the Dutch and Chinese cohort study than with NO2 or NOx. Respiratory mortality may be more related to primary traffic-related pollutants than with long-range transported particles, though further work is needed to test this hypothesis. The smaller number of deaths due to respiratory disease compared to cardiovascular diseases, contributed to larger confidence intervals within individual studies and larger variability of the main effect estimates across studies. In time series studies including several large multi-city studies in the USA and Europe, significant associations between daily variations in PM and respiratory mortality were found [1–4]. Expressed per 10 μg/m3 PM excess risks of about 1% are typically reported for short-term exposures, larger than for all-cause mortality [1–4]. In contrast to cardiovascular disease, current evidence therefore does not suggest an additional risk from long-term exposure, possibly related to mortality displacement [2, 3]. More studies are needed to evaluate long-term exposures on respiratory mortality more thoroughly.
Conclusions
There is a significant number of new studies on long-term air pollution exposure, covering a wider geographic area, including Asia. These recent studies support associations found in previous cohort studies on PM2.5. The pooled effect estimate expressed as excess risk per 10 μg/m3 increase in PM2.5 exposure was 6% (95% CI 4, 8%) for all-cause and 11% (95% 5, 16%) for cardiovascular mortality. Long-term exposure to PM2.5 was more associated with mortality from cardiovascular disease (particularly ischemic heart disease) than from non-malignant respiratory diseases (pooled estimate 3% (95% CI −6, 13%)). Significant heterogeneity in PM2.5 effect estimates was found across studies, likely related to differences in particle composition, infiltration of particles indoors, population characteristics and methodological differences in exposure assessment and confounder control. All-cause mortality was significantly associated with elemental carbon (pooled estimate per 1 μg/m3 6% (95% CI 5, 7%)) and NO2 (pooled estimate per 10 μg/m3 5% (95% CI 3, 8%)), both markers of combustion sources. There was little evidence for an association between long term coarse particulate matter exposure and mortality, possibly due to the small number of studies and limitations in exposure assessment. Across studies, there was little evidence for stronger association among women compared to men. Subjects with lower education and obese subjects experienced larger mortality effect related to fine PM, though the evidence for differences related to education has been weakened in more recent studies.
Our review suggests several specific research questions. Research into the reasons for the heterogeneity of effect estimates would be extremely useful for health impact assessment. Better exposure assessment including spatially resolved outdoor exposures and more chemically speciated PM might in part be able to resolve the observed heterogeneity. Chemical speciation would allow assessing particles from different sources e.g. particles from combustion sources and non-tailpipe emissions separately, a question clearly relevant for air pollution control policy. Specific attention to motorized traffic emissions is important because (road) traffic is an important source of ambient air pollution. More work on coarse particles and at the other side of the particle size spectrum, ultrafine particles is needed. Ongoing new research in the USA in the Multi-Ethnic study of Atherosclerosis and Air pollution (MESA-AIR) and the European Study of Cohorts for Air Pollution Effects (ESCAPE) that use large cohorts and state-of the art spatially-resolved exposure methods will likely contribute significant new answers in the near future to these questions.
Abbreviations
- ACS:
-
American Cancer Society study
- BS:
-
Black Smoke
- BC:
-
Black Carbon
- CI:
-
Confidence interval
- EC:
-
Elemental Carbon
- NO2:
-
Nitrogen dioxide
- NOx:
-
Nitrogen oxides
- PM:
-
Particulate matter
- PM2.5:
-
Particles smaller than 2.5 μm
- PM10:
-
Particles smaller than 10 μm
- TSP:
-
Total suspended particles.
References
World Health Organization: Systematic review of air pollution, a global update. 2006
Pope CA, Dockery DW: Health effects of fine particulate air pollution: lines that connect. J Air Waste Manag Assoc. 2006, 56: 709-742. 10.1080/10473289.2006.10464485.
Brunekreef B, Holgate ST: Air pollution and health. Lancet. 2002, 360: 1233-1242. 10.1016/S0140-6736(02)11274-8.
Brook RD, Rajagopalan S, Pope CA, Brook JR, Bhatnagar A, Diez-Roux AV, Holguin F, Hong Y, Luepker RV, Mittleman MA, Peters A, Siscovick D, Smith SC, Whitsel L, Kaufman JD: Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American heart association. Circulation. 2010, 121: 2331-2378. 10.1161/CIR.0b013e3181dbece1.
Krishnan RM, Kaufman JD, Hoek G: Chronic effects of air pollution on cardiovascular health. Cardiovascular effects of inhaled ultrafine and nanosized particles. Edited by: Cassee FR, Mills NL, Newby D. 2011, Hoboken, New Jersey: John Wiley & Sons, Inc
HEI panel: HEI Special report 17. Traffic-related air pollution. A critical review of the literature on emissions, exposure and health effects. 2010, Boston, MA: Health Effects Institute
Janssen NA, Hoek G, Simic-Lawson M, Fischer P, van Bree L, ten Brink H, Keuken M, Atkinson RW, Anderson HR, Brunekreef B, Cassee FR: Black carbon as an additional indicator of the adverse effects of airborne particles compared with PM10 and PM2.5. Environ Health Perspect. 2011, 119: 1691-1699. 10.1289/ehp.1003369.
Peters A, Rückerl R, Cyrys J: Lessons from air pollution epidemiology for studies of engineered nanomaterials. J Occup Environ Med. 2011, 53 (6 SUPPL): S8-S13.
Rückerl R, Schneider A, Breitner S, Cyrys J, Peters A: Health effects of particulate air pollution: a review of epidemiological evidence. Inhal Toxicol. 2011, 23: 555-592. 10.3109/08958378.2011.593587.
Boogaard H, Kos GPA, Weijers EP, Janssen NAH, Fischer PH, van der Zee SC, de Hartog JJ, Hoek G: Contrast in air pollution components between major streets and background locations: particulate matter mass, black carbon, elemental composition, nitrogen oxide and ultrafine particle number. Atmos Environ. 2011, 45: 650-658. 10.1016/j.atmosenv.2010.10.033.
Brunekreef B, Forsberg B: Epidemiological evidence of effects of coarse airborne particles on health. Eur Respir J. 2005, 26: 309-318. 10.1183/09031936.05.00001805.
DerSimonian R, Laird N: Meta-analysis in clinical trials. Control Clin Trials. 177, 7: 177-188.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG: Measuring inconsistency in meta-analyses. Br Med J. 2003, 327: 557-560. 10.1136/bmj.327.7414.557.
Laden F, Schwartz J, Speizer FE, Dockery DW: Reduction in fine particulate Air pollution and mortality: extended follow-up of the Harvard Six cities study. Am J Respir Crit Care Med. 2006, 173: 667-672. 10.1164/rccm.200503-443OC.
Dockery DW, Pope CA, Xu X, Spengler JD, Ware JH, Fay ME, Ferris BG, Speizer FE: An association between air pollution and mortality in six U.S. cities. N Engl J Med. 1993, 329: 1753-1759. 10.1056/NEJM199312093292401.
Lepeule J, Laden F, Dockery D, Schwartz J: Chronic exposure to fine particles and mortality: an extended follow-up of the Harvard six cities study from 1974 to 2009. Environ Health Perspect. 2012, 120: 965-970. 10.1289/ehp.1104660.
Pope CA, Thun MJ, Namboodiri MM, Dockery DW, Evans JS, Speizer FE, Jr HC: Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am J Respir Crit Care Med. 1995, 151: 669-674. 10.1164/ajrccm/151.3_Pt_1.669.
Pope CA, Thun MJ, Calle EE, Krewski D, Ito K, Thurston GD: Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA. 2002, 287: 1132-1141. 10.1001/jama.287.9.1132.
Jerrett M, Burnett RT, Ma R, Pope CA, Krewski D, Newbold KB, Thurston G, Shi Y, Finkelstein N, Calle EE, Thun MJ: Spatial analysis of air pollution and mortality in Los Angeles. Epidemiology. 2005, 16: 727-736. 10.1097/01.ede.0000181630.15826.7d.
Gehring U, Heinrich J, Kramer U, Grote V, Hochadel M, Sugiri D, Kraft M, Rauchfuss K, Eberwein HG, Wichmann HE: Long-term exposure to ambient air pollution and cardiopulmonary mortality in women. Epidemiology. 2006, 17: 545-551. 10.1097/01.ede.0000224541.38258.87.
Heinrich J, Thiering E, Rzehak P, Krämer U, Hochadel M, Rauchfuss KM, Gehring U, Wichmann H: Long-term exposure to NO2 and PM10 and all-cause and cause-specific mortality in a prospective cohort of women. Occup Environ Med. 2013, 70: 179-186. 10.1136/oemed-2012-100876.
Miller KA, Siscovick DS, Sheppard L, Shepherd K, Sullivan JH, Anderson GL, Kaufman JD: Long-term exposure to air pollution and incidence of cardiovascular events in women. N Engl J Med. 2007, 356: 447-458. 10.1056/NEJMoa054409.
Beelen R, Hoek G, van den Brandt PA, Goldbohm RA, Fischer P, Schouten LJ, Jerrett M, Hughes E, Armstrong B, Brunekreef B: Long-term effects of traffic-related air pollution on mortality in a Dutch cohort (NLCS-AIR study). Environ Health Perspect. 2008, 116: 196-202. 10.1289/ehp.10614.
Puett RC, Schwartz J, Hart JE, Yanosky JD, Speizer FE, Suh H, Paciorek CJ, Neas LM, Laden F: Chronic particulate exposure, mortality, and coronary heart disease in the Nurses’ Health Study. Am J Epidemiol. 2008, 168: 1161-1168. 10.1093/aje/kwn232.
Puett RC, Hart JE, Yanosky JD, Paciorek C, Schwartz J, Suh H, Speizer FE, Laden F: Chronic fine and coarse particulate exposure, mortality, and coronary heart disease in the Nurses’ Health Study. Environ Health Perspect. 2009, 117: 1697-1701. 10.1289/ehp.0900572.
Zeger SL, Dominici F, McDermott A, Samet JM: Mortality in the Medicare population and chronic exposure to fine particulate air pollution in urban centers (2000–2005). Environ Health Perspect. 2008, 116: 1614-1619. 10.1289/ehp.11449.
Ostro B, Lipsett M, Reynolds P, Goldberg D, Hertz A, Garcia C, Henderson KD, Bernstein L: Long-term exposure to constituents of fine particulate air pollution and mortality: results from the California teachers study. Environ Health Perspect. 2010, 118: 363-369.
Huss A, Spoerri A, Egger M, Röösli M: Aircraft noise, air pollution, and mortality from myocardial infarction. Epidemiology. 2010, 21: 829-836. 10.1097/EDE.0b013e3181f4e634.
Puett RC, Hart JE, Suh H, Mittleman M, Laden F: Particulate matter exposures, mortality, and cardiovascular disease in the health professionals follow-up study. Environ Health Perspect. 2011, 119: 1130-1135. 10.1289/ehp.1002921.
Gan WQ, Koehoorn M, Davies HW, Demers PA, Tamburic L, Brauer M: Long-term exposure to traffic-related air pollution and the risk of coronary heart disease hospitalization and mortality. Environ Health Perspect. 2011, 119: 501-507.
Cao J, Yang C, Li J, Chen R, Chen B, Gu D, Kan H: Association between long-term exposure to outdoor air pollution and mortality in China: a cohort study. J Hazard Mater. 2011, 186: 1594-1600. 10.1016/j.jhazmat.2010.12.036.
Hart JE, Garshick E, Dockery DW, Smith TJ, Ryan L, Laden F: Long-term ambient multipollutant exposures and mortality. Am J Respir Crit Care Med. 2011, 183: 73-78. 10.1164/rccm.200912-1903OC.
Zhang P, Dong G, Sun B, Zhang L, Chen X, Ma N, Yu F, Guo H, Huang H, Lee YL, Tang N, Chen J: Long-term exposure to ambient air pollution and mortality due to cardiovascular disease and cerebrovascular disease in Shenyang, China. PLoS One. 2011, 6: e20827-10.1371/journal.pone.0020827.
Crouse DL, Peters PA, van Donkelaar A, Goldberg MS, Villeneuve PJ, Brion O, Khan S, Atari DO, Jerrett M, Pope CA, Brauer M, Brook JR, Martin RV, Stieb D, Burnett RT: Risk of nonaccidental and cardiovascular mortality in relation to long-term exposure to low concentrations of fine particulate matter: a Canadian national-level cohort study. Environ Health Perspect. 2012, 120: 708-714. 10.1289/ehp.1104049.
Hales S, Blakely T, Woodward A: Air pollution and mortality in New Zealand: cohort study. J Epidemiol Community Health. 2012, 66: 468-473. 10.1136/jech.2010.112490.
Lipsett MJ, Ostro BD, Reynolds P, Goldberg D, Hertz A, Jerrett M, Smith DF, Garcia C, Chang ET, Bernstein L: Long-term exposure to air pollution and cardiorespiratory disease in the California teachers study cohort. Am J Respir Crit Care Med. 2011, 184: 828-835. 10.1164/rccm.201012-2082OC.
Ueda K, Nagasawa SY, Nitta H, Miura K, Ueshima H, NIPPON DATA80 Research Group: Exposure to particulate matter and long-term risk of cardiovascular mortality in Japan: NIPPON DATA80. J Atheroscler Thromb. 2012, 19: 246-254. 10.5551/jat.9506.
Cesaroni G, Badaloni C, Gariazzo C, Stafoggia M, Sozzi R, Davoli M, Forastiere F: Long-term exposure to urban air pollution and mortality in a cohort of more than a million adults in Rome. Environ Health Perspect. 2013, 121: 324-331. 10.1289/ehp.1205862.
Pope CA, Burnett RT, Thurston GD, Thun MJ, Calle EE, Krewski D, Godleski JJ: Cardiovascular mortality and long-term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways of disease. Circulation. 2004, 109: 71-77.
Abbey DE, Nishino N, McDonnell WF, Burchette RJ, Knutsen SF, Lawrence BW, Yang JX: Long-term inhalable particles and other air pollutants related to mortality in nonsmokers. Am J Respir Crit Care Med. 1999, 159: 373-382. 10.1164/ajrccm.159.2.9806020.
Chen LH, Knutsen SF, Shavlik D, Beeson WL, Petersen F, Ghamsary M, Abbey D: The association between fatal coronary heart disease and ambient particulate air pollution: Are females at greater risk?. Environ Health Perspect. 2005, 113: 1723-1729. 10.1289/ehp.8190.
Filleul L, Rondeau V, Vandentorren S, Le Moual N, Cantagrel A, Annesi-Maesano I, Charpin D, Declercq C, Neukirch F, Paris C, Vervloet D, Brochard P, Tessier JF, Kauffmann F, Baldi I: Twenty five year mortality and air pollution: results from the French PAARC survey. Occup Environ Med. 2005, 62: 453-460. 10.1136/oem.2004.014746.
Krewski D, Jerrett M, Burnett RT, Ma R, Hughes E, Shi Y, Turner MC, Pope CA, Thurston G, Calle EE, Thun MJ, Beckerman B, DeLuca P, Finkelstein N, Ito K, Moore DK, Newbold KB, Ramsay T, Ross Z, Shin H, Tempalski B: Extended follow-up and spatial analysis of the American cancer society study linking particulate air pollution and mortality. Res Rep Health Eff Inst. 2009, 140: 5-114. discussion 115–36
Ljungman P, Bellander T, Schneider A, Breitner S, Forastiera F, Hampel R, Illig T, Jacquemin B, Katsouyanni K, von Klot S, Koenig W, Lanki T, Nyberg F, Pekkanen J, Pistelli R, Pitsavos C, Rosenqvist M, Sunyer J, Peters A: Modification of the interleukin-6 response to air pollution by interleukin-6 and fibrinogen polymorphisms. Environ Health Perspect. 2009, 117: 1373-1379.
Peters A, Greven S, Heid IM, Baldari F, Breitner S, Bellander T, Chrysohoou C, Illig T, Jacquemin B, Koenig W, Lanki T, Nyberg F, Pekkanen J, Pistelli R, Rückerl R, Stefanadis C, Schneider A, Sunyer J, Wichmann HE: Fibrinogen genes modify the fibrinogen response to ambient particulate matter. Am J Respir Crit Care Med. 2009, 179: 484-491. 10.1164/rccm.200805-751OC.
Janssen NA, Schwartz J, Zanobetti A, Suh HH: Air conditioning and source-specific particles as modifiers of the effect of PM(10) on hospital admissions for heart and lung disease. Environ Health Perspect. 2002, 110: 43-49. 10.1289/ehp.02110s143.
Mercer LD, Szpiro AA, Sheppard L, Lindström J, Adar SD, Allen RW, Avol EL, Oron AP, Larson T, Liu L-S, Kaufman JD: Comparing universal kriging and land-use regression for predicting concentrations of gaseous oxides of nitrogen (NOx) for the Multi-Ethnic Study of Atherosclerosis and Air Pollution (MESA Air). Atmos Environ. 2011, 45: 4412-4420. 10.1016/j.atmosenv.2011.05.043.
Cohen MA, Adar SD, Allen RW, Avol E, Curl CL, Gould T, Hardie D, Ho A, Kinney P, Larson TV, Sampson P, Sheppard L, Stukovsky KD, Swan SS, Liu L-S, Kaufman JD: Approach to estimating participant pollutant exposures in the Multi-Ethnic Study of Atherosclerosis and Air Pollution (MESA Air). Environ Sci Technol. 2009, 43: 4687-4693. 10.1021/es8030837.
Van Roosbroeck S, Hoek G, Meliefste K, Janssen NA, Brunekreef B: Validity of residential traffic intensity as an estimate of long-term personal exposure to traffic-related air pollution among adults. Environ Sci Technol. 2008, 42: 1337-1344. 10.1021/es0712827.
Katsouyanni K, Touloumi G, Samoli E, Gryparis A, Le Tertre A, Monopolis Y, Rossi G, Zmirou D, Ballester F, Boumghar A, Anderson HR, Wojtyniak B, Paldy A, Braunstein R, Pekkanen J, Schindler C, Schwartz J: Confounding and effect modification in the short-term effects of ambient particles on total mortality: results from 29 European cities within the APHEA2 project. Epidemiology. 2001, 12: 521-531. 10.1097/00001648-200109000-00011.
Laden F, Neas LM, Dockery DW, Schwartz J: Association of fine particulate matter from different sources with daily mortality in six U.S. cities. Environ Health Perspect. 2000, 108: 941-947. 10.1289/ehp.00108941.
Lanki T, de Hartog JJ, Heinrich J, Hoek G, Janssen NA, Peters A, Stolzel M, Timonen KL, Vallius M, Vanninen E, Pekkanen J: Can we identify sources of fine particles responsible for exercise-induced ischemia on days with elevated air pollution? The ULTRA study. Environ Health Perspect. 2006, 114: 655-660. 10.1289/ehp.8578.
Bell ML, Ebisu K, Peng RD, Samet JM, Dominici F: Hospital admissions and chemical composition of fine particle air pollution. Am J Respir Crit Care Med. 2009, 179: 1115-1120. 10.1164/rccm.200808-1240OC.
Zanobetti A, Bind MA, Schwartz J: Particulate air pollution and survival in a COPD cohort. Environ Health. 2008, 7: 48-10.1186/1476-069X-7-48.
Zanobetti A, Schwartz J: Particulate air pollution, progression, and survival after myocardial infarction. Environ Health Perspect. 2007, 115: 769-775. 10.1289/ehp.9201.
Cesaroni G, Porta D, Badaloni C, Stafoggia M, Eeftens M, Meliefste K, Forastiere F: Nitrogen dioxide levels estimated from land use regression models several years apart and association with mortality in a large cohort study. Environ Health. 2012, 11: 48-10.1186/1476-069X-11-48.
Eeftens M, Beelen R, Fischer P, Brunekreef B, Meliefste K, Hoek G: Stability of measured and modelled spatial contrasts in NO2 over time. Occup Environ Med. 2011, 68: 765-770. 10.1136/oem.2010.061135.
Wang R, Henderson SB, Sbihi H, Allen RW, Brauer M: Temporal stability of land use regression models for traffic-related air pollution. Atmos Environ. 2013, 64: 312-319.
Dong GH, Zhang P, Sun B, Zhang L, Chen X, Ma N, Yu F, Guo H, Huang H, Lee YL, Tang N, Chen J: Long-term exposure to ambient air pollution and respiratory disease mortality in Shenyang, China: a 12-year population-based retrospective cohort study. Respiration. 2012, 84: 360-368. 10.1159/000332930.
Beelen R, Hoek G, Houthuijs D, van den Brandt PA, Goldbohm RA, Fischer P, Schouten LJ, Armstrong B, Brunekreef B: The joint association of air pollution and noise from road traffic with cardiovascular mortality in a cohort study. Occup Environ Med. 2009, 66: 243-250.
Selander J, Nilsson ME, Bluhm G, Rosenlund M, Lindqvist M, Nise G, Pershagen G: Long-term exposure to road traffic noise and myocardial infarction. Epidemiology. 2009, 20: 272-279. 10.1097/EDE.0b013e31819463bd.
Gan WQ, Davies HW, Koehoorn M, Brauer M: Association of long-term exposure to community noise and traffic-related air pollution with coronary heart disease mortality. Am J Epidemiol. 2012, 175: 898-906. 10.1093/aje/kwr424.
McDonnell WF, Nishino-Ishikawa N, Petersen FF, Chen LH, Abbey DE: Relationships of mortality with the fine and coarse fractions of long-term ambient PM10 concentrations in nonsmokers. J Expo Anal Environ Epidemiol. 2000, 10: 427-436. 10.1038/sj.jea.7500095.
Smith KR, Jerrett M, Anderson HR, Burnett RT, Stone V, Derwent R, Atkinson RW, Cohen A, Shonkoff SB, Krewski D, Pope CA, Thun MJ, Thurston G: Public health benefits of strategies to reduce greenhouse-gas emissions: health implications of short-lived greenhouse pollutants. Lancet. 2009, 374: 2091-2103. 10.1016/S0140-6736(09)61716-5.
von Klot S, Gryparis A, Tonne C, Yanosky J, Coull BA, Goldberg RJ, Lessard D, Melly SJ, Suh HH, Schwartz J: Elemental carbon exposure at residence and survival after acute myocardial infarction. Epidemiology. 2009, 20: 547-554. 10.1097/EDE.0b013e31819d9501.
Lipfert F, Wyzga R, Baty J, Miller J: Traffic density as a surrogate measure of environmental exposures in studies of air pollution health effects: long-term mortality in a cohort of US veterans. Atmos Environ. 2006, 40: 154-169. 10.1016/j.atmosenv.2005.09.027.
Beverland IJ, Cohen GR, Heal MR, Carder M, Yap C, Robertson C, Hart CL, Agius RM: A comparison of short-term and long-term air pollution exposure associations with mortality in two cohorts in Scotland. Environ Health Perspect. 2012, 120: 1280-1285. 10.1289/ehp.1104509.
Nafstad P, Haheim LL, Wisloff T, Gram F, Oftedal B, Holme I, Hjermann I, Leren P: Urban air pollution and mortality in a cohort of Norwegian men. Environ Health Perspect. 2004, 112: 610-615. 10.1289/ehp.6684.
Raaschou-Nielsen O, Andersen ZJ, Jensen SS, Ketzel M, Sorensen M, Hansen J, Loft S, Tjonneland A, Overvad K: Traffic air pollution and mortality from cardiovascular disease and all causes: a Danish cohort study. Environ Health. 2012, 11: 60-10.1186/1476-069X-11-60.
Yorifuji T, Kashima S, Tsuda T, Takao S, Suzuki E, Doi H, Sugiyama M, Ishikawa-Takata K, Ohta T: Long-term exposure to traffic-related air pollution and mortality in Shizuoka, Japan. Occup Environ Med. 2010, 67: 111-117. 10.1136/oem.2008.045542.
Chen H, Goldberg MS, Burnett RT, Jerrett M, Wheeler AJ, Villeneuve PJ: Long-term exposure to traffic-related air pollution and cardiovascular mortality. Epidemiology. 2013, 24: 35-43. 10.1097/EDE.0b013e318276c005.
Rosenlund M, Berglind N, Pershagen G, Hallqvist J, Jonson T, Bellander T: Long-term exposure to urban air pollution and myocardial infarction. Epidemiology. 2006, 17: 383-390. 10.1097/01.ede.0000219722.25569.0f.
Rosenlund M, Picciotto S, Forastiere F, Stafoggia M, Perucci CA: Traffic-related air pollution in relation to incidence and prognosis of coronary heart disease. Epidemiology. 2008, 19: 121-128. 10.1097/EDE.0b013e31815c1921.
Rosenlund M, Bellander T, Nordquist T, Alfredsson L: Traffic-generated air pollution and myocardial infarction. Epidemiology. 2009, 20: 265-271. 10.1097/EDE.0b013e318190ea68.
Heckbert SR, Kooperberg C, Safford MM, Psaty BM, Hsia J, McTiernan A, Gaziano JM, Frishman WH, Curb JD: Comparison of self-report, hospital discharge codes, and adjudication of cardiovascular events in the Women’s Health Initiative. Am J Epidemiol. 2004, 160: 1152-1158. 10.1093/aje/kwh314.
Mills NL, Donaldson K, Hadoke PW, Boon NA, MacNee W, Cassee FR, Sandstrom T, Blomberg A, Newby DE: Adverse cardiovascular effects of air pollution. Nat Clin Pract Cardiovasc Med. 2009, 6: 36-44. 10.1038/ncpcardio1399.
Kunzli N, Jerrett M, Mack WJ, Beckerman B, LaBree L, Gilliland F, Thomas D, Peters J, Hodis HN: Ambient air pollution and atherosclerosis in Los Angeles. Environ Health Perspect. 2005, 113: 201-206.
Maheswaran R, Elliott P: Stroke mortality associated with living near main roads in England and Wales: a geographical study. Stroke. 2003, 34: 2776-2780. 10.1161/01.STR.0000101750.77547.11.
Maheswaran R, Haining RP, Pearson T, Law J, Brindley P, Best NG: Outdoor NOx and stroke mortality: adjusting for small area level smoking prevalence using a Bayesian approach. Stat Methods Med Res. 2006, 15: 499-516.
Ljungman PL, Berglind N, Holmgren C, Gadler F, Edvardsson N, Pershagen G, Rosenqvist M, Sjögren B, Bellander T: Rapid effects of air pollution on ventricular arrhythmias. Eur Heart J. 2008, 29: 2894-2901. 10.1093/eurheartj/ehn463.
Acknowledgments
The paper has been prepared in the framework of the projects ESCAPE and TRANSPHORM. The research leading to these results has received funding from the European Community’s Seventh Framework Program (FP7/2007-2011) under grant agreement number: 211250.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None of the authors has a competing interest.
Authors’ contributions
GH, RMK, RB, AP, BO, BB and JK have contributed to the definition of the scope of the review, identification of studies and interpretation of results. GH drafted the text. GH, RMK, RB, AP, BO, BB and JK provided critical comments and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Hoek, G., Krishnan, R.M., Beelen, R. et al. Long-term air pollution exposure and cardio- respiratory mortality: a review. Environ Health 12, 43 (2013). https://doi.org/10.1186/1476-069X-12-43
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-069X-12-43