
Abstract
Percentage of body fat is strongly associated with the risk of several chronic diseases but its accurate measurement is difficult. Bioelectrical impedance analysis (BIA) is a relatively simple, quick and non-invasive technique, to measure body composition. It measures body fat accurately in controlled clinical conditions but its performance in the field is inconsistent. In large epidemiologic studies simpler surrogate techniques such as body mass index (BMI), waist circumference, and waist-hip ratio are frequently used instead of BIA to measure body fatness. We reviewed the rationale, theory, and technique of recently developed systems such as foot (or hand)-to-foot BIA measurement, and the elements that could influence its results in large epidemiologic studies. BIA results are influenced by factors such as the environment, ethnicity, phase of menstrual cycle, and underlying medical conditions. We concluded that BIA measurements validated for specific ethnic groups, populations and conditions can accurately measure body fat in those populations, but not others and suggest that for large epdiemiological studies with diverse populations BIA may not be the appropriate choice for body composition measurement unless specific calibration equations are developed for different groups participating in the study.
Similar content being viewed by others


Introduction
In this review we discuss the issues associated with the application of bioelectrical impedance analysis (BIA) to measure body composition in large epidemiologic studies with multiethnic populations. The review is limited to healthy adults and does not include children, adolescents, elderly, and unhealthy individuals. The most recent system such as foot (or hand) to foot system is the main focus of this review and the early tetra-polar electrode system will not be discussed. These recent models are readily available and easy to use.
Percent body fat is strongly associated with the risk of chronic diseases such as hypertension, dyslipidemia, diabetes mellitus, and coronary heart disease [1–4]. In epidemiological studies, surrogate measures of body fatness such as body mass index (BMI), waist circumference, waist-hip ratio and skin fold thickness have been used extensively. However, these techniques do not precisely characterize persons by body composition (percentage of body fat or muscle mass), and there is substantial variation across age, sex and ethnic groups [5–7]. Several techniques have been used to assess percent body fat in controlled laboratory conditions. These include underwater weighing (densitometry), dual energy x-ray absorptiometry (DEXA), bioelectrical impedance analysis (BIA) and magnetic resonance imaging (MRI). However, densitometry, DEXA, and MRI are expensive, inconvenient for the participant, and not feasible to conduct in the field because they require large specialized equipment. For these reasons, their use in large epidemiological studies is limited.
BIA, by contrast, is relatively simple, quick (takes only a few minutes), and non-invasive which gives reliable measurements of body composition with minimal intra- and inter-observer variability [8]; the results are available immediately and reproducible with <1% error on repeated measurements [9]. This technique became commercially available for the first time in the mid- 1980s [10], and requires inexpensive, portable equipment, making it an appealing alternative to assess body composition in epidemiological studies [11].
Principles of bioelectrical impedance technique
BIA analysis is based on the principle that electric current flows at different rates through the body depending upon its composition. The body is composed mostly of water with ions, through which an electric current can flow. The water in the body is localized in two compartments: extra-cellular water (ECW, approximately 45%) and intracellular water (ICW, approximately 55%) [12]. On the other hand, the body also contains non-conducting materials (body fat) that provide resistance to the flow of electric current. Adipose tissue is significantly less conductive than muscle or bone [13]. The principal of BIA is that electric current passes through the body at a differential rate depending on body composition. Hence, there is a direct relationship between the concentrations of ions and the electrical conductivity and an indirect relationship exists between the ion concentration and the resistance of the solution.
Body impedance (Z) is defined as the opposition of a conductor to the flow of an alternating current, and consists of two components: resistance (R) and reactance (Xc). Resistance (R) is the major opposition of the conductor and at usual low frequency (50 kHz), the extra-cellular part of non-adipose tissue works as a resistor [14]. Reactance is an additional opposition or the storage of an electrical charge by a condenser for a short period of time; the lipid component of the membranes of the Body Cell Mass (BCM) behave as capacitors and reduce the flow of intracellular ions. In practice, impedance is the amount of dropped voltage when a small constant current (800 uA) with a fixed frequency (50 kHz) passes between electrodes spanning the body. However, lean tissue, which is rich in water and electrolytes, has minimal impedance and increases to a maximum when all lean tissue is replaced by fat/adipose tissue. Hence, lean body mass and Fat Mass (FM) can be calculated from the difference in conductivity [15].
The other assumptions for BIA measurement are that the body is a cylindrical-shaped ionic conductor with homogeneous composition, a fixed cross-sectional area and a uniform distribution of current density [16, 17]; BIA measures the impedance to the flow of an electric current through the total body fluid. Therefore, the conductive volume (V) which represents total body water (TBW) or FFM is directly related to the square length of conductor (S) and inversely correlated to resistance of the cross-section area (R), while p is the specific receptivity of the conductor, yielding the equation: V = p × S2/R. Based on this assumption, the same arms and legs respectively contribute to almost 47% and 50% of whole body resistance despite contributing to 4% and 17% of body weight respectively. In contrast, the trunk, which contains 50% of the body mass, contributes only 5–12% of whole body resistance [12].
Predictive equations
Many empirical equations have been developed for estimation of TBW, FFM and body cell mass (BCM), by using sex, age, weight, height and race as explanatory variables. However, predictive equations are generally population-specific and can be useful only for those populations with characteristics similar to those of the reference populations [18, 19]. When these equations have been used to predict body composition in different populations, the results have been inconsistent. The developed predictive equations cannot be generalized to diverse populations. Heyward and Wagner reviewed the reliability and validity of different equations for African Americans, Asians and Indian Americans. They found that the majority of studies indicated that the BIA method is not accurate when a generalized equation is applied for different ethnic groups [20].
Summary of bio-impedance technique
▪ Based on the principle that body fat impedes electric current more than body protein
▪ Impedance is a drop in voltage when a small constant current with a fixed frequency passes between electrodes spanning the body
▪ Predictive equations estimate TBW, FFM and body cell mass (BCM) using sex, age, weight, height and race
Validity of BIA measurements
The human body is not uniform either in length, cross-sectional area, or ionic composition and this affects the accuracy of BIA measurements [15]. In addition, body impedance varies among different ethnic groups and influences the accuracy of BIA [21]. Validity of hand to hand (Omron BF306 BIA) with a 4-C model was tested among Chinese and Japanese participants which showed different levels of biases in predicted levels of body fat (SEE = 4.5% BF) which may have resulted from different levels of body fat, age and relative arm span [22]. Demura et al. in a sample of 50 Japanese men aged 18 to 27 y. validated foot-to-foot (Tanita, TBF-102), and hand-to-hand (Omron, HBF-300) and hand-to-foot (Selco, SIF-891) BIA analyzers against hydro-densitometry (HD) [23]. They found higher correlation between hand to foot (r = 0.96) than foot to foot (r = 0.71) against HD as a reference method and there was 2.2% to 3.3% overestimation when they used the manufacturer's equations, therefore, they developed new equations for their sample. Jebb et al. tested the validity of foot-to-foot (Tanita -350) among 104 men and 101 women recruited from Dunn Nutrition Centre using DEXA as a reference method. The observed limit of agreement for fat mass was ± 7.9 kg [24]. A number of other factors that influence BIA results are described in this section.
Consumption of food or beverages
Although food or fluid intake before BIA measurement affects TBW and ECW, a general agreement on the ideal amount of time between food and fluid intake and BIA measurements has yet to be consolidated. It has been suggested that due to the large cross-sectional surface of the trunk, even fluid intake of up to 2 L is shown to be "electrically silent" during the first hour after consumption [25, 26]. Kaminsky and Whaley (1993) compared body fat percentage measurements after 3 hours and 12 hours of fasting and found no significant difference between these values [27]. Lukaski et al., (1986) emphasizes that dehydration increases resistance by nearly 40 Ω, which results in a 5.0 kg underestimation of FFM [28] and Evans et al., (1998) showed increased impedance one hour after eating a heavy meal [25]. In contrast, investigators have reported that food intake, its absorption and the resulting increase in movement of fluid into the bloodstream from 2–4 hours before BIA measurement, decreases the impedance value from 4 to 15 Ω, or <3% and results in overestimation of FFM by almost 1.5 kg [29]. Slinde and Rossander-Hulthen, after giving standard food to 18 healthy subjects, measured BIA 18 times during 24 hr. Their results showed that percentage of body fat varied by 8.8% and 9.9% from the highest to the lowest measurement in women and men respectively [30]. In contrast, Chumlea et al., (1987) found no effect of food consumption before BIA measurement on impedance measurements [31]. For these reasons undertaking an overnight fast is recommended as a routine standardization technique before impedance measurements [17, 32].
Exercise
Although exercise of mild intensity may not affect BIA measurements, moderate and intensive exercise before measurements may change the measured impedance by different mechanisms [33]. For example, exercise increases cardiac output and vascular perfusion and subsequently increases blood flow to skeletal muscle, which warms the muscle and decreases muscle resistance which results in reduced impedance [26]. In addition, intensive activity causes vasodilatation, an increase in skin temperature, which also reduces measured impedance [34]. Jogging or cycling at moderate intensities for 90–120 min decreases measured impedance by 50 to 70 Ω, which results in nearly a 12 kg overestimation of FFM [35]. Therefore, to reduce measurement error, BIA should not be performed within several hours of moderate to intensive exercise. In addition, the chosen mode for each individual may affect the accuracy of measurement. Swartz et al, in a well designed study, compared the % BF measured among high or moderately active and inactive individuals by hydrostatic weight and BIA using different athletic and adult modes in a foot-to-foot BIA (Tanita TBF-305). Their results showed that although the electrical impedance was not significantly different, the chosen adult mode for highly and moderately active individuals significantly overestimated the percent of body fat [36].
Medical conditions
Although some investigators have applied BIA method in various patients and clinical settings, it should be noted that there are some medical conditions which change serum electrolytes, hematocrit and blood flow, affecting Z and p, independent of body fluid volume [26]. Conversely, there are some other medical conditions, which via a change in fluid distribution alter Z measurements. Significant alteration in body hydration, fluid distribution and differences in the ratio of ECW to ICW caused by a medical condition will affect impedance measurements [37, 38]. Among those conditions, the most significant confounding variable is edema of the distal extremities, which is mainly caused by peripheral venous insufficiency. This insufficiency may result from congestive heart failure, cirrhosis, nephrotic syndrome, hypoalbuminemia, and lympheodema [39]. Other medical conditions, which affect BIA validity, include cutaneous disease that may alter electrode-skin electrical transmission in patients with amputations, poliomyelitis and muscular dystrophies. These conditions will have significant effects on the application of BIA in the clinical population [17, 40].
Environmental factors
Although environmental changes do not significantly affect actual whole body volume, they appear to alter the Z measurements by changing skin temperature. The result of several studies showed an inverse relation between skin temperature and impedance which means impedance increases with a lowering in temperature and decrease with a rise in skin temperature. Gudivaka et al observed 8% change in resistance at 50 kHz with 8.4°C change in skin temperature [41]. Thus, changes in cutaneous and muscle blood flow may have a large impact on BIA measurements in both clinical and field settings.
Within-subject variability
Due to increased progesterone plasma levels after ovulation and the change in hydration status, within-subject variability of impedance may be higher in women. The effect of this variability has been examined by several studies and various results have been reported. Gualdi-Russo et al., did not find significant differences in TBW estimated at different points in time during the follicular and premenstrual stages [42]. On the other hand, Gleichauf et al., suggested that the average of several measurements during a menstrual cycle could be considered as an estimation of body composition [43]. However, it has been recommended that BIA measurement not be taken at a time while the participant is experiencing large weight gain related to the menstrual cycle [44]. Menopause changes body composition and fat distribution and women experience a loss in lean mass and an increase in weight, fat mass and central fat deposition [45–49]. The ratio of fat/lean mass, especially in the lower part of the body increases [50, 51], which may affect the estimated impedance as the current passes through the legs. Therefore, the accuracy of BIA measurements increases by applying specific prediction equations for postmenopausal women [52].
Ethnicity
In recent years, BIA has been extensively applied among different age groups of both sexes, including mostly Caucasian populations of USA and Europe, and several prediction equations have been developed for these samples [53–55]. Also, a few prediction equations have been developed based on samples from African Americans, Hispanics and Native Americans [56]. Stolarczky et al., (1997) showed that by applying population-specific equations for estimation of lean body mass among Native American women, the standard error for estimating (SEE) decreased from 8.1 kg to 2.6 kg [56]. However, it has been suggested that biological and physiological assumptions for estimation of body composition, which are mainly based on Caucasian samples, may not be accurate for other ethnic groups. Hence, the validity of these equations must be tested in the population under study. There are several factors responsible for ethnic differences, which may affect the extent and direction of the error while measuring body composition by BIA such as:
• Fat distribution Ethnicity affects fat patterning and consequently influences the validity of equations. It has been shown that the proportion of fat deposition on trunk varies by 5.7% between different ethnic groups of Asians, Mexican Americans, Caucasians and African Americans [57].
• Body density Body density may have a significant impact on the accuracy of estimated lean body mass and fat-free mass. Several studies showed that African Americans have greater body density and greater body mass cell compared to Caucasian Americans [58, 59]. Swinburn et al., (1999) found that Polynesians in New Zealand have higher levels of fat-free mass and less body fat than Europeans at any given body mass index [60]. In contrast, Kyle et al., (2001) indicated that Japanese men and women had 10–12% higher body fat than Swiss men and women [55]. It has also been reported that Asian populations (Chinese, Malay, Singaporean Indians) have higher body fat percentages at a given BMI and Wang et al. reported a lower hydration of the FFM in Asians [6, 61].
In prediction equation calculations, it has been assumed that the fat free mass density does not vary among different ethnic groups. Because the density of FFM differs between different ethnic groups, this assumption may be a major source of error.
• Differences in proportional limb lengths as mentioned before, impedance demonstrates a direct relationship between conductive volume (V) and the square length of a conductor (S). Since whole body impedance is mainly based on the impedance of limbs [62], the differences among different racial groups may mostly relate to differences in proportion of limb lengths [63]. This hypothesis is supported by several studies, for example, whole-body impedance of Nigerians was significantly greater than that of matched Caucasian individuals, but was not different among different tribes of Nigeria [11]. Also, several other studies showed that black populations have longer limbs than white populations and increased lumbar lordosis [64–66].
Generally speaking, based on the preceding hypothesis, regarding age, race, level of activity etc. it has been suggested that the general prediction equation across different age and ethnic groups should not be applied without cross validating the study population [61, 67].
Summary of factors impacting BIA results
▪ Contact between limbs and trunk
▪ Inaccurate body weight
▪ Consumption of food and drink (overnight fast suggested)
▪ Moderate to intense level physical activity 2–3 hours before measurement
▪ Medical conditions impacting fluid and electrolyte balance
▪ Ambient temperature (cold increases impedance)
▪ Individual characteristics (abdominal obesity, muscle mass, weight loss, menstrual cycle, menopause)
▪ Ethnic variation, possibly mediated by body density and proportional limb length
Conclusion
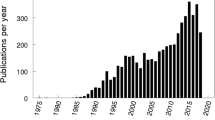
BIA has become a popular method for estimation of body composition during the last two decades. Since 1990, more than 1600 published articles have been reported using BIA as a tool of body composition measurement [17, 40, 68] and our search with the key words of body composition and bioelectrical impedance showed that 235 articles were published in English between 2004 and 2006 and we found different levels of agreements between different BIA models and reference methods. Also, there are many different equations for BIA calibration thus results of studies should be compared with more caution. BIA seems to reasonably estimate body composition in controlled conditions for healthy and euvolemic adults by applying a population specific predictive equation and it is not recommended to generalize a few equations for international epidemiologic studies, which involve participants from diverse populations. As far as we know, for some ethnic groups such as South Asians or Middle Easterners, or African residing in Africa predictive equations have not yet been developed. Hence, it is necessary to develop new predictive equations or cross validate existing equations on new populations to be studied.
If the BIA equation is not appropriately chosen based on age, gender, level of physical activity, level of body fat and ethnicity, the results of the study will not be reliable.
Overall BIA is a useful tool for clinical studies, but for large epidemiological studies with diverse population, particularly in developing nations, BIA has limited use unless valuation studies are conducted specifically for the populations under study.
References
Dentali F, Sharma AM, Douketis JD: Management of hypertension in overweight and obese patients: a practical guide for clinicians. Curr Hypertens Rep. 2005, 7: 330-336. 10.1007/s11906-005-0065-5.
Merchant AT, Anand SS, Vuksan V, Jacobs R, Davis B, Teo K, Yusuf S: Protein intake is inversely associated with abdominal obesity in a multi-ethnic population. J Nutr. 2005, 135: 1196-1201.
Sharma AM, Chetty VT: Obesity, hypertension and insulin resistance. Acta Diabetol. 2005, 42 (Suppl 1): S3-S8. 10.1007/s00592-005-0175-1.
Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L: Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004, 364: 937-952. 10.1016/S0140-6736(04)17018-9.
Dagenais GR, Yi Q, Mann JF, Bosch J, Pogue J, Yusuf S: Prognostic impact of body weight and abdominal obesity in women and men with cardiovascular disease. Am Heart J. 2005, 149: 54-60. 10.1016/j.ahj.2004.07.009.
Wang J, Thornton JC, Kolesnik S, Pierson RN: Anthropometry in body composition. An overview. Ann N Y Acad Sci. 2000, 904: 317-326.
Womersley J: A comparison of the skinfold method with extent of 'overweight' and various weight-height relationships in the assessment of obesity. Br J Nutr. 1977, 38: 271-284. 10.1079/BJN19770088.
Diaz EO, Villar J, Immink M, Gonzales T: Bioimpedance or anthropometry?. Eur J Clin Nutr. 1989, 43: 129-137.
Segal KR, Burastero S, Chun A, Coronel P, Pierson RN, Wang J: Estimation of extracellular and total body water by multiple-frequency bioelectrical-impedance measurement. Am J Clin Nutr. 1991, 54: 26-29.
Buchholz AC, Bartok C, Schoeller DA: The validity of bioelectrical impedance models in clinical populations. Nutr Clin Pract. 2004, 19: 433-446. 10.1177/0115426504019005433.
Azinge EC, Mabayoje M, Ward LC: Body proportions in three Nigerian tribes. Acta Diabetol. 2003, 40 (Suppl 1): S317-S319. 10.1007/s00592-003-0097-8.
Coppini LZ, Waitzberg DL, Campos AC: Limitations and validation of bioelectrical impedance analysis in morbidly obese patients. Curr Opin Clin Nutr Metab Care. 2005, 8: 329-332.
Scharfetter H, Schlager T, Stollberger R, Felsberger R, Hutten H, Hinghofer-Szalkay H: Assessing abdominal fatness with local bioimpedance analysis: basics and experimental findings. Int J Obes Relat Metab Disord. 2001, 25: 502-511. 10.1038/sj.ijo.0801556.
Kotler DP, Burastero S, Wang J, Pierson RN: Prediction of body cell mass, fat-free mass, and total body water with bioelectrical impedance analysis: effects of race, sex, and disease. Am J Clin Nutr. 1996, 64: 489S-497S.
Pietrobelli A, Heymsfield SB: Establishing body composition in obesity. J Endocrinol Invest. 2002, 25: 884-892.
Houtkooper LB, Lohman TG, Going SB, Howell WH: Why bioelectrical impedance analysis should be used for estimating adiposity. Am J Clin Nutr. 1996, 64: 436S-448S.
Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Manuel GJ, Lilienthal Heitmann B, Kent-Smith L, Melchior JC, Pirlich M, Scharfetter H, Schols WJ, Pichard C: Bioelectrical impedance analysis-part II: utilization in clinical practice. Clin Nutr. 2004, 23: 1430-1453. 10.1016/j.clnu.2004.09.012.
Deurenberg P, Deurenberg-Yap M, Schouten FJ: Validity of total and segmental impedance measurements for prediction of body composition across ethnic population groups. Eur J Clin Nutr. 2002, 56: 214-220. 10.1038/sj.ejcn.1601303.
Kyle UG, Piccoli A, Pichard C: Body composition measurements: interpretation finally made easy for clinical use. Curr Opin Clin Nutr Metab Care. 2003, 6: 387-393. 10.1097/00075197-200307000-00006.
Heyward VH, Wagner DR: Body composition and ethnicity. Applied body composition assessment. Human Kinetics. 2004, 135-172.
Ward LC, Heitmann BL, Craig P, Stroud D, Azinge EC, Jebb S, Cornish BH, Swinburn B, O'Dea K, Rowley K, McDermott R, Thomas BJ, Leonard D: Association between ethnicity, body mass index, and bioelectrical impedance. Implications for the population specificity of prediction equations. Ann N Y Acad Sci. 2000, 904: 199-202.
Deurenberg P, Deurenberg-Yap M: Validation of skinfold thickness and hand-held impedance measurements for estimation of body fat percentage among Singaporean Chinese, Malay and Indian subjects. Asia Pac J Clin Nutr. 2002, 11: 1-7. 10.1046/j.1440-6047.2002.00258.x.
Demura S, Yamaji S, Goshi F, Kobayashi H, Sato S, Nagasawa Y: The validity and reliability of relative body fat estimates and the construction of new prediction equations for young Japanese adult males. J Sports Sci. 2002, 20: 153-164. 10.1080/026404102317200864.
Jebb SA, Cole TJ, Doman D, Murgatroyd PR, Prentice AM: Evaluation of the novel Tanita body-fat analyser to measure body composition by comparison with a four-compartment model. Br J Nutr. 2000, 83: 115-122.
Evans WD, McClagish H, Trudgett C: Factors affecting the in vivo precision of bioelectrical impedance analysis. Appl Radiat Isot. 1998, 49: 485-487. 10.1016/S0969-8043(97)00061-4.
Kushner RF, Gudivaka R, Schoeller DA: Clinical characteristics influencing bioelectrical impedance analysis measurements. Am J Clin Nutr. 1996, 64: 423S-427S.
Kaminsky LA, Whaley MH: Differences in estimates of percent body fat using bioelectrical impedance. J Sports Med Phys Fitness. 1993, 33: 172-177.
Lukaski HC, Bolonchuk WW, Hall CB, Siders WA: Validation of tetrapolar bioelectrical impedance method to assess human body composition. J Appl Physiol. 1986, 60: 1327-1332.
Deurenberg P, Weststrate JA, Paymans I, van der KK: Factors affecting bioelectrical impedance measurements in humans. Eur J Clin Nutr. 1988, 42: 1017-1022.
Slinde F, Rossander-Hulthen L: Bioelectrical impedance: effect of 3 identical meals on diurnal impedance variation and calculation of body composition. Am J Clin Nutr. 2001, 74: 474-478.
Chumlea WC, Roche AF, Guo SM, Woynarowska B: The influence of physiologic variables and oral contraceptives on bioelectric impedance. Hum Biol. 1987, 59: 257-269.
Fogelholm M, Sievanen H, Kukkonen-Harjula K, Oja P, Vuori I: Effects of meal and its electrolytes on bioelectrical impedance. Basic Life Sci. 1993, 60: 331-332.
Garby L, Lammert O, Nielsen E: Negligible effects of previous moderate physical activity and changes in environmental temperature on whole body electrical impedance. Eur J Clin Nutr. 1990, 44: 545-546.
Caton JR, Mole PA, Adams WC, Heustis DS: Body composition analysis by bioelectrical impedance: effect of skin temperature. Med Sci Sports Exerc. 1988, 20: 489-491.
Abu KM, McCutcheon MJ, Reddy S, Pearman PL, Hunter GR, Weinsier RL: Electrical impedance in assessing human body composition: the BIA method. Am J Clin Nutr. 1988, 47: 789-792.
Swartz AM, Swartz AM, Jeremy EM, King GA, Thompson DL: Evaluation of a foot-to-foot bioelectrical impedance analyser in highly active, moderately active and less active young men. Br J Nutr. 2002, 88: 205-210.
Battistini N, Facchini F, Bedogni G, Severi S, Fiori G, Pettener D: The prediction of extracellular and total body water from bioelectric impedance in a non-Caucasian population from central Asia. Ann Hum Biol. 1995, 22: 315-320. 10.1080/03014469500003982.
Piccoli A, Rossi B, Pillon L, Bucciante G: Body fluid overload and bioelectrical impedance analysis in renal patients. Miner Electrolyte Metab. 1996, 22: 76-78.
Guglielmi FW, Mastronuzzi T, Pietrini L, Panarese A, Panella C, Francavilla A: The RXc graph in evaluating and monitoring fluid balance in patients with liver cirrhosis. Ann N Y Acad Sci. 1999, 873: 105-111. 10.1111/j.1749-6632.1999.tb09456.x.
Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P, Elia M, Gomez JM, Heitmann BL, Kent-Smith L, Melchior JC, Pirlich M, Scharfetter H, Schols AM, Pichard C: Bioelectrical impedance analysis – part I: review of principles and methods. Clin Nutr. 2004, 23: 1226-1243. 10.1016/j.clnu.2004.06.004.
Gudivaka R, Schoeller D, Kushner RF: Effect of skin temperature on multifrequency bioelectrical impedance analysis. J Appl Physiol. 1996, 81: 838-845.
Gualdi-Russo E, Toselli S: Influence of various factors on the measurement of multifrequency bioimpedance. Homo. 2002, 53: 1-16. 10.1078/0018-442X-00035.
Gleichauf CN, Roe DA: The menstrual cycle's effect on the reliability of bioimpedance measurements for assessing body composition. Am J Clin Nutr. 1989, 50: 903-907.
Heyward VH: Practical body composition assessment for children, adults, and older adults. Int J Sport Nutr. 1998, 8: 285-307.
Macdonald HM, New SA, Campbell MK, Reid DM: Longitudinal changes in weight in perimenopausal and early postmenopausal women: effects of dietary energy intake, energy expenditure, dietary calcium intake and hormone replacement therapy. Int J Obes Relat Metab Disord. 2003, 27: 669-676. 10.1038/sj.ijo.0802283.
Toth MJ, Gardner AW, Ades PA, Poehlman ET: Contribution of body composition and physical activity to age-related decline in peak VO2 in men and women. J Appl Physiol. 1994, 77: 647-652.
Wang Q, Hassager C, Ravn P, Wang S, Christiansen C: Total and regional body-composition changes in early postmenopausal women: age-related or menopause-related?. Am J Clin Nutr. 1994, 60: 843-848.
Wing RR, Matthews KA, Kuller LH, Meilahn EN, Plantinga PL: Weight gain at the time of menopause. Arch Intern Med. 1991, 151: 97-102. 10.1001/archinte.151.1.97.
Zamboni M, Turcato E, Santana H, Maggi S, Harris TB, Pietrobelli A, Heymsfield SB, Micciolo R, Bosello O: The relationship between body composition and physical performance in older women. J Am Geriatr Soc. 1999, 47: 1403-1408.
Chen Z, Bassford T, Green SB, Cauley JA, Jackson RD, LaCroix AZ, Leboff M, Stefanick ML, Margolis KL: Postmenopausal hormone therapy and body composition – a substudy of the estrogen plus progestin trial of the Women's Health Initiative. Am J Clin Nutr. 2005, 82: 651-656.
Reubinoff BE, Wurtman J, Rojansky N, Adler D, Stein P, Schenker JG, Brzezinski A: Effects of hormone replacement therapy on weight, body composition, fat distribution, and food intake in early postmenopausal women: a prospective study. Fertil Steril. 1995, 64: 963-968.
Xie X, Kolthoff N, Barenholt O, Nielsen SP: Validation of a leg-to-leg bioimpedance analysis system in assessing body composition in postmenopausal women. Int J Obes Relat Metab Disord. 1999, 23: 1079-1084. 10.1038/sj.ijo.0801034.
Deurenberg P, Weststrate JA, Seidell JC: Body mass index as a measure of body fatness: age- and sex-specific prediction formulas. Br J Nutr. 1991, 65: 105-114. 10.1079/BJN19910073.
Deurenberg P, Deurenberg-Yap M: Differences in body-composition assumptions across ethnic groups: practical consequences. Curr Opin Clin Nutr Metab Care. 2001, 4: 377-383. 10.1097/00075197-200109000-00007.
Kyle UG, Genton L, Karsegard L, Slosman DO, Pichard C: Single prediction equation for bioelectrical impedance analysis in adults aged 20–94 years. Nutrition. 2001, 17: 248-253. 10.1016/S0899-9007(00)00553-0.
Stolarczyk LM, Heyward VH, Van Loan MD, Hicks VL, Wilson WL, Reano LM: The fatness-specific bioelectrical impedance analysis equations of Segal et al: are they generalizable and practical?. Am J Clin Nutr. 1997, 66: 8-17.
Malina RM, Huang YC, Brown KH: Subcutaneous adipose tissue distribution in adolescent girls of four ethnic groups. Int J Obes Relat Metab Disord. 1995, 19: 793-797.
Jakicic JM, Wing RR, Lang W: Bioelectrical impedance analysis to assess body composition in obese adult women: the effect of ethnicity. Int J Obes Relat Metab Disord. 1998, 22: 243-249. 10.1038/sj.ijo.0800576.
Merz AL, Trotterm M, Peterson RR: Estimation of skeleton weight in the living. Am J Phys Anthropol. 1956, 14: 589-609. 10.1002/ajpa.1330140405.
Swinburn BA, Ley SJ, Carmichael HE, Plank LD: Body size and composition in Polynesians. Int J Obes Relat Metab Disord. 1999, 23: 1178-1183. 10.1038/sj.ijo.0801053.
Deurenberg-Yap M, Schmidt G, van Staveren WA, Deurenberg P: The paradox of low body mass index and high body fat percentage among Chinese, Malays and Indians in Singapore. Int J Obes Relat Metab Disord. 2000, 24: 1011-1017. 10.1038/sj.ijo.0801353.
Fuller NJ, Elia M: Potential use of bioelectrical impedance of the 'whole body' and of body segments for the assessment of body composition: comparison with densitometry and anthropometry. Eur J Clin Nutr. 1989, 43: 779-791.
Wagner DR, Heyward VH: Measures of body composition in blacks and whites: a comparative review. Am J Clin Nutr. 2000, 71: 1392-1402.
Harsha DW, Frerichs RR, Berenson GS: Densitometry and anthropometry of black and white children. Hum Biol. 1978, 50: 261-280.
Malina RM: Skinfolds in American Negro and white children. J Am Diet Assoc. 1971, 59: 34-40.
Rahmani A, Locatelli E, Lacour JR: Differences in morphology and force/velocity relationship between Senegalese and Italian sprinters. Eur J Appl Physiol. 2004, 91: 399-405. 10.1007/s00421-003-0989-x.
de Waart FG, Li R, Deurenberg P: Comparison of body composition assessments by bioelectrical impedance and by anthropometry in premenopausal Chinese women. Br J Nutr. 1993, 69: 657-664. 10.1079/BJN19930067.
Barbosa-Silva MC, Barros AJ: Bioelectrical impedance analysis in clinical practice: a new perspective on its use beyond body composition equations. Curr Opin Clin Nutr Metab Care. 2005, 8: 311-317.
Acknowledgements
We wish to thank Dr. Yusuf (Director of Population Health Research Institute) for all his supports and guidance.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
MD ran the electronic searches, reviewed all abstracts and articles, coordinated and drafted the manuscript. ATM participated in reviewing the articles and helped to draft the manuscripts.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Dehghan, M., Merchant, A.T. Is bioelectrical impedance accurate for use in large epidemiological studies?. Nutr J 7, 26 (2008). https://doi.org/10.1186/1475-2891-7-26
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2891-7-26