
Abstract
Currently the world faces epidemic of several closely related conditions: obesity, metabolic syndrome and type 2 diabetes (T2DM). The lipid profile of these patients and those with metabolic syndrome is characterized by the concurrent presence of qualitative as well as quantitative lipoprotein abnormalities: low levels of HDL, increased triglycerides, and prevalence of LDL particles that are smaller and denser than normal. This lipid phenotype has been defined as atherogenic dyslipidemia. Overwhelming evidences demonstrate that all components of the atherogenic dyslipidemia are important risk-factors for cardiovascular diseases. Optimal reduction of cardiovascular risk through comprehensive management of atherogenic dyslipidemias basically depends of the presence of efficacious lipid-modulating agents (beyond statin-based reduction of LDL-C). The most important class of medications which can be effectively used nowadays to combat atherogenic dyslipidemias is the fibrates. From a clinical point of view, in all available 5 randomized control trials beneficial effects of major fibrates (gemfibrozil, fenofibrate, bezafibrate) were clearly demonstrated and were highly significant in patients with atherogenic dyslipidemia. In these circumstances, the main determinant of the overall results of the trial is mainly dependent of the number of the included appropriate patients with atherogenic dyslipidemia. In a meta-analysis of dyslipidemic subgroups totaling 4726 patients a significant 35% relative risk reduction in cardiovascular events was observed compared with a non significant 6% reduction in those without dyslipidemia. However, different fibrates may have a somewhat different spectrum of effects. Currently only fenofibrate was investigated and proved to be effective in reducing microvascular complications of diabetes. Bezafibrate reduced the severity of intermittent claudication. Cardinal differences between bezafibrate and other fibrates are related to the effects on glucose metabolism and insulin resistance. Bezafibrate is the only clinically available pan - (alpha, beta, gamma) PPAR balanced activator. Bezafibrate decreases blood glucose level, HbA1C, insulin resistance and reduces the incidence of T2DM compared to placebo or other fibrates. Among major fibrates, bezafibrate appears to have the strongest and fenofibrate the weakest effect on HDL-C. Current therapeutic use of statins as monotherapy is still leaving many patients with atherogenic dyslipidemia at high risk for coronary events because even intensive statin therapy does not eliminate the residual cardiovascular risk associated with low HDL and/or high triglycerides. As compared with statin monotherapy (effective mainly on LDL-C levels and plaque stabilization), the association of a statin with a fibrate will also have a major impact on triglycerides, HDL and LDL particle size. Moreover, in the specific case of bezafibrate one could expect neutralizing of the adverse pro-diabetic effect of statins. Though muscle pain and myositis is an issue in statin/fibrate treatment, adverse interaction appears to occur to a significantly greater extent when gemfibrozil is administered. However, bezafibrate and fenofibrate seems to be safer and better tolerated. Combined fibrate/statin therapy is more effective in achieving a comprehensive lipid control and may lead to additional cardiovascular risk reduction, as could be suggested for fenofibrate following ACCORD Lipid study subgroup analysis and for bezafibrate on the basis of one small randomized study and multiple observational data. Therefore, in appropriate patients with atherogenic dyslipidemia fibrates- either as monotherapy or combined with statins – are consistently associated with reduced risk of cardiovascular events. Fibrates currently constitute an indispensable part of the modern anti-dyslipidemic arsenal for patients with atherogenic dyslipidemia.
Similar content being viewed by others


Atherogenic dyslipidemia
Currently the world faces epidemic of closely related conditions: obesity, metabolic syndrome and type 2 diabetes (T2DM)[1–6]. A strong correlation between T2DM and cardiovascular diseases is well established[7–9]. Also for the metabolic syndrome (MetS) the best available evidence from randomized control trials (RCT) and large meta-analyses systematically had shown increased risk of cardiovascular events[10–14]. The recent and largest meta-analysis[12] included near one million patients (total n = 951,083). The investigators concluded that the MetS is associated with a 2-fold increase in cardiovascular outcomes and a 1.5-fold increase in all-cause mortality rates.
The lipid profile of patients with T2DM and MetS is characterized by the concurrent presence of qualitative as well as quantitative lipoprotein abnormalities: low levels of high density lipoprotein cholesterol (HDL-C) (<50 mg/dl in women, < 40 mg/dl in men), increased triglycerides (TG >150 mg/dl), and prevalence of low density lipoprotein (LDL) particles that are smaller and denser than normal (Figure 1). This lipid phenotype has been defined as atherogenic dyslipidemia[15–20]. Interestingly, elevated LDL cholesterol (LDL-C) level is not typical of T2DM nor MetS. Overwhelming evidences demonstrate that all components of the atherogenic dyslipidemia are important risk-factors for cardiovascular diseases[21–25].

Atherogenic Dyslipidemia triad: the lipid profile which is typical for patients with type 2 diabetes and the metabolic syndrome is characterized by the low HDL-C, increased triglycerides and prevalence of small, dense LDL particles.
Particularly, a strong association exists between elevated triglycerides and cardiovascular disease. However, the extent to which triglycerides directly promote disease or represent a biomarker of risk has been debated for decades. The largest and most comprehensive recent meta-analysis included 29 prospective studies and 262,525 participants, proving a strong and highly significant association between triglycerides and coronary risk. Adjustment for HDL-C attenuated the magnitude but did not abolish the significant association between triglycerides and coronary risk[26]. The triglyceride -rich environment has been shown to be strongly associated with an atherogenic lipoprotein phenotype or atherogenic dyslipidemia[22]. In the United States, the National Health and Nutrition Examination Survey (NHANES) has monitored biomarkers of cardiovascular risk for 3 decades. Accordingly, increases in fasting serum triglyceride levels were observed between surveys conducted in 1976–1980 and 1999–2002[27]. Also, nonfasting triglyceride strongly correlated with coronary risk[28, 29]. There is a broad agreement that reverse cholesterol transport, the process of transporting excess cholesterol from the arterial wall’s foam macrophages to the liver, bile, and feces is one of HDL’s important anti-atherogenic properties. Circulating HDL particles are greatly heterogeneous with a very complex metabolic profile. HDL-C measures the cholesterol content of nascent HDL, HDL2, and HDL3 particles and is, therefore, a crude marker of reverse cholesterol transport, whereas non-HDL-cholesterol is a valid marker of coronary risk[30–34].
Optimal reduction of cardiovascular risk through a comprehensive management of atherogenic dyslipidemias basically depends of the presence of efficacious lipid-modulating agents (beyond statin-based reduction of LDL-C). However, most of these agents are currently under serious concerns: niacin after negative AIM HIGH study[35] and before HPS-2 THRIVE trial results, and cholesteryl ester transfer protein (CETP) -inhibitors and glitazars are still in controversial developments and not available for clinical use. Omega-3 polyunsaturated fatty acids supplementation seems to not really influence major cardiovascular outcomes[36]. Therefore, the single class of medications which can be at the moment effectively used to combat atherogenic dyslipidemia beyond statins is only fibric acid derivatives - fibrates.
The role of fibrates in the management of atherogenic dyslipidemia
Fibrates are used in clinical practice for about half century due to their ability to substantially decrease triglyceride levels and increase HDL. All fibrates are peroxisome proliferators-activated receptors (PPARs) α agonists. Fibrates enhance the oxidation of fatty acids (FA) in liver and muscle and reduce the rate of hepatic lipogenesis, thereby reducing secretion of very-low-density lipoprotein (VLDL) triglycerides. The increased uptake of triglyceride-derived fatty acids in muscle cells results from an increase in lipoprotein lipase (LPL) activity in adjacent capillaries and a decrease in the apolipoprotein CIII (Apo CIII) concentration mediated transcriptionally by PPAR alpha. The decrease in apolipoprotein CIII reduces the inhibition of LPL activity. The enhanced catabolism of VLDL generates surface remnants, which are transferred to HDL. HDL concentrations are further augmented by an increase in PPARα - mediated transcription of apolipoprotein AI (Apo AI) and apolipoprotein AII (Apo AII). Ultimately, the rate of HDL-mediated reverse cholesterol transport may increase. Fibrates activate PPARα, which binds to a PPARα response element in conjunction with the retinoid X receptor. Other effects of fibrates include an increase in the size of LDL particles, increased removal of LDL, and a reduction in the levels of plasminogen activator inhibitor type I[37, 38].
From a clinical point of view, in all available 5 randomized control trials (Table 1) the beneficial effects of major fibrates (gemfibrozil, fenofibrate, bezafibrate) were clearly demonstrated and were highly significant in patients with atherogenic dyslipidemia[39–45]. For example, fenofibrate in the FIELD study: no significance in “general population”, already significant 14% risk reduction in low HDL subgroup, 23% significant risk reduction in high triglycerides subgroup and 27% significant risk reduction in patients with atherogenic dyslipidemia[41]. In the earliest and the most successful Helsinki Heart Study with gemfibrozil, near all benefits were derived from the patients with atherogenic dyslipidemia without any impressive effects in other subgroups[43]. The same is true for bezafibrate in the BIP trial[42], for fenofibrate in the ACCORD-Lipid trial[39] and for gemfibrozil in the VA-HIT trial[44]. We can see amazing similarity among all fibrates trials. In these circumstances, the key determinant of the overall results of the trial is dependent mainly on the number of the included appropriate patients with atherogenic dyslipidemia. So, in the ACCORD-Lipid trial there were only 17% appropriate patients with atherogenic dyslipidemia (941 of 5489)! In these patients 31% risk reductions was achieved (hazard ratio = 0.69, 95% confidence interval 0.49 - 0.97, p = 0.03 for within subgroup analysis, p for interaction = 0.057). However, 83% of patients in this trial were inappropriate for a fibrate treatment. Among them, the event rate was 10.1% in both treatment groups. Thus, overall results of the ACCORD-Lipid trial did not reach significance and this inappropriate patients selection lead to fail of the study.
In a recent meta-analysis of five dyslipidemic subgroups totaling 4726 patients, a 35% relative risk reduction in cardiovascular events was observed compared with a non significant 6% reduction in those without dyslipidemia[46]. Meta-analysis performed in a so called “general population”[47] reflecting a blend of effects in patients with and without atherogenic dyslipidemia - a “mean diluted” effect of fibrate therapy was reduced, producing only 13% RR reduction for coronary events (p < 0.0001). Figure 2 illustrates a dilution effect in epidemiology: strong significant cardiovascular risk reduction in patients with atherogenic dyslipidemia, non significant effect in those without dyslipidemia and blended modest effect in the mixed “general population”.

Therefore, in patients with atherogenic dyslipidemia (high triglycerides and low HDL-C), fibrates - either as monotherapy or combined with statins - are consistently associated with reduced risk of cardiovascular events. In patients without dyslipidemia this favorable effect - as expected - is absent.
Fibrates: different spectrum of effects
However, different fibrates may have a somewhat dissimilar spectrum of effects. Currently only fenofibrate[39, 41] was investigated in deep and proved to be effective in reducing microvascular complications of diabetes (in terms of diabetic retinopathy, progression of microalbuminuria and risk of limb amputations). However, there is no reason to suggest that other fibrates cannot do the same. The strongest hints for this were obtained in the large LEADER study when bezafibrate significantly reduced the severity of intermittent claudication for up to three years[48]. In addition, bezafibrate effectively reduced microvascular complications in a experimental study[49]. Also in the old RCTs, clofibrate was partially effective in the treatment of diabetic retinopathy due to an increased rate of absorption of hard exudates[50, 51].
The underlying mechanisms of these effects are not fully elucidated. The reductions in the risk of T2DM-related retinopathy and risk of amputation with fenofibrate were apparently independent of effects on lipid parameters. The leading hypothesis included activation of PPARα which can modulate angiogenesis through a mechanism dependent on vascular endothelial growth factor[52]. Actions arising via PPARα activation are likely to be shared between all fibric acid derivatives[52]. Alternatively, influence on endothelial function, anti-inflammatory and anti-apoptotic effects and decreased circulating levels of fibrinogen could be involved[52, 53].
Cardinal differences between bezafibrate and other fibrates are related to effects on glucose metabolism and insulin resistance. Bezafibrate, in contrast to other fibrates is pan - (alpha, beta, gamma) PPAR balanced activator[54, 55]. Bezafibrate leads to long-term stabilization of insulin sensitivity and pancreatic beta-cell function, reduced blood glucose level and HbA1C[56–59]. In addition, bezafibrate significantly increased serum adiponectin level[60]. Multiple studies have shown that bezafibrate reduced the incidence of T2DM by 30-40% compared to placebo or other fibrates during a long-term follow-up period[61–63].
In patients with MetS, bezafibrate treatment was associated with significant 29% reduced risk of any MI and 33% reduced risk of non-fatal MI. The early decrease in MI incidence was reflected later in a tendency of reduced cardiac mortality. Of note, among patients with augmented features of MetS (4–5 risk factors for MetS) a marked 56% reduction in cardiac mortality on bezafibrate was observed[64]. Of course, caution should be used in interpreting these findings, which were identified in a post-hoc analysis.
What is the place of fibrates in the statins world?
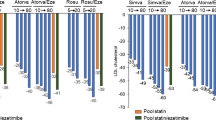
Until now, there were no direct “head to head” statin vs. fibrate comparisons at all. Only recently intermediate-size (274 patients) RCT have demonstrated that bezafibrate was significantly better than pravastatin (a relatively weak statin) in reduction of cardiovascular events[65]. Anyway, even intensive statin therapy does not eliminate the cardiovascular risk associated with low HDL or/and high triglycerides (atherogenic dyslipidemia)! Current therapeutic use of statins as monotherapy is still leaving many patients with combined dyslipidemia (which included atherogenic dyslipidemia) at high residual risk for coronary events[38, 66–74]. Figure 3A is a graphic representation of the definition of residual cardiovascular risk in patients treated by conventional statin therapy. The significant residual cardiovascular risk is still present and is not affected by standard LDL - lowering therapy.

A. Residual risk in people with diabetes and atherogenic dyslipidemia: effect of standard-dose statin therapy, pooled data [66–74]. Red column represents the coronary risk in the people with diabetes and atherogenic dyslipidemia treated by statins as compared to placebo (blue column), and the patients without diabetes and atherogenic dyslipidemia treated by statins (green column). The yellow arrows demonstrate the additional coronary risk of the diabetic patients with atherogenic dyslipidemia treated by statins. B. Residual risk in people with diabetes and atherogenic dyslipidemia: effect of intenesive statin therapy. The hypothetical extra benefit obtained by intensive statin therapy based on the meta-analysis (it is presented by the white box)[80]. Residual risk is still remained considerable.
The next step in the risk reduction was the concept of “intensive” high dose statin therapy. Direct testing of varying degrees (intensive vs. conventional) of LDL-C lowering by using of active comparators (statin vs. statin) has been tested in 5 large outcomes trials[75–79]: PROVE IT--TIMI 22, A to Z, TNT, IDEAL and SEARCH. Out of the 5 trials which investigated intensive vs. standard statin regime, we have 2 “positive” with strong reservations: PROVE IT-TIMI 22 (it was based on very strange study design) and TNT (total death moved in a wrong direction) - and 3 “negative”: A to Z, IDEAL and SEARCH. Anyway, pooled data were in favour of the intensive statin therapy[80]. Figure 3B illustrates the hypothetical extra benefit obtained by intensive statin therapy based on the meta-analysis (represented by the white box). Residual risk is still remained considerable. Significant increase in side effects during intensive therapy was observed (elevations of liver enzymes, muscle aches, cognitive decline and the development of diabetes mellitus)[38, 80–83].
The risk associated with high triglycerides and low HDL may be eliminated by fibrate. Among major fibrates, bezafibrate appears to have the strongest[42, 48] and fenofibrate the weakest[39, 45] effect on HDL-C (Figure 4). As compared with statin monotherapy (effective mainly on LDL-C levels and plaque stabilization), the association of a statin with a fibrate will also have a major impact on triglycerides, HDL and LDL particle size. Moreover, in the case of bezafibrate one could expect neutralizing of the adverse pro-diabetic effect of statins. Though muscle pain and myositis is an issue in statin/fibrate treatment, adverse interaction appears to occur to a significantly greater extent when gemfibrozil is administered. However, bezafibrate and fenofibrate seem to be safer and better tolerated[84–93].

Particularly, plasma concentration of statins are markedly increased by gemfibrozil but not by fenofibrate or bezafibrate[89, 90, 93]. So, gemfibrozil, which is a good “evidence-based” fibrate for monotherapy, apears to be a problematic in the “statins world”. Unfortunately, safety concerns about gemfibrozil may lead to exaggerate precautions regarding fibrate administration and therefore diminish the use of these useful agents.
In a fibrate/statin combined therapy, the statin should probably be taken at the evening and the fibrate in the morning to avoid matched peak dose concentrations. Anyway, although in clinical trials the rate of adverse events on combination was not significantly greater compared with monotherapy, clinical and laboratory monitoring of patients who receive combined treatment could be prudent.
Currently there are a few hard outcome evidences regarding a combination statin/fibrate. In ACCORD Lipid study fenofibrate leads to cardiovascular risk reduction in pre-specified subgroup of patients with atherogenic dyslipidemia[39]. In the observational study of the 150 patients, the combination of bezafibrate and simvastatin was more effective than monotherapy in reduction of cardiovascular events[92]. In the small randomized controlled trial bezafibrate on top of statin-based treatment was a safe and significantly reduced major adverse cardiovascular events (MACE) in patients with acute ST elevation MI[94]. The authors particularly emphasized in this study ability of bezafibrate significantly reduced fibrinogen levels.
Recently, new data regarding statin/fibrate combination were published using the high quality comprehensive nationwide ACSIS registry[95]. There were 8545 patients treated with statin alone and 437 patients treated with a statin/fibrate combination (mainly bezafibrate). Development of 30-day MACE (primary end-point) was recorded in 6.0% patients from the statin monotherapy group vs. 3.2% from the combination group, (p = 0.01). 30-day re-hospitalization rate was also significantly lower in the combination group. Kaplan-Meier analysis of total mortality during one year was close to significance in favor of the combination (p = 0.066). Multivariate analysis identified the fibrate/statin combination as an independent predictor of 46% reduced risk of MACE in overall population (p = 0.03). In the subgroup interaction analysis the most impressive results were found in the subgroup with diabetes and atherogenic dyslipidemia. As one could expect, in patients without dyslipidemia this effect was absent. It should be emphasized that even though these “real world” observation data cannot replace RCT, the consistency of the results supports their credibility.
Conclusions
Even intensive statin therapy does not eliminate the residual cardiovascular risk associated with atherogenic dyslipidemia (low HDL and high triglycerides). Meta-analyses of randomized control trials clearly demonstrated that the main fibrates significantly reduce this risk. Combined fibrate/statin therapy is more effective in achieving a comprehensive lipid control and may lead to additional cardiovascular risk reduction, as could be suggested for fenofibrate following ACCORD Lipid study subgroup analysis and for bezafibrate on the bais on one small randomized study and multiple observational data. Therefore, in appropriate patients with atherogenic dyslipidemia fibrates- either as monotherapy or combined with statins – are consistently associated with reduced risk of cardiovascular events. Fibrates currently are an indispensable part of the modern anti-dyslipidemic arsenal for patients with atherogenic dyslipidemia.
Abbreviations
- ACSIS:
-
Acute Coronary Syndromes-Israel Survey
- BIP:
-
Bezafibrate Infarction Prevention study
- CETP:
-
Cholesteryl ester transfer protein
- CHD:
-
Coronary heart disease
- FA:
-
Fatty acids
- HDL-C:
-
High density lipoprotein cholesterol
- LDL-C:
-
Low density lipoprotein cholesterol
- LPL:
-
Lipoprotein lipase
- MACE:
-
Major adverse cardiovascular events
- MI:
-
Myocardial infarction
- PPARs:
-
Peroxisome proliferators-activated receptors
- RCT:
-
The randomized control trials
- VLDL:
-
Very-low-density lipoprotein.
References
Brown M, Byatt T, Marsh T, McPherson K: National heart forum: micro simulation of obesity trends 2006 – 2050: obesity trends for adults analysis from the health survey for England 1993 – 2007 February 2010. 2010, National Heart Forum, London, http://nhfshare.heartforum.org.uk/RMAssets/NHFreports/NHF_adultobese_short_170210.pdf (Accessed October 1 2012)
National Diabetes Information Clearinghouse (NDIC): Diabetes overview. NIH publication No. 09–3873. 2008, http://diabetes.niddk.nih.gov/dm/pubs/overview/ (Accessed October 1 2012)
van Vliet M, Heymans MW, von Rosenstiel IA, Brandjes DP, Beijnen JH, Diamant M: Cardiometabolic risk variables in overweight and obese children: a worldwide comparison. Cardiovasc Diabetol. 2011, 10: 106-10.1186/1475-2840-10-106.
Tenenbaum A, Motro M, Schwammenthal E, Fisman EZ: Macrovascular complications of metabolic syndrome: an early intervention is imperative. Int J Cardiol. 2004, 97: 167-172. 10.1016/j.ijcard.2003.07.033.
Centers for Disease Control and Prevention: National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States, 2011. 2011, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Atlanta
Tenenbaum A, Fisman EZ: “The metabolic syndrome… is dead”: these reports are an exaggeration. Cardiovasc Diabetol. 2011, 10: 11-10.1186/1475-2840-10-11.
Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M: Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998, 339: 229-234. 10.1056/NEJM199807233390404.
Donahoe SM, Stewart GC, McCabe CH, Mohanavelu S, Murphy SA, Cannon CP, Antman EM: Diabetes and mortality following acute coronary syndromes. JAMA. 2007, 298: 765-775. 10.1001/jama.298.7.765.
Reynoso-Noverón N, Mehta R, Almeda-Valdes P, Rojas-Martinez R, Villalpando S, Hernández-Ávila M, Aguilar-Salinas CA: Estimated incidence of cardiovascular complications related to type 2 diabetes in Mexico using the UKPDS outcome model and a population-based survey. Cardiovasc Diabetol. 2011, 10: 1-10.1186/1475-2840-10-1.
Gami AS, Witt BJ, Howard DE, Erwin PJ, Gami LA, Somers VK, Montori VM: Metabolic syndrome and risk of incident cardiovascular events and death: a systematic review and meta-analysis of longitudinal studies. J Am Coll Cardiol. 2007, 49: 403-414. 10.1016/j.jacc.2006.09.032.
Galassi A, Reynolds K, He J: Metabolic syndrome and risk of cardiovascular disease: a meta-analysis. Am J Med. 2006, 119: 812-819. 10.1016/j.amjmed.2006.02.031.
Mottillo S, Filion KB, Genest J, Joseph L, Pilote L, Poirier P, Rinfret S, Schiffrin EL, Eisenberg MJ: The metabolic syndrome and cardiovascular risk. A systematic review and meta-analysis. J Am Coll Cardiol. 2010, 56: 1113-1132. 10.1016/j.jacc.2010.05.034.
Scott R, Donoghoe M, Watts GF, O’Brien R, Pardy C, Taskinen MR, Davis TM, Colman PG, Manning P, Fulcher G, Keech AC, FIELD Study Investigators: Impact of metabolic syndrome and its components on cardiovascular disease event rates in 4900 patients with type 2 diabetes assigned to placebo in the FIELD randomised trial. Cardiovasc Diabetol. 2011, 10: 102-10.1186/1475-2840-10-102.
Ninomiya JK, L’Italien G, Criqui MH, Whyte JL, Gamst A, Chen RS: Association of the metabolic syndrome with history of myocardial infarction and stroke in the Third National Health and Nutrition Examination Survey. Circulation. 2004, 109: 42-46. 10.1161/01.CIR.0000116602.10533.2E.
Austin MA, Breslow JL, Hennekens CH, Buring JE, Willett WC, Krauss RM: Low-density lipoprotein subclass patterns and risk of myocardial infarction. JAMA. 1988, 260: 1917-1921. 10.1001/jama.1988.03410130125037.
Austin MA, King MC, Vranizan KM, Krauss RM: Atherogenic lipoprotein phenotype. A proposed genetic marker for coronary heart disease risk. Circulation. 1990, 82: 495-506. 10.1161/01.CIR.82.2.495.
National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002, 106: 3143-3421.
Tenenbaum A, Fisman EZ, Motro M, Adler Y: Atherogenic dyslipidemia in metabolic syndrome and type 2 diabetes: therapeutic options beyond statins. Cardiovasc Diabetol. 2006, 5: 20-10.1186/1475-2840-5-20.
Ghandehari H, Kamal-Bahl S, Wong ND: Prevalence and extent of dyslipidemia and recommended lipid levels in US adults with and without cardiovascular comorbidities: the National Health and Nutrition Examination Survey 2003–2004. Am Heart J. 2008, 156: 112-119. 10.1016/j.ahj.2008.03.005.
Rizzo M, Berneis K: Lipid triad or atherogenic lipoprotein phenotype: a role in cardiovascular prevention?. J Atheroscler Thromb. 2005, 12: 237-239. 10.5551/jat.12.237.
Li C, Ford ES, Tsai J, Zhao G, Balluz LS, Gidding SS: Serum non-high-density lipoprotein cholesterol concentration and risk of death from cardiovascular diseases among U.S. adults with diagnosed diabetes: the Third National Health and Nutrition Examination Survey linked mortality study. Cardiovasc Diabetol. 2011, 10: 46-10.1186/1475-2840-10-46.
Sarwar N, Sandhu MS, Ricketts SL, Butterworth AS, Di Angelantonio E, Boekholdt SM, Ouwehand W, Watkins H, Samani NJ, Saleheen D, Lawlor D, Reilly MP, Hingorani AD, Talmud PJ, Danesh J, Triglyceride Coronary Disease Genetics Consortium and Emerging Risk Factors Collaboration: Triglyceride-mediated pathways and coronary disease: collaborative analysis of 101 studies. Lancet. 2010, 375: 1634-1639.
Chaudhary R, Likidlilid A, Peerapatdit T, Tresukosol D, Srisuma S, Ratanamaneechat S, Sriratanasathavorn C: Apolipoprotein E gene polymorphism: effects on plasma lipids and risk of type 2 diabetes and coronary artery disease. Cardiovasc Diabetol. 2012, 11: 36-10.1186/1475-2840-11-36.
Chiang JK, Lai NS, Chang JK, Koo M: Predicting insulin resistance using the triglyceride-to-high-density lipoprotein cholesterol ratio in Taiwanese adults. Cardiovasc Diabetol. 2011, 10: 93-10.1186/1475-2840-10-93.
Hopkins PN, Wu LL, Hunt SC, Brinton EA: Plasma triglycerides and type III hyperlipidemia are independently associated with premature familial coronary artery disease. J Am Coll Cardiol. 2005, 45: 1003-1012. 10.1016/j.jacc.2004.11.062.
Sarwar N, Danesh J, Eiriksdottir G, Sigurdsson G, Wareham N, Bingham S, Boekholdt SM, Khaw KT, Gudnason V: Triglycerides and the risk of coronary heart disease: 10,158 incident cases among 262,525 participants in 29 Western prospective studies. Circulation. 2007, 115: 450-458. 10.1161/CIRCULATIONAHA.106.637793.
Miller M, Stone NJ, Ballantyne C, Bittner V, Criqui MH, Ginsberg HN, Goldberg AC, Howard WJ, Jacobson MS, Kris-Etherton PM, Lennie TA, Levi M, Mazzone T, Pennathur S, American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committee of the Council on Nutrition, Physical Activity, and Metabolism Council on Arteriosclerosis, Thrombosis and Vascular Biology Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease: Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011, 123: 2292-2333. 10.1161/CIR.0b013e3182160726.
Nordestgaard BG, Benn M, Schnohr P, Tybjaerg-Hansen A: Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA. 2007, 298: 299-308. 10.1001/jama.298.3.299.
Bansal S, Buring JE, Rifai N, Mora S, Sacks FM, Ridker PM: Fasting compared with nonfasting triglycerides and risk of cardiovascular events in women. JAMA. 2007, 298: 309-316. 10.1001/jama.298.3.309.
Mackey RH, Greenland P, Goff DC, Lloyd-Jones D, Sibley CT, Mora S: High-Density Lipoprotein Cholesterol and Particle Concentrations, Carotid Atherosclerosis, and Coronary Events: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol. 2012, 60: 508-516. 10.1016/j.jacc.2012.03.060.
Goldenberg I, Boyko V, Tennenbaum A, Tanne D, Behar S, Guetta V: Long-term benefit of high-density lipoprotein cholesterol-raising therapy with bezafibrate: 16-year mortality follow-up of the bezafibrate infarction prevention trial. Arch Intern Med. 2009, 169: 508-514. 10.1001/archinternmed.2008.584.
Manninen V, Elo MO, Frick MH, Haapa K, Heinonen OP, Heinsalmi P, Helo P, Huttunen JK, Kaitaniemi P, Koskinen P, Mäenpää H, Mälkönen M, Mänttäri M, Norola S, Pasternack A, Pikkarainen J, Romo M, Sjöblom T, Nikkilä ES: Lipid alterations and decline in the incidence of coronary heart disease in the Helsinki Heart Study. JAMA. 1988, 260: 641-651. 10.1001/jama.1988.03410050061031.
Hermans MP, Sacks FM, Ahn SA, Rousseau MF: Non-HDL-cholesterol as valid surrogate to apolipoprotein B100 measurement in diabetes: Discriminant Ratio and unbiased equivalence. Cardiovasc Diabetol. 2011, 10: 20-10.1186/1475-2840-10-20.
Natarajan P, Ray KK, Cannon CP: High-density lipoprotein and coronary heart disease: current and future therapies. J Am Coll Cardiol. 2010, 55: 1283-1299. 10.1016/j.jacc.2010.01.008.
Boden WE, Probstfield JL, Anderson T, Chaitman BR, Desvignes-Nickens P, Koprowicz K, McBride R, Teo K, Weintraub W, AIM-HIGH Investigators: Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011, 365: 2255-2267.
Rizos EC, Ntzani EE, Bika E, Kostapanos MS, Elisaf MS: Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: a systematic review and meta-analysis. JAMA. 2012, 308: 1024-1033. 10.1001/2012.jama.11374.
Knopp RH: Drug treatment of lipid disorders. N Engl J Med. 1999, 341: 498-511. 10.1056/NEJM199908123410707.
Tenenbaum A, Fisman EZ, Motro M, Adler Y: Optimal management of combined dyslipidemia: what have we behind statins monotherapy?. Adv Cardiol. 2008, 45: 127-153.
ACCORD Study Group: Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. 2010, 362: 1563-1574.
Tenenbaum A, Fisman EZ: “If it ain’t broke, don’t fix it”: a commentary on the positive–negative results of the ACCORD Lipid study. Cardiovasc Diabetol. 2010, 9: 24-10.1186/1475-2840-9-24.
Scott R, O’Brien R, Fulcher G, Pardy C, D’Emden M, Tse D, Taskinen MR, Ehnholm C, Keech A, Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) Study Investigators: Effects of fenofibrate treatment on cardiovascular disease risk in 9,795 individuals with type 2 diabetes and various components of the metabolic syndrome: the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) study. Diabetes Care. 2009, 32: 493-498. 10.2337/dc08-1543.
The BIP Study Group: Secondary prevention by raising HDL cholesterol and reducing triglycerides in patients with coronary artery disease: the Bezafibrate Infarction Prevention (BIP) study. Circulation. 2000, 102: 21-27.
Manninen V, Tenkanen L, Koskinen P, Huttunen JK, Mänttäri M, Heinonen OP, Frick MH: Joint effects of serum triglyceride and LDL cholesterol and HDL cholesterol concentrations on coronary heart disease risk in the Helsinki Heart Study: implications for treatment. Circulation. 1992, 85: 37-45. 10.1161/01.CIR.85.1.37.
Robins SJ, Collins D, Wittes JT, Papademetriou V, Deedwania PC, Schaefer EJ, McNamara JR, Kashyap ML, Hershman JM, Wexler LF, Rubins HB, VA-HIT Study Group: Relation of gemfibrozil treatment and lipid levels with major coronary events: VA-HIT: a randomized controlled trial. JAMA. 2001, 285: 1585-1591. 10.1001/jama.285.12.1585.
Keech A, Simes RJ, Barter P, Best J, Scott R, Taskinen MR, Forder P, Pillai A, Davis T, Glasziou P, Drury P, Kesäniemi YA, Sullivan D, Hunt D, Colman P, d’Emden M, Whiting M, Ehnholm C, Laakso M, FIELD study investigators: Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005, 366: 1849-1861.
Sacks FM, Carey VJ, Fruchart JC: Combination lipid therapy in type 2 diabetes. N Engl J Med. 2010, 363: 692-694.
Jun M, Foote C, Lv J, Neal B, Patel A, Nicholls SJ, Grobbee DE, Cass A, Chalmers J, Perkovic V: Effects of fibrates on cardiovascular outcomes: a systematic review and meta-analysis. Lancet. 2010, 375: 1875-1878. 10.1016/S0140-6736(10)60656-3.
Meade T, Zuhrie R, Cook C, Cooper J: Bezafibrate in men with lower extremity arterial disease: randomised controlled trial. BMJ. 2002, 325 (7373): 1139-10.1136/bmj.325.7373.1139.
Khazaei M, Salehi E, Rashidi B: Pan-PPAR agonist, bezafibrate, restores angiogenesis in hindlimb ischemia in normal and diabetic rats. Int J Pept. 2012, 2012: 637212.
Harrold BP, Marmion VJ, Gough KR: A double-blind controlled trial of clofibrate in the treatment of diabetic retinopathy. Diabetes. 1969, 18: 285-391.
Duncan LJ, Cullen JF, Ireland JT, Nolan J, Clarke BF, Oliver MF: A three-year trial of atromid therapy in exudative diabetic retinopathy. Diabetes. 1968, 17: 458-467.
Hermans MP: Non-invited review: prevention of microvascular diabetic complications by fenofibrate: lessons from FIELD and ACCORD. Diab Vasc Dis Res. 2011, 8: 180-189. 10.1177/1479164111407783.
Kim J, Ahn JH, Kim JH, Yu YS, Kim HS, Ha J, Shinn SH, Oh YS: Fenofibrate regulates retinal endothelial cell survival through the AMPK signal transduction pathway. Exp Eye Res. 2007, 84: 886-893. 10.1016/j.exer.2007.01.009.
Tenenbaum A, Motro M, Fisman EZ: Dual and pan-peroxisome proliferator-activated receptors (PPAR) co-agonism: the bezafibrate lessons. Cardiovasc Diabetol. 2005, 4: 14-10.1186/1475-2840-4-14.
Willson TM, Brown PJ, Sternbach DD, Henke BR: The PPARs: from orphan receptors to drug discovery. J Med Chem. 2000, 43: 527-550. 10.1021/jm990554g.
Tenenbaum A, Fisman EZ, Boyko V, Benderly M, Tanne D, Haim M, Matas Z, Motro M, Behar S: Attenuation of progression of insulin resistance in patients with coronary artery disease by bezafibrate. Arch Intern Med. 2006, 166: 737-741. 10.1001/archinte.166.7.737.
Ogawa S, Takeuchi K, Sugimura K, Fukuda M, Lee R, Ito S, Sato T: Bezafibrate reduces blood glucose in type 2 diabetes mellitus. Metabolism. 2000, 49: 331-334. 10.1016/S0026-0495(00)90176-8.
Tenenbaum H, Behar S, Boyko V, Adler Y, Fisman EZ, Tanne D, Lapidot M, Schwammenthal E, Feinberg M, Matas Z, Motro M, Tenenbaum A: Long-term effect of bezafibrate on pancreatic beta-cell function and insulin resistance in patients with diabetes. Atherosclerosis. 2007, 194: 265-271. 10.1016/j.atherosclerosis.2006.08.005.
Teramoto T, Shirai K, Daida H, Yamada N: Effects of bezafibrate on lipid and glucose metabolism in dyslipidemic patients with diabetes: the J-BENEFIT study. Cardiovasc Diabetol. 2012, 11: 29-10.1186/1475-2840-11-29.
Hiuge A, Tenenbaum A, Maeda N, Benderly M, Kumada M, Fisman EZ, Tanne D, Matas Z, Hibuse T, Fujita K, Nishizawa H, Adler Y, Motro M, Kihara S, Shimomura I, Behar S, Funahashi T: Effects of peroxisome proliferator-activated receptor ligands, bezafibrate and fenofibrate, on adiponectin level. Arterioscler Thromb Vasc Biol. 2007, 27: 635-644. 10.1161/01.ATV.0000256469.06782.d5.
Tenenbaum A, Motro M, Fisman EZ, Schwammenthal E, Adler Y, Goldenberg I, Leor J, Boyko V, Mandelzweig L, Behar S: Peroxisome proliferator-activated receptors ligand bezafibrate for prevention of type 2 diabetes mellitus in patients with coronary artery disease. Circulation. 2004, 109: 2197-2202. 10.1161/01.CIR.0000126824.12785.B6.
Tenenbaum A, Motro M, Fisman EZ, Adler Y, Shemesh J, Tanne D, Leor J, Boyko V, Schwammenthal E, Behar S: Effect of bezafibrate on incidence of type 2 diabetes mellitus in obese patients. Eur Heart J. 2005, 26: 2032-2038. 10.1093/eurheartj/ehi310.
Flory JH, Ellenberg S, Szapary PO, Strom BL, Hennessy S: Antidiabetic action of bezafibrate in a large observational database. Diabetes Care. 2009, 32: 547-551. 10.2337/dc08-1809.
Tenenbaum A, Motro M, Fisman EZ, Tanne D, Boyko V, Behar S: Bezafibrate for the secondary prevention of myocardial infarction in patients with metabolic syndrome. Arch Intern Med. 2005, 165: 1154-1160. 10.1001/archinte.165.10.1154.
Sano K, Nakamura T, Hirano M, Kitta Y, Kobayashi T, Fujioka D, Saito Y, Yano T, Watanabe K, Watanabe Y, Mishina H, Obata JE, Kawabata K, Kugiyama K: Comparative study of bezafibrate and pravastatin in patients with coronary artery disease and high levels of remnant lipoprotein. Circ J. 2010, 74: 1644-1650. 10.1253/circj.CJ-10-0079.
Heart Protection Study Collaborative Group: MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002, 360: 7-22.
Sacks FM, Tonkin AM, Shepherd J, Braunwald E, Cobbe S, Hawkins CM, Keech A, Packard C, Simes J, Byington R, Furberg CD, for the Prospective Pravastatin Pooling Project: Effect of pravastatin on coronary disease events in subgroups defined by coronary risk factors. Circulation. 2000, 102: 1893-1900. 10.1161/01.CIR.102.16.1893.
Ballantyne CM, Herd JA, Ferlic LL, Dunn JK, Farmer JA, Jones PH, Schein JR, Gotto AM: Influence of low HDL on progression of coronary artery disease and response to fluvastatin therapy. Circulation. 1999, 99: 736-743. 10.1161/01.CIR.99.6.736.
Scandinavian Simvastatin Survival Study Group: Baseline serum cholesterol and treatment effect in the Scandinavian Simvastatin Survival Study (4S). Lancet. 1995, 345: 1274-1275.
The Long-Term Intervention With Pravastatin in Ischaemic Disease (LIPID) Study Group: Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998, 339: 1349-1357.
Pfeffer MA, Sacks FM, Moyé LA, East C, Goldman S, Nash DT, Rouleau JR, Rouleau JL, Sussex BA, Theroux P, Vanden Belt RJ, Braunwald E: Influence of baseline lipids on effectiveness of pravastatin in the CARE trial. J Am Coll Cardiol. 1999, 33: 125-130. 10.1016/S0735-1097(98)00522-1.
Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, MacFarlane PW, McKillop JH, Packard CJ: Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med. 1995, 333: 1301-1307. 10.1056/NEJM199511163332001.
Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, Langendorfer A, Stein EA, Kruyer W, Gotto AM: Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. JAMA. 1998, 279: 1615-1622. 10.1001/jama.279.20.1615.
Chapman MJ, Redfern JS, McGovern ME, Giral P: Optimal pharmacotherapy to combat the atherogenic lipid triad. Curr Opin Cardiol. 2011, 26: 403-411. 10.1097/HCO.0b013e32834965e9.
Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, Joyal SV, Hill KA, Pfeffer MA, Skene AM: Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 Investigators: intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004, 350: 1495-1504. 10.1056/NEJMoa040583.
de Lemos JA, Blazing MA, Wiviott SD, Lewis EF, Fox KA, White HD, Rouleau JL, Pedersen TR, Gardner LH, Mukherjee R, Ramsey KE, Palmisano J, Bilheimer DW, Pfeffer MA, Califf RM, Braunwald E, A to Z Investigators: Early intensive vs. a delayed conservative simvastatin strategy in patients with acute coronary syndromes: phase Z of the A to Z trial. JAMA. 2004, 292: 1307-1316. 10.1001/jama.292.11.1307.
LaRosa JC, Grundy SM, Waters DD, Shear C, Barter P, Fruchart JC, Gotto AM, Greten H, Kastelein JJ, Shepherd J, Wenger NK: Treating to New Targets (TNT) Investigators: intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med. 2005, 352: 1425-1435. 10.1056/NEJMoa050461.
Pedersen TR, Faergeman O, Kastelein JJ, Olsson AG, Tikkanen MJ, Holme I, Larsen ML, Bendiksen FS, Lindahl C, Szarek M, Tsai J, Incremental Decrease in End Points Through Aggressive Lipid Lowering (IDEAL) Study Group: High-dose atorvastatin vs. usual-dose simvastatin for secondary prevention after myocardial infarction: the IDEAL study: a randomized controlled trial. JAMA. 2005, 294: 2437-2445. 10.1001/jama.294.19.2437.
Armitage J, Bowman L, Wallendszus K, Bulbulia R, Rahimi K, Haynes R, Parish S, Peto R, Collins R, Study of the Effectiveness of Additional Reductions in Cholesterol and Homocysteine (SEARCH) Collaborative Group: Intensive lowering of LDL cholesterol with 80 mg versus 20 mg simvastatin daily in 12,064 survivors of myocardial infarction: a double-blind randomised trial. Lancet. 2010, 376: 1658-1669. 10.1016/S0140-6736(10)60310-8.
Cannon CP, Steinberg BA, Murphy SA, Mega JL, Braunwald E: Meta-analysis of cardiovascular outcomes trials comparing intensive versus moderate statin therapy. J Am Coll Cardiol. 2006, 48: 438-445. 10.1016/j.jacc.2006.04.070.
Wagstaff LR, Mitton MW, Arvik BM, Doraiswamy PM: Statin-associated memory loss: analysis of 60 case reports and review of the literature. Pharmacotherapy. 2003, 23: 871-880. 10.1592/phco.23.7.871.32720.
Muldoon MF, Ryan CM, Sereika SM, Flory JD, Manuck SB: Randomized trial of the effects of simvastatin on cognitive functioning in hypercholesterolemic adults. Am J Med. 2004, 117: 823-829. 10.1016/j.amjmed.2004.07.041.
Culver AL, Ockene IS, Balasubramanian R, Olendzki BC, Sepavich DM, Wactawski-Wende J, Manson JE, Qiao Y, Liu S, Merriam PA, Rahilly-Tierny C, Thomas F, Berger JS, Ockene JK, Curb JD, Ma Y: Statin use and risk of diabetes mellitus in postmenopausal women in the Women’s Health Initiative. Arch Intern Med. 2012, 172: 144-152. 10.1001/archinternmed.2011.625.
Jones PH, Davidson MH: Reporting rate of rhabdomyolysis with fenofibrate + statin versus gemfibrozil + any statin. Am J Cardiol. 2005, 95: 120-122. 10.1016/j.amjcard.2004.08.076.
Fruchart JC, Sacks F, Hermans MP, Assmann G, Brown WV, Ceska R, Chapman MJ, Dodson PM, Fioretto P, Ginsberg HN, Kadowaki T, Lablanche JM, Marx N, Plutzky J, Reiner Z, Rosenson RS, Staels B, Stock JK, Sy R, Wanner C, Zambon A, Zimmet P: The Residual Risk Reduction Initiative: a call to action to reduce residual vascular risk in patients with dyslipidemia. Am J Cardiol. 2008, 102: 1K-34K. 10.1016/j.amjcard.2008.10.002.
Farnier M: Combination Therapy with an HMG-CoA Reductase Inhibitor and a Fibric Acid Derivative: a Critical Review of Potential Benefits and Drawbacks. Am J Cardiovasc Drugs. 2003, 3: 169-178. 10.2165/00129784-200303030-00003.
Shek A, Ferrill MJ: Statin-fibrate combination therapy. Ann Pharmacother. 2001, 35: 908-917.
Prueksaritanont T, Tang C, Qui Y, Mu L, Subramanian R, Lin JH: Effects of fibrates on metabolism of statins in human hepatocytes. Drug Metab Dispos. 2002, 30: 1280-1287. 10.1124/dmd.30.11.1280.
Backman JT JT, Kyrklund C, Kivistö KT, Wang JS, Neuvonen PJ: Plasma concentrations of active simvastatin acid are increased by gemfibrozil. Clin Pharmacol Ther. 2000, 68: 122-129. 10.1067/mcp.2000.108507.
Kyrklund C, Backman JT, Kivistö KT, Neuvonen M, Laitila J, Neuvonen PJ: Plasma conentrations of active lovastatin acid are markedly increased by gemfibrozil but not by bezafibrate. Clin Pharmacol Ther. 2001, 69: 340-345. 10.1067/mcp.2001.115542.
Kehely A, MacMahon M, Barbir M, Wray R, Hunt BJ, Prescott RJ, Thompson GR: Combined bezafibrate and simvastatin treatment for mixed hyperlipidaemia. QJM. 1995, 88: 421-427.
Gavish D, Leibovitz E, Shapira I, Rubinstein A: Bezafibrate and simvastatin combination therapy for diabetic dyslipidaemia: efficacy and safety. J Intern Med. 2000, 247: 563-569. 10.1046/j.1365-2796.2000.00646.x.
Bergman AJ, Murphy G, Burke J, Zhao JJ, Valesky R, Liu L, Lasseter KC, He W, Prueksaritanont T, Qiu Y, Hartford A, Vega JM, Paolini JF: Simvastatin does not have a clinically significant pharmacokinetic interaction with fenofibrate in humans. J Clin Pharmacol. 2004, 44: 1054-1062. 10.1177/0091270004268044.
Madrid-Miller A, Moreno-Ruiz LA, Borrayo-Sánchez G, Almeida-Gutiérrez E, Martínez-Gómez DF, Jáuregui-Aguilar R: Impact of bezafibrate treatment in patients with hyperfibrinogenemia and ST-elevation acute myocardial infarction: a randomized clinical trial. Cir Cir. 2010, 78: 229-237.
Tenenbaum A, Medvedofsky D, Fisman EZ, Bubyr L, Matetzky S, Tanne D, Klempfner R, Shemesh J, Goldenberg I: Cardiovascular events in patients received combined fibrate/statin treatment versus statin monotherapy: Acute Coronary Syndrome Israeli Surveys data. PLoS One. 2012, 7 (4): e35298-10.1371/journal.pone.0035298.
Acknowledgments
This work was supported in part by the Cardiovascular Diabetology Research Foundation (RA 58-040-684-1), Holon, Israel.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
AT received speaker fee and travel expenses support from Abbott, Tribute, Novartis and Merck. EZF declares that he has no competing interests.
Authors’ contribution
Both authors have equally contributed in the conception and drafting of the manuscript. Both authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Tenenbaum, A., Fisman, E.Z. Fibrates are an essential part of modern anti-dyslipidemic arsenal: spotlight on atherogenic dyslipidemia and residual risk reduction. Cardiovasc Diabetol 11, 125 (2012). https://doi.org/10.1186/1475-2840-11-125
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2840-11-125