
Abstract
Background
Women report more occupational ill-health and are more sick-listed than men. Exploration of women's working conditions would therefore seem to be valuable. In this study we investigated the prevalence of work-related stress and its association with self-perceived health and sick-leave in a population of employed, working Swedish women.
Methods
This cross-sectional population study comprised 424 employed, working women who answered questionnaires on work-related stress, self-perceived health and sick-leave. The odds ratio (OR) with 95% confidence interval (CI) was calculated in order to analyse the association between the exposure variables of work-related stress and outcome variables of ill-health symptoms, self-rated health and sick-leave.
Results
Ten percent of the group reported high perceived stress owing to indistinct organisation and conflicts, and 25% high perceived stress owing to individual demands and commitment. Twenty-two percent reported low influence at work and 33% reported work interference with leisure time. All categories of overall work-related stress were significantly associated with increased odds of high level of illness symptoms, with the highest OR for high perceived stress owing to indistinct organisation and conflicts and high perceived stress owing to individual demands and commitment with an OR of 3.17 (CI = 1.51–6.62) and 4.53 (CI = 2.71–7.56) respectively. High perceived stress owing to indistinct organisation and conflicts and low influence at work were significantly associated with sick-leave with an OR of 3.85 (CI = 1.59–9.30) and 2.54 (CI = 1.17–5.48) respectively.
Conclusion
This study showed an association between, on the one hand, work-related stress, and on the other hand, illness symptoms and sick-leave. Distinguishing between the occurrence of negative work characteristics, and the immediate perception of stress because of these, resulted in a broad view of women's working conditions and expanded knowledge of work-related stress in women.
Similar content being viewed by others


Background
Work characteristics such as insufficient leadership, injustice at work and poor organisational climate have been linked to sickness absence in both women and men [1–3]. Furthermore, high demands, low control and low social support have, in several studies, been found to increase the risk of sickness absence and musculoskeletal and psychiatric disorders [4–7]. Increased workload with perceived high psychological and physical demands has been connected to symptoms of illness, as well as to sick-leave, and this is more pronounced in women [6, 6–9]. Physical and mental demands greater than own capacity and high work stress combined with lack of control over working hours constituted a risk of sick-leave among women [8, 10]. Person-related characteristics, such as over-commitment, strenuous effort at work and low self-efficacy, have also been associated with poor health perception and sick-leave [11, 12]. Even though we know that different work-related factors influence health and sick-leave outcomes, little research has focused on the prevalence of work-related stress in a general working population of women.
During the 1990s the rate of sick-leave increased dramatically in Sweden, but has somewhat decreased in the last few years. The costs for early retirement pensions, however, have increased and over half a million people are on disability pension. Women account for the majority of sick-leave as well as early retirement pension [13, 14]. In just a few years the proportion of psychiatric sickness certification diagnoses has risen from 18% to over 30% on sickness certificates. Diagnoses of depression, stress reactions and anxiety syndromes show the greatest increase [13, 14]. Large reductions in private as well as public funding have resulted in increased workload, with a greater risk of sick-leave [14, 15]. In the same period of time the psychosocial work environment has deteriorated, i.e. stressful work, work demands and work pace have increased, and the effect is especially pronounced in women [13, 14]. Women also report a decline in health with more fatigue and musculoskeletal pain than men [14]. In Sweden, women and men are to a large extent concentrated in different sectors of the labour market [16]. They might therefore be exposed in different ways and to different degrees to work-related stress. Consequently, it is important to explore women's working situation further.
In a qualitative, explorative study [17] women on sick-leave owing to work-related strain described the gradual road to sickness absence as a process going from controlling everyday life, to total loss of control of working and private life. At work, both environmental and personal factors contributed to the process. The women described the work situation as strained, and they suffered from lack of organisational clarity, little influence and unsolved conflicts. The participants saw themselves as people with high demands on their capacity, strong sense of responsibility and having difficulties setting limits. This combination of work-related factors and personal characteristics led to loss of control and sick-leave. Based on that study a questionnaire was developed with the purpose of assessing the perceived stress dimension in relation to these environmental and personal factors [18]. To determine the need for preventative steps decreasing the development of sick-leave in women it is of some importance to find out how common work-related stress is in a general population of women, and to obtain more knowledge about the relationship between women's work-related stress and their health perception and sick-leave. To our knowledge, there are few studies on the prevalence of work-related stress in women. The aim of the present study was to investigate the prevalence of work-related stress and its association with self-perceived health and sick-leave in a general population of employed, working women aged thirty-eight or fifty.
Methods
Research design and population
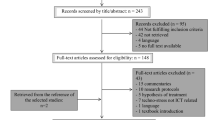
This cross-sectional study of women aged thirty-eight and fifty was part of a longitudinal population based study – 'The Population Study of Women in Gothenburg, Sweden'. The two-cohort design has been aimed to capture two important stages in women's life. Cohort comparisons have been carried out in 1968–69, 1980–81, 1992–93 and 2004–05 [19]. In the latest study, stretching from October 2004 to April 2005, a random sample of 38-year-old and 50-year-old women registered for census purposes in Gothenburg was identified and invited to participate in a free health examination. Additionally, 85 participants aged 38 in the 1992–93 cohort, and who in 2004–05 were 50 years old, were invited. In all, 846 women were asked to participate (7 were excluded owing to difficulties in speaking and understanding Swedish) (Table 1). The external drop-outs were 339, of whom 191 declined or did not turn up and 148 could not be contacted (participation rates 60% and 58% respectively). In total, 500 women accepted and participated in the study (Table 1) [20].
Inclusion criteria for the present cross-sectional study were employed or self-employed women. Four hundred and thirty-three women of the sample fulfilled these criteria. Of these, nine women did not complete the work stress questionnaire and dropped out. In all, 424 women participated in the present study (Table 1). The study was approved by the Ethics Committee, University of Gothenburg, Sweden.
Procedure
The participants went through a half-day health examination which included an interview, questionnaires, physical examinations, measurements and blood tests [20]. At the end of the health examination all participants received a questionnaire designed for the present study and a stamped addressed envelope in which to return the completed questionnaire. Two reminders were given by telephone at two-week intervals.
Exposure variables
Work characteristics and perceived stress
The instrument used was the Work Stress Questionnaire, developed from the qualitative study described above [17, 18]. Two main themes were identified. One was related to factors at work and the other to the persons themselves. Categories were recognized and questions were constructed. The self-assessed instrument consists of 21 main questions grouped into four categories: indistinct organisation and conflicts and individual demands and commitment contain 7 questions respectively and answers to these questions are Yes, Partly and No; influence at work and work interference with leisure time contain 4 and 3 questions respectively and answers are given on a four-point ordinal scale – Yes, always, Yes, rather often, No, seldom and No, never. Each of the questions in the categories indistinct organisation and conflicts and individual demands and commitment has an appended question 'Do you perceive it as stressful?' Answers to this question are given on a four-point ordinal scale – Not at all stressful, Less stressful, Stressful and Very stressful. These were grouped into two categories of perceived stress owing to work characteristics: perceived stress owing to indistinct organisation and conflicts (7 questions) and perceived stress owing to individual demands and commitment (7 questions). The reliability of the questionnaire was tested in a test-retest study by a non-parametric statistical method for evaluation of paired data. The test values were close to zero throughout, which indicates a high level of reliability [18]. The items were evaluated by a pilot group, representing the questionnaire's target group, who agreed to face validity of the questions and their content [18].
Definition of overall work-related stress
Overall work-related stress was defined as follows: Confirmatory answers of the items within the category indistinct organisation and conflicts and individual demands and commitment were counted for every participant. In order to find enough exposure differences, without having to compare the extremes, we chose to dichotomise at the upper quartile. For indistinct organisation and conflicts (7 questions), high level of exposure was defined as confirmatory answers to 4–7 items and low level of exposure was defined as confirmatory answers to 0–3 items. For individual demands and commitment (7 questions), the cut-off for high level was 7 items and low level 0–6 items. Each participant's median response category of the four questions in influence at work was calculated and then dichotomised into high influence (always or often) and low (never or seldom). The median response category of the three questions in work interference with leisure time for each participant was calculated and then dichotomised into low (never or seldom) and high (always or often). Further, each participant's median response category of the seven questions respectively in perceived stress owing to indistinct organisation and conflicts and in perceived stress owing to individual demands and commitment was calculated and then dichotomised into low stress perception (defined as no confirmation of perceived stress, not stressful or less stressful), and high stress perception (confirmatory answers to stressful or very stressful).
Test of validity
The exposure variables as defined above were validated against a question about general experienced stress. This was the only question about stress in the study of 'The Population Study of Women in Gothenburg, Sweden' and had earlier been used in these longitudinal surveys [19]. The question was: 'Have you experienced any period of stress during a longer period of time, i.e. a month or more? The word stress implies that you have been irritable, tense, nervous, anxious or sleepless in relation to work, health, family or in relation to conflicts in these areas or in relation to something else'. Six possible statements were given on an ordinal scale: have never experienced any period of stress, have experienced period of stress but not the last 5 years, have experienced period of stress the last 5 years, have experienced several periods of stress the last 5 years, lived with constant stress the last year, lived with constant stress the last 5 years. The answers were dichotomised into low stress experience ('have never experienced stress' to 'have experienced a period of stress in the last 5 years) and high stress experience ('have experienced several periods of stress' to 'lived with constant stress for the last 5 years').
The six categories of work-related stress were all significantly associated with the question about general experienced of stress. The highest OR were high perceived stress owing to indistinct organisation and conflicts and high perceived stress owing to individual demands and commitment with an OR of 4.16 (1.92–9.00) and 3.98 (2.42–6.54), respectively – not presented in any table.
Outcome variables
Self-rated symptoms
Self-rated symptoms were assessed by one question: 'Have you, during the last 3 months, been troubled by any of the symptoms listed?' Thirty different mental and physical symptoms were listed and two possible statements were given: Yes or No. Each participant's number of stated symptoms was counted and dichotomised according to median cut: high level of self-rated symptoms was defined as 8 or more stated symptoms. This question has been used in the longitudinal survey of 'The Population Study of Women in Gothenburg, Sweden' [19, 21].
Self-rated health
Self-rated health was assessed by the statement: 'In general, would you state your health as being ...'. Answers were given on a five-point ordinal scale – Excellent, Very good, Good, Fair and Bad. Self-rated health has been shown to be a good indicator of health, predicting morbidity and mortality in prospective studies [22]. Poor self-rated health was dichotomised into poor (Fair/Bad) and good (Excellent/Very good/Good). Since only a small group (n = 48) assessed poor self-rated health, we chose to include a salutogenic perspective and assessed the associations with good self-rated health, which was defined and dichotomised into good (Excellent/Very good) and poor (Good/Fair/Bad).
Sick-leave
Self-reported sick-leave was assessed by the questions: 'Are you on sick-leave at the moment?', 'To what degree?' and 'For how long have you been sick-listed? State the number of weeks'. These questions were not validated. Voss et al [23] found, however, the agreement between self-reported and registered data on sick-leave good.
Statistics
Descriptive statistics of work-related stress were calculated. The chi-squared and Fisher's two-tailed exact test were used to test differences in the proportions between groups; age-group (38-year-old/50-year-old), educational level (>12 years/10–12 years, ≤ 9 years), occupational class (manager, high and middle level non-manual/low level non-manual, manual), employer (private, self-employed, combined/public) and sick-leave/no sick-leave. The odds ratio (OR) with 95% confidence intervals (CI) was calculated in order to analyse the association between the exposure variables of work-related stress and outcome variables of sick-leave, self-rated health and symptoms of illness. The OR was also used to validate the exposure variable against the question about general experienced stress. The logistic regression models were used to adjust for age-group, educational level, occupational class and employer.
Results
Demography and distribution of exposure differences
A significantly larger proportion of the 50-year-old women were public employees (p < 0.001). A majority had professions characterised as high or middle level non-manual occupation. Thirty participants were on sick-leave and sick-leave spells had a range from less than 1 month to over 4 years. Of those on full-time sick-leave all but one had been on sick-leave <2 months. A significantly larger proportion of those on sick-leave belonged to the age group of 50-year-olds (p < 0.006) (Table 2).
No differences were found between age groups concerning exposure to work-related stress. The proportion who reported a high level of work interference with leisure time was, however, significantly larger among individuals with a high education level (p = 0.03), higher occupational class (p = 0.03) and private employment (p = 0.04). The proportion of high indistinct organisation and conflicts was larger among public employees (p = 0.01) and high individual demands and commitment was larger among higher occupational class (p = 0.01). A larger proportion among those on sick-leave reported low influence at work (p = 0.02) and high perceived stress owing to indistinct organisation and conflicts (p = 0.01) – data not shown.
Prevalence of work characteristics and perceived stress
The prevalence of the three most reported work characteristics in indistinct organisation and conflicts was increased work-load (66%), conflicts at work (65%) and involved in conflicts at work (35%). The three most reported characteristics in individual demands and commitment were putting high demands on oneself at work, being engaged in one's work and thinking about work after the working day with 93, 94 and 92% respectively. In influence at work 29% reported difficulties in influencing decisions and 25% reported difficulties in deciding the working pace. The prevalence of work characteristics in work interference with leisure time was approximately 30% for the three items (Table 3).
The prevalence of the three most reported items in perceived stress owing to indistinct organisation and conflicts was 38% for increased workload, 23% for conflicts at work and 17% for reporting stress because of supervisors not solving the conflicts. Most prevalent items in perceived stress owing to individual demands and commitment were stress owing to hard to set limits with a prevalence of 44%, high demands on oneself at work, 29% and high responsibility for one's work, 29% (Table 4).
Prevalence of overall work-related stress
The overall work-related stress was, as described in the method section, grouped into four categories of work characteristics and two categories of perceived stress owing to work characteristics. Twenty-nine percent reported a high level of exposure caused by indistinct organisation and conflicts and 26% a high level caused by individual demands and commitment. Ten percent of the entire group reported high perceived stress owing to indistinct organisation and conflicts and 25% high perceived stress owing to individual demands and commitment. Twenty-two percent stated low Influence at work and 33% work interference with leisure time (Table 5).
Associations between overall work-related stress and outcome variables
All categories of work-related stress were significantly associated with increased odds of high level ill-health symptoms, with the highest OR for high perceived stress owing to indistinct organisation and conflicts and perceived stress owing to individual demands and commitment with an OR of 3.17 (1.51–6.62) and 4.53 (2.71–7.56), respectively. High individual demands and commitment and perceived stress owing to individual demands and commitment were significantly associated with Poor self-rated health with an OR of 2.50 (1.34–4.62) and 2.64 (1.42–4.91), respectively. The OR for high levels of exposure was low for those with a Good self-rated health. High perceived stress owing to indistinct organisation and conflicts and low influence at work was significantly associated with sick-leave with an OR of 3.85 (CI = 1.59–9.30) and 2.54 (CI = 1.17–5.48), respectively. After adjustments for age, education, occupation and employer, OR remained almost unaltered and significant in all categories (Table 5).
Discussion
The aim of the present study was to investigate the prevalence of different types of work-related stress and its association with self-perceived health and sick-leave in a population of employed, working women aged thirty-eight or fifty years. The most common type of work-related stress was due to work interference with leisure time, followed by stress due to low influence at work, high perceived stress owing to indistinct organisation and conflicts and high perceived stress owing to individual demands and commitment. We also found a high prevalence of several specific work characteristics. Items in the category concerning individual demands and commitment showed the highest occurrence. The prevalence of perceived stress owing to certain work characteristics was, however, lower, although perceived stress owing to increased workload and hard-to-set limits had a prevalence of around 40% each. These findings of perceived stress can appear rather low in comparison with other studies, though. In a European report from 2000, 29% of female employees in Europe reported stress related to work [24]. One explanation of this disparity could be differences in measuring the exposure variables. The questionnaire in this study assesses not only the occurrence of work characteristics but also the immediate perception of the characteristics' stressfulness, i.e. if the characteristic is perceived as stressful or not. This study distinguishes between the occurrence of negative work characteristics and the perception of stress owing to these characteristics.
The European report also found that the prevalence varied between different occupations. Professionals reported highest stress, 40% compared with 17% in elementary occupations [24]. Two British studies, one of head teachers and one of police officers, found the prevalence of self-reported work-related stress to be 43 and 41% respectively [25, 26]. We found few differences, however, between occupational classes, except for high individual demands and commitment where the prevalence was higher among the higher occupational classes. Furthermore, female head teachers reported more stress than male, and in both studies workload was a main stressor [25, 26]. Correspondingly, in our study the prevalence of increased workload was high with high perceived stress as a result. Research finds that high workload constitutes a risk of ill-health perception and sickness absence [6–8, 27].
It is notable that the prevalence of high perceived stress owing to individual demands and commitment was higher than for perceived stress owing to indistinct organisation and conflicts. Twenty-five percent reported high perceived stress owing to individual demands and commitment. High dedication to work and difficulties in managing the work situation seem to result in a high amount of stress. The issue is whether the occurrence of perceived stress will result in negative consequences or not. Some studies have linked over-commitment to a higher risk of poor health [11, 28] and ill-health perception has been associated with sickness absence [29–31]. High effort and low reward, the so-called effort-reward imbalance, were also shown to have an adverse effect on self-reported health in a European comparative study [32]. In our earlier mentioned qualitative study, women sick-listed owing to work-related strain described putting high demands on themselves, having a high sense of responsibility and difficulty in setting limits as contributory factors in being put on sick-leave [17]. Perceived stress owing to individual demands and commitment may therefore have consequences for health outcomes and sick-leave.
Work-related stress and associations with sick-leave
The prevalence of high influence at work was 78%. Likewise, the prevalence of low perceived stress owing to indistinct organisation and conflicts was as high as 90%. This was unexpected, since several studies point to a deterioration of work conditions, especially in women [13, 14, 24]. On the other hand, those reporting low influence at work and high perceived stress owing to indistinct organisation and conflicts had an increased probability of sick-leave, with an OR of 2.54 and 3.85 respectively. These connections correspond to several other findings linking low influence at work and work-related stress to an increased risk of sickness absence [1–4, 9, 31]. One might also have expected associations between the four other categories of work-related stress. To our knowledge, however, few studies have linked individual demands and commitment to sickness absence. Over-commitment has been related to vital exhaustion, low mental health and sleep disturbance, though [11, 28, 33]. The phenomenon of sickness absence is complex and needs to be understood in a broad context, on societal as well as organisational and individual levels [34, 35].
Work-related stress and associations with self-perceived health
In this study an association between on the one hand all the categories of overall work-related stress, and on the other hand a high level of self-rated symptoms was also found. Women reporting high perceived stress owing to organisation and conflicts and high perceived stress owing to individual demands and commitment had an increased probability of having a high level of self-rated symptoms with an OR of 3.17 and 4.53 respectively. This corresponds with earlier research where different work characteristics were associated with ill-health perceptions [6, 7, 11, 28, 29, 31]. Correspondence between work-related stress and poor self-rated health was only found, however, in two of the six categories with the strongest association with perceived stress owing to individual demands and commitments having an OR of 2.64. Low reported work-related stress was, however, associated with good self-rated health. All of the significant associations between the exposure and outcome variables remained after adjustment for the confounders of age groups, educational level, occupational class, employer and sick-leave.
Work interference with leisure time was reported by 33% of the participants, and high level of interference was associated with a high level of self-rated symptoms having an OR of 2.07. Something to bear in mind is that women are part of the paid work force approximately to the same extent as men, with a participation rate of 80% to men's 86% [36]. At the same time unpaid work, such as household duties and childcare, has not decreased and women contribute the most to these chores [36, 37]. In a study of white-collar women and men, women reported a higher total workload, including paid and unpaid work, more stress and higher severity of symptoms than men [38]. Work-family conflict has been found to constitute a risk of sickness absence in both women and men. It is most pronounced, however, and with poorer health outcomes, among women [39].
Socio-demographic differences
Unexpectedly, we found few differences between the two age groups. A greater proportion of the 50-year-olds was sick-listed and in public employment, but no differences regarding exposure to work-related stress were shown. Some diversity was found among different occupational classes, educational levels and employment in relation to work-related stress exposure, though. Work interference with leisure time seems to be the category that differs the most between the groups. This is consistent with earlier findings where professionals perceive more stress than others [31] and also point out workload and work-family interference as main stressors [25]. More public than private employees found indistinct organisation and conflicts to be high. This may be explained by the large staff reductions and reorganisations in the public sector during the nineties, with higher workload for the retained staff as a consequence [14]. The lack of employment differences, i.e. between public and private employees regarding the exposure to work-related stress, could be explained by the occupational gender segregation which puts women in subordinate positions in the public as well as the private sector. In Sweden in general, three out of four managers are men; four out of five in the private sector [36]. Women appear to have less control at work than men and so-called active jobs (high control and high demands) constitute a risk for women, as opposed to men [9, 29].
Methodological considerations
This study had a cross-sectional design and no conclusions regarding causality can be made. Previous research, however, supports the finding that being exposed to work-related stress increases the risk of symptoms of illness and sick-leave [4, 6–8, 29]. Studies based on self report measures can be influenced by several factors, such as recall bias, socially desirable answers and exposure suspicion bias. It is therefore essential to interpret the results with caution. In this particular study we do not think that these possible sources of bias only follow one direction, i.e. towards overestimation. From clinical experience it is not uncommon that individuals exposed to severe stress underestimate the sources of stress in their lives. It is notable that some statistically significant values of the confidence interval of OR were wide and therefore the results have to be treated with caution. One possible limitation of the study was that the exposure variables were assessed with a recently-developed questionnaire. It has been found to have high reliability and face validity, but further research is required to ensure its validity. In this study, the validity was tested and correspondence was found between all categories of work-related stress and general stress experienced. Some of the items had a low prevalence and should perhaps have been considered for omission. The grouping of the items in different categories of work-related stress was, however, based on empirical findings in a qualitative study [17] and, since this questionnaire is still under development, we decided to let the items remain. Despite its limitations, the Work Stress Questionnaire has shown new ways of assessing work-related stress. The advantages with this questionnaire lie both in the design, which combines environmental and personal work characteristics, and in the quality of assessments of the experience of perceived stress in relation to each specific item.
As regards selection bias, the education level was higher (>12 years = 55%) in the study population than in the general population of women in Gothenburg in 2004 (>12 years = 44%) [40]. The study population, however, is not completely comparable with the general population, since only employed women were included. The general population also includes, for example, women who have not yet entered the labour market and unemployed women presumed to have a lower educational level. The sickness absence rate was somewhat higher in the study population (7%) than in the general female population of 2004 (5.6%) [36]. This can be explained by the higher representation of 50-year-olds.
Conclusion
In order to devise preventative steps, it is important to identify individuals at risk of symptoms of illness and sickness absence owing to work-related stress. This study showed an association between on one hand work-related stress, and on the other, self-rated symptoms and sick-leave in employed, working women aged 38 or 50. By using the Work Stress Questionnaire that distinguishes between the occurrence of a negative work characteristic and the immediate perception of stress owing to the characteristic, we get a broader view of women's working conditions and an expanded knowledge of work-related stress in women. These findings imply that work-related stress among a general population of Swedish middle-aged employed women is an important public health issue.
References
Kivimaki M, Elovainio M, Vahtera J, Ferrie JE: Organisational justice and health of employees: prospective cohort study. Occup Environ Med. 2003, 60 (1): 27-33. 10.1136/oem.60.1.27. discussion 33-4.
Vaananen A, Kalimo R, Toppinen-Tanner S, Mutanen P, Peiro JM, Kivimaki M, et al: Role clarity, fairness, and organizational climate as predictors of sickness absence: a prospective study in the private sector. Scand J Public Health. 2004, 32 (6): 426-34. 10.1080/14034940410028136.
Head J, Kivimaki M, Siegrist J, Ferrie JE, Vahtera J, Shipley MJ, et al: Effort-reward imbalance and relational injustice at work predict sickness absence: the Whitehall II study. J Psychosom Res. 2007, 63 (4): 433-40. 10.1016/j.jpsychores.2007.06.021.
North FM, Syme SL, Feeney A, Shipley M, Marmot M: Psychosocial work environment and sickness absence among British civil servants: the Whitehall II study. Am J Public Health. 1996, 86 (3): 332-40. 10.2105/AJPH.86.3.332.
Oxenstierna G, Ferrie J, Hyde M, Westerlund H, Theorell T: Dual source support and control at work in relation to poor health. Scand J Public Health. 2005, 33 (6): 455-63. 10.1080/14034940510006030.
Östergren PO, Hanson BS, Balogh I, Ektor-Andersen J, Isacsson A, Orbaek P, et al: Incidence of shoulder and neck pain in a working population: effect modification between mechanical and psychosocial exposures at work? Results from a one year follow up of the Malmo shoulder and neck study cohort. J Epidemiol Community Health. 2005, 59 (9): 721-8. 10.1136/jech.2005.034801.
Stansfeld SA, Fuhrer R, Shipley MJ, Marmot MG: Work characteristics predict psychiatric disorder: prospective results from the Whitehall II Study. Occup Environ Med. 1999, 56 (5): 302-7. 10.1136/oem.56.5.302.
Vingård E, Lindberg P, Josephson M, Voss M, Heijbel B, Alfredsson L, et al: Long-term sick-listing among women in the public sector and its associations with age, social situation, lifestyle, and work factors: a three-year follow-up study. Scand J Public Health. 2005, 33 (5): 370-5. 10.1080/14034940510005860.
Lidwall U, Marklund S: What is healthy work for women and men? – A case-control study of gender- and sector-specific effects of psycho-social working conditions on long-term sickness absence. Work. 2006, 27 (2): 153-63.
Ala-Mursula L, Vahtera J, Linna A, Pentti J, Kivimaki M: Employee worktime control moderates the effects of job strain and effort-reward imbalance on sickness absence: the 10-town study. J Epidemiol Community Health. 2005, 59 (10): 851-7. 10.1136/jech.2004.030924.
Niedhammer I, Chastang JF, David S, Barouhiel L, Barrandon G: Psychosocial work environment and mental health: Job-strain and effort-reward imbalance models in a context of major organizational changes. Int J Occup Environ Health. 2006, 12 (2): 111-9.
Busch H, Göransson S, Melin B: Self-efficacy beliefs predict sustained long-term sick absenteeism in individuals with chronic musculoskeletal pain. Pain Pract. 2007, 7 (3): 234-40. 10.1111/j.1533-2500.2007.00134.x.
Lidwall U, Marklund S, Skogman Thoursie P: Sickness absence in Sweden. Worklife and Health in Sweden 2004. Edited by: Gustafsson R, Lundberg I. 2004, Stockholm: National Institute for Working Life, 183-204.
Persson G, Danielsson M, Rosen M, Alexanderson K, Lundberg O, Lundgren B, et al: Health in Sweden: the National Public Health Report 2005. Scand J Public Health Suppl. 2006, 67: 3-10. 10.1080/14034950600677360.
Vahtera J, Kivimaki M, Pentti J, Linna A, Virtanen M, Virtanen P, et al: Organisational downsizing, sickness absence, and mortality: 10-town prospective cohort study. Bmj. 2004, 328 (7439): 555-10.1136/bmj.37972.496262.0D.
Östlin P: Gender inequalities in health: the significance of work. Gender and social inequities in health. Edited by: Wamala SP, Lynch J. 2002, Lund: Studentlitteratur, 43-65.
Holmgren K, Dahlin Ivanoff S: Women on sickness absence – views of possibilities and obstacles for returning to work. A focus group study. Disabil Rehabil. 2004, 26 (4): 213-22.
Holmgren K, Hensing G, Dahlin-Ivanoff S: Development of a questionnaire assessing work-related stress in women – identifying individuals who risk being put on sick leave. Disabil Rehabil. 2009, 31 (4): 284-292. 10.1080/09638280801931287.
Bengtsson C, Blohme G, Hallberg L, Hallström T, Isaksson B, Korsan-Bengtsen K, et al: The study of women in Gothenburg 1968–1969 – a population study. General design, purpose and sampling results. Acta Med Scand. 1973, 193 (4): 311-8.
Björkelund C, Andersson-Hange D, Andersson K, Bengtsson C, Blomstrand A, Bondyr-Carlsson D, et al: Secular trends in cardiovascular risk factors with a 36-year perspective: Observations from 38- and 50-years-olds in the population study of women in Gothenburg. Scan J Prim Health Care. 2008, Accepted for publication March 2008
Tibblin G, Tibblin B, Peciva S, Kullman S, Svärdsudd K: "The Goteborg quality of life instrument" – an assessment of well-being and symptoms among men born 1913 and 1923. Methods and validity. Scand J Prim Health Care Suppl. 1990, 1: 33-8.
Singh-Manoux A, Gueguen A, Martikainen P, Ferrie J, Marmot M, Shipley M: Self-rated health and mortality: short- and long-term associations in the Whitehall II study. Psychosom Med. 2007, 69 (2): 138-43. 10.1097/PSY.0b013e318030483a.
Voss M, Stark S, Alfredsson L, Vingard E, Josephson M: Comparisons of self-reported and register data on sickness absence among public employees in Sweden. Occup Environ Med. 2008, 65 (1): 61-7. 10.1136/oem.2006.031427.
Paoli P, Merllié D: Third European survey on working conditions 2000. Luxembourg: European Foundation for the Improvement of Living and Working Conditions. 2001
Phillips S, Sen D, McNamee R: Prevalence and causes of self-reported work-related stress in head teachers. Occup Med (Lond). 2007, 57 (5): 367-76. 10.1093/occmed/kqm055.
Collins PA, Gibbs AC: Stress in police officers: a study of the origins, prevalence and severity of stress-related symptoms within a county police force. Occup Med (Lond). 2003, 53 (4): 256-64. 10.1093/occmed/kqg061.
Rauhala A, Kivimaki M, Fagerstrom L, Elovainio M, Virtanen M, Vahtera J, et al: What degree of work overload is likely to cause increased sickness absenteeism among nurses? Evidence from the RAFAELA patient classification system. J Adv Nurs. 2007, 57 (3): 286-95. 10.1111/j.1365-2648.2006.04118.x.
Preckel D, von Kanel R, Kudielka BM, Fischer JE: Overcommitment to work is associated with vital exhaustion. Int Arch Occup Environ Health. 2005, 78 (2): 117-22. 10.1007/s00420-004-0572-8.
Krantz G, Östergren PO: Do common symptoms in women predict long spells of sickness absence? A prospective community-based study on Swedish women 40 to 50 years of age. Scand J Public Health. 2002, 30 (3): 176-83. 10.1080/14034940210133816.
Bultmann U, Huibers MJ, van Amelsvoort LP, Kant I, Kasl SV, Swaen GM: Psychological distress, fatigue and long-term sickness absence: prospective results from the Maastricht Cohort Study. J Occup Environ Med. 2005, 47 (9): 941-7. 10.1097/01.jom.0000172865.07397.9a.
Virtanen M, Vahtera J, Pentti J, Honkonen T, Elovainio M, Kivimaki M: Job strain and psychologic distress influence on sickness absence among Finnish employees. Am J Prev Med. 2007, 33 (3): 182-7. 10.1016/j.amepre.2007.05.003.
Siegrist J, Starke D, Chandola T, Godin I, Marmot M, Niedhammer I, et al: The measurement of effort-reward imbalance at work: European comparisons. Soc Sci Med. 2004, 58 (8): 1483-99. 10.1016/S0277-9536(03)00351-4.
Fahlen G, Knutsson A, Peter R, Åkerstedt T, Nordin M, Alfredsson L, et al: Effort-reward imbalance, sleep disturbances and fatigue. Int Arch Occup Environ Health. 2006, 79 (5): 371-8. 10.1007/s00420-005-0063-6.
Alexanderson K, Norlund A: Swedish Council on Technology Assessment in Health Care (SBU). Chapter 12. Future need for research. Scand J Public Health Suppl. 2004, 256-8. 10.1080/14034950410021925. 63
Holmgren K, Ivanoff SD: Supervisors' views on employer responsibility in the return to work process. A focus group study. J Occup Rehabil. 2007, 17 (1): 93-106. 10.1007/s10926-006-9041-4.
Statistics Sweden: Women and men in Sweden 2006. 2006, Stockholm: Official Statistics of Sweden
Gjerdingen D, McGovern P, Bekker M, Lundberg U, Willemsen T: Women's work roles and their impact on health, well-being, and career: comparisons between the United States, Sweden, and The Netherlands. Women and Health. 2000, 31 (4): 1-20.
Krantz G, Berntsson L, Lundberg U: Total workload, work stress and perceived symptoms in Swedish male and female white-collar employees. Eur J Public Health. 2005, 15 (2): 209-14. 10.1093/eurpub/cki079.
Jansen NW, Kant IJ, van Amelsvoort LG, Kristensen TS, Swaen GM, Nijhuis FJ: Work-family conflict as a risk factor for sickness absence. Occup Environ Med. 2006, 63 (7): 488-94. 10.1136/oem.2005.024943.
Göteborgs stad. (The city of Gothenburg). [homepage on the Internet]. Sjukförmåner (Sickness benefit). [updated 2007 Oct 9, cited 2008 Mars 20], [http://www.goteborg.se/statistik]
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/9/73/prepub
Acknowledgements
This study was supported by the Primary Health Care in Gothenburg and by grants from the local Research and Development Council of Gothenburg and Southern Bohuslän. 'The Population Study of Women in Gothenburg, Sweden' was supported by the Swedish Council for Working Life and Social Research (EpiLife and WISH studies) and Swedish Research Council. We thank Thorbjörn Jonsson for linguistic advice, and Valter Sundh for helping us with the statistical analyses.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
The work with this study was based on true collaboration between the authors. KH, SDI, GH contributed to the interpretation of data and in the development of the manuscript. KH, SDI, CB, GH have all contributed to the design of this study and revision of the manuscript. All authors read and approved of the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Holmgren, K., Dahlin-Ivanoff, S., Björkelund, C. et al. The prevalence of work-related stress, and its association with self-perceived health and sick-leave, in a population of employed Swedish women. BMC Public Health 9, 73 (2009). https://doi.org/10.1186/1471-2458-9-73
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-9-73