
Abstract
Background
Few validated guidelines exist for developing messages in health promotion practice. In clinical practice, the Appraisal of Guidelines, Research, and Evaluation II (AGREE II) Instrument is the international gold standard for guideline assessment, development, and reporting. In a case study format, this paper describes the application of the AGREE II principles to guide the development of health promotion guidelines for constructing messages to supplement the new Canadian Physical Activity Guidelines (CPAG) released in 2011.
Methods
The AGREE II items were modified to suit the objectives of developing messages that (1) clarify key components of the new CPAG and (2) motivate Canadians to meet the CPAG. The adapted AGREE II Instrument was used as a systematic guide for the recommendation development process. Over a two-day meeting, five workgroups (one for each CPAG – child, youth, adult, older adult – and one overarching group) of five to six experts (including behavior change, messaging, and exercise physiology researchers, key stakeholders, and end users) reviewed and discussed evidence for creating and targeting messages to supplement the new CPAG. Recommendations were summarized and reviewed by workgroup experts. The recommendations were pilot tested among end users and then finalized by the workgroup.
Results
The AGREE II was a useful tool in guiding the development of evidence-based specific recommendations for constructing and disseminating messages that supplement and increase awareness of the new CPAG (child, youth, adults, and older adults). The process also led to the development of sample messages and provision of a rationale alongside the recommendations.
Conclusions
To our knowledge, these are the first set of evidence-informed recommendations for constructing and disseminating messages supplementing physical activity guidelines. This project also represents the first application of international standards for guideline development (i.e., AGREE II) to the creation of practical recommendations specifically aimed to inform health promotion and public health practice. The messaging recommendations have the potential to increase the public health impact of evidence-based guidelines.
Similar content being viewed by others


Background
Public health practice is often criticized for a lack of evidence-based decision-making in program development and implementation in the area of health behavior change [1]. Indeed, over the past decade, a substantial body of research examining strategies for changing individuals’ health behavior (c.f., [2, 3]) has accumulated largely in the absence of systematic processes for disseminating the research findings to public health practitioners. In other health-related fields, evidence-based practice guidelines are a central mechanism for knowledge translation and a foundation for evidence-based decision-making. Evidence-based practice guidelines consolidate research evidence, can be disseminated broadly, and inform decision-making [4, 5]. In turn, guideline implementation can improve patient outcomes [6, 7]. To address the lack of evidence-based health behavior change practice recommendations, a systematic process for recommendation development is needed. Having an established process has potential to facilitate the translation of health behavior change research into practice and to address a significant research-to-practice gap. The development of recommendations will add practical value to the accumulating body of behavior change research and will create standards of practice with potential to improve the impact of health promotion programs.
In clinical medicine (e.g., oncology, cardiology), the Appraisal of Guidelines, Research, and Evaluation II (AGREE II) Instrument is the international gold standard for guideline assessment, development, and reporting [8]. Encompassing 23 items representing six quality domains (i.e., scope and purpose, stakeholder involvement, rigour of development, clarity of presentation, applicability, editorial independence), the AGREE II Instrument is generic and has potential to be applied to establishing guidelines for any step in the health care continuum (i.e., from health promotion to public health to interventions) [8]. Despite this potential, to our knowledge, the AGREE II has not been applied to guide the use of evidence to inform the development of health behavior change practice recommendations that can be used by public health practitioners. Using a case study format, in this paper we describe a process guided by a modified version of AGREE II for developing evidence-based recommendations for constructing behavior change messages to accompany the Canadian Physical Activity Guidelines (CPAG) for children, youth, adults, and older adults.
The context
Several countries (e.g., United States, Canada, United Kingdom) and international organizations (e.g., World Health Organization) have recently released new or updated physical activity guidelines [9–13]. These clinical practice guidelines were created through rigorous systematic review and development processes. (c.f., [10]). The CPAG in particular were developed in accordance with the AGREE II [8]. As a whole, these guidelines reflect the most up-to-date evidence for the frequency, intensity, duration and type of physical activity necessary to achieve health benefits. The guidelines do not, however, provide specific information aimed to persuade people to become more active. Thus, to motivate people to become active, the guidelines must be supplemented with messages that convey how to achieve the recommended activity level and why this is relevant to them (i.e., motivational messages). The responsibility for delivering these motivational messages largely falls to stakeholder organizations and practitioners disseminating the guidelines through their physical activity promotion initiatives (e.g., ad campaigns, brochures, websites). Thus to optimize uptake of the guidelines, organizations and practitioners need to be informed about the new guidelines, and given strategies for constructing motivational messages. To address this need among Canadian organizations, we undertook a two-phase process for developing recommendations for constructing messages to supplement the new CPAG specifically. In Phase 1, a systematic process was used to review the relevant literature. In Phase 2, an expert panel convened to develop the practical recommendations for the constructing messages to supplement the CPAG. The purpose of this case study is to provide an overview of these processes and a model for developing practice recommendations in other health behaviour change domains.
Phase 1: literature review and background rationale
A systematic process to inform the development of messages supplementing the CPAG was undertaken by the Canadian Society for Exercise Physiology (CSEP). Initially, the CSEP received funding from the Public Health Agency of Canada (PHAC) and the First Nations and Inuit Health Branch of Health Canada to support an evidence-informed review of the physical activity and messaging literature [14]. With additional funding from PHAC, the CSEP commissioned two systematic reviews of specific messaging and behaviour change techniques [15, 16]. The major conclusions from these three reviews were as follows:
● Brawley and Latimer [14] recommended that: a) messages should be informative, thought-provoking, clear, and persuasive while targeting constructs from behavior change theories (i.e., self-efficacy) and b) moderators that influence message impact should be identified and considered when creating messages and messaging interventions.
● Latimer, Brawley, and Bassett [15] concluded that although additional research is needed, tailored, gain-framed, and self-efficacy messages seemed to be promising strategies for constructing physical activity messages.
● Rhodes and Pfaeffi [16] identified notable gaps in the physical activity intervention literature and suggested that when developing messages supplementing the guidelines, there may be benefit in emphasizing aspects of self-regulation, self-efficacy and affective outcome expectancies.
Taken together, these three reviews provided the foundational principles for developing the message construction recommendations (Phase 2).
Phase 2: recommendation development
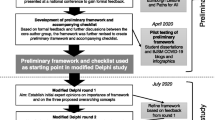
In Phase 2 of the message development process, an expert panel was convened. The panel was responsible for interpreting the evidence from Phase 1 and developing practical recommendations for constructing and disseminating messages supplementing the new CPAG. We followed a systematic protocol modified from the AGREE II Instrument [8] to ensure rigor, comprehensiveness and transparency in the process of developing the recommendations. The timeline for the project is outlined in Figure 1. The development process was conducted within the mandate of the CSEP program activities. Reporting upon the process including stakeholder evaluations represents secondary use of anonymous information. In accordance with the Tri-Council Policy statement these activities do not fall in the scope of research ethics review.

Timeline for developing and revising the messaging recommendations. This flow chart outlines the timeline for developing the messaging recommendations.
Methods
The two lead authors of this paper consulted one of the developers of the AGREE II Instrument to gain an understanding of: a) the methodological underpinnings of each of the 23 AGREE II items and b) how AGREE II principles applied to the objective of developing evidence-based messaging recommendations. With this knowledge, we modified the tool by tailoring the item wording to suit our objective. The modified items are described in Additional file 1. Specifically, we shifted the focus in the original AGREE II from patient populations to the guidelines’ target audiences (children, youth, adults and older adults). We also used a modified evidence review process to accommodate project constraints. When considering the implications of the recommendations, the impact on health outcomes was not considered directly but rather the impact of the recommendations on resource demands for organizations and stakeholders applying the recommendations was considered. The subsequent sections outline the application of the modified AGREE II domains.
AGREE domain 1: the scope and purpose
The objectives and the practical questions addressed by the recommendations were determined initially by the project leaders in consultation with three key stakeholders – CSEP, ParticipACTION, and PHAC. These three organizations were involved in defining the scope and purpose because they are considered leaders in physical activity promotion within Canada and were slated to jointly disseminate the CPAG. The objectives and practical questions addressed by our recommendations are listed in Additional file 1.
The expert workgroups determined the target populations for each of the messages and recommendations specific to each CPAG. The target populations were determined by reviewing evidence of key social influences on physical activity behavior (c.f. the list of resources included in Additional file 2). The target populations and rationale for these populations are outlined in Tables 1, 2, 3, 4, 5, 6 and the Additional files 3, 4, 5, 6, 7.
AGREE domain 2: stakeholder involvement
The CSEP, ParticipACTION, and the PHAC in consultation with the lead researchers determined the key stakeholders (end users) of the recommendations. The recommendations specifically were directed towards organizations (government and non-governmental) and individual health professionals using the CPAG to promote physical activity participation.
Key stakeholders were involved at multiple points throughout the process. For example, the project was directed by CSEP, ParticipACTION, and PHAC – with input from researchers with expertise in theoretical approaches to physical activity promotion and messaging. Twenty-eight experts from across Canada participated in small workgroups during a 2-day meeting. Experts included researchers from multiple disciplines, health professionals, and representatives from government and non-governmental organizations. The table included in Additional file 8 lists workgroup members, their expertise, and their roles in the guideline development process. Once developed, the recommendations were reviewed through an online consultation by 81 end users.
AGREE domain 3: rigor of development
The evidence-base
The evidence-base included systematic reviews related to physical activity determinants, message development, and message delivery [14–16], articles specific to messaging in Canada, and examples of successful comprehensive messaging campaigns [17–22]. The evidence-base was developed through purposeful article selection by the project directors rather than systematic review methods. This approach was used because multiple, up-to-date systematic reviews applicable to message development already were available and some context-specific data had recently been collected. Of benefit, this approach allowed expeditious preparation of the evidence-base and the inclusion of evidence specific to the Canadian context; yet this approach was susceptible to selection bias. The evidence selection methods were as follows:
-
a)
The systematic reviews prepared in Phase 1 of the project served as the focal evidence for the recommendations. In a further attempt to ensure broad inclusion of relevant literature and to minimize bias, the evidence-base also included additional review articles that were identified by the project directors while preparing their systematic reviews in Phase 1.
-
b)
A sample of articles reporting the success of past efforts to communicate the guidelines in Canada and of physical activity mass media campaigns in North America were selected from personal libraries. To reduce potential selection bias, the expert workgroup members were asked to identify any additional published messaging research specific to the North American context. No additional articles were circulated.
-
c)
The evidence base also included a summary of findings from a series of public consultations and a nation-wide survey regarding stakeholders’ preferences for the delivery of messages supplementing the new CPAG. The consultations and survey were completed by the PHAC just prior to the meeting. A representative from the PHAC delivered a presentation at the start of the meeting summarizing key findings related to Canadians’ preferred messengers and format for delivering the new CPAG and supplemental messages.
The strengths and limitations of the messaging evidence were considered extensively in each of the articles that the workgroups were provided. Common strengths of the evidence were: a) the application of a theoretical framework to guide physical activity behavior change (e.g.,[16, 17]); b) the availability of Canadian data describing previous efforts to disseminate physical activity guidelines (e.g.,[18, 19] ); and c) the use of large population-based samples to monitor message uptake (e.g., [20, 21] ). Common limitations included: a) the reliance on self-report measures to assess primary outcome variables (e.g., [15, 22]); b) the lack of evidence supporting theoretical mediators of behavior change resulting from interventions with low fidelity and no initial pilot testing (e.g.,[15–17]); and c) the restricted generalizability of the study findings to the larger population (many of the intervention studies used to inform our recommendations included samples of middle-aged women) [15]. As such, the quality of the messaging evidence was not assessed systematically. Rather, we relied on the expert panel to consider the strengths and limitations of the evidence as identified within each article and to judge the appropriateness of the evidence for informing the messaging recommendations.
In cases where the evidence provided did not adequately support a messaging recommendation, workgroup members were asked to seek out supplemental evidence from the peer-reviewed scientific literature. The quality of this supplemental evidence was not assessed directly; instead, expert panel members determined its appropriateness for use. For example, the work group focusing on the CPAG for children used several supplemental references to support the important role of parents in promoting physical activity in this age group.
Recommendation development
We developed the messaging recommendations through a multi-step process. One week in advance of the meeting, delegates were provided with a set of four to six articles from the evidence base to review. The resources provided to each workgroup are listed in a table included in Additional file 2. At the start of the meeting the project directors also delivered a 30-minute presentation summarizing key points to consider from the evidence base and the PHAC representative informed the group of the findings from their recent consultation process. Next, the workgroups participated in a series of structured discussions to formulate the guidelines. The workgroups were required to support each of their discussion points using the evidence base provided or supplemental evidence they had sought out independently. The larger group reviewed the key discussion points that emerged from each workgroup. Following the meeting, a summary document was circulated to the workgroups for review and revision. All recommendations and their associated evidence included in the final document are described in Additional files 3, 4, 5, 6, 7.
Implications and updates
The recommendations have direct practical implications. The practical benefit is that they are the first set of evidence-based recommendations for creating messages supplementing physical activity guidelines. The application of these recommendations to practice has the potential to increase the effectiveness of the uptake of physical activity guidelines through the creation of message-based resources and tools.
The larger group also discussed procedures for updating the messaging recommendations. Due to resource limitations within the end users’ organizations, regular updates to the messages in the absence of a subsequent revision to the CPAG were not viewed as feasible. The consensus was that there already were limited resources for the release of the new CPAG let alone for constantly updating materials promoting the guidelines. The CPAG are slated for review and update every three to five years [10]. This would be optimal timing for updating the messaging recommendations as well; likely new clarification messages would be necessary at minimum.
AGREE domain 4: clarity of presentation
For each CPAG, multiple recommendations were provided to allow flexibility in formulating messages. To create a concise resource for practitioners, the first author extracted these recommendations from the final summary document and created a series of information sheets. The information sheets include the recommendations and a preamble stating the objective of the recommendations. These information sheets were evaluated through a web-based survey by 81 practitioners including representatives from all levels of government (36.9%), fitness professionals (20.0%), staff/board members from non-governmental organizations (18.5%), and allied health professionals (10.8%). Each recommendation was rated on a 7-point scale for clarity, comprehensiveness, and ease of use. Participants also indicated their agreement with the recommendation and their likelihood of using the recommendation in practice. Overall, the responses to the survey were positive with all means falling above the scale midpoint and ranging from 4.48 to 5.43.
There were several suggestions to identify additional message target groups and channels of dissemination. Many participants requested additional details, examples, and resources. The specific recommendations were not modified in accordance with these requests. There was not adequate evidence to extend beyond the target groups and channels of dissemination already identified in the recommendations. Providing additional examples and resources was beyond the parameters of the recommendations. To address this feedback, the scope of the recommendations was clarified in the general preamble added to the beginning of the recommendations.
AGREE domain 5: applicability
Uptake
The applicability of the recommendations was thoroughly considered by the panel. Sample messages and possible channels for message dissemination were provided with the recommendations to facilitate their application to practice. The panel discussed potential barriers to implementing the messaging recommendations. Concerns were raised regarding how to transition between existing materials and new materials promoting the new CPAG. For example, some provincial organizations were in the middle of mass media campaigns that included messages and materials promoting the older guidelines. Uncertainty regarding the financial resources available to produce new materials to supplement the new CPAG and the lack of a comprehensive strategic plan for developing these materials were considered barriers to applying our messaging recommendations.
A subgroup of six experts was convened to discuss strategies for evaluating the dissemination of the new CPAG and supplemental materials. The use of existing data collection mechanisms (e.g., Canadian Fitness and Lifestyle Research Institute Physical Activity Monitor, ParticipACTION’s ongoing market survey) was recommended. The group also suggested using the hierarchy of effects model [23] and the RE-AIM framework [24] to guide the dissemination evaluation. Because no resources were allocated to either dissemination or evaluation, no specific plans were made to further develop an evaluation scheme.
AGREE domain 6: editorial independence
The process was funded by CSEP and PHAC. Although these organizations participated in the process of developing the recommendations, their involvement did not influence the recommendations for creating messages. Their involvement did influence discussions related to facilitators and barriers to implementation, resource implications and evaluation. Delegates from these organizations were able to present the real challenges facing the release of the new CPAG and the production of supplemental materials. The depth of the discussion related to evaluation was blunted by uncertainties related to available funding.
None of the workgroup members declared a conflict of interest.
Results
Recommendations
Through a systematic process guided by the AGREE II, we developed evidence-based specific recommendations for constructing and disseminating messages supplementing the new CPAG for children, youth, adults, and older adults. Recommendations also were developed to raise awareness of the new guidelines in general guided process. The recommendations are summarized in Tables 1, 2, 3, 4, 5, 6. The rationale supporting these recommendations is included in the Additional files 3, 4, 5, 6, 7.
Uptake
At the time of the consensus meeting, several opportunities for uptake of the messaging recommendations were anticipated through the three key stakeholder groups involved in the project. Initially, we intended our recommendations to inform the development of messages accompanying the CPAG when they were released in January 2011 (two months after the consensus meeting). This uptake did not come to fruition due to changes in our stakeholder involvement and delay in producing the final messaging recommendations.
While some supplementary materials were produced for the release of the CPAG, they were limited. Some of the materials did incorporate content that aligned with our recommendations.
Discussion
Strengths and limitations of our recommendations
To our knowledge, our efforts for constructing and disseminating messages supplementing the new CPAG represent the first set of evidence-informed recommendations for creating messages supplementing physical activity guidelines. Given that we drew from existing evidence of effective messaging interventions (e.g., VERB, ParticipACTION [22, 25]), these recommendations represent an accumulation of best practices in the field of physical activity promotion, health communications, and public health intervention.
Although the messaging recommendations have potential for shaping practice, their limitations must be acknowledged. Our recommendations do not have direct health benefits– they target an intermediary group (message developers) rather than the end users per se. However, if practitioners effectively apply the recommendations, there are potential indirect effects on health because the resulting messages will promote physical activity in accordance with the new CPAG.
The recommendations are further limited as a result of methodological constraints – many of which could easily have been addressed by involving a guideline development methodologist as part of the research team from the onset. First, the evidence-base was determined by the primary authors with suggestions from expert panel members. It also included findings from an unpublished government report that included newly collected data critical to informing the guidelines. Rigorous systematic review methods that include evaluation of study quality and strict inclusion criteria are optimal.
Second, the messaging recommendations were not sent for external review outside of the panel of experts who participated in the development process. The panel had substantial breadth in expertise; nonetheless external reviewers might have suggested modifications to strengthen the recommendations. Had we opted for additional external review, we could have sought the opinions of international experts, health communication technology researchers, and marketing and advertising professionals as individuals with this type of expertise were underrepresented in our workgroups. Indeed, the addition of individuals with expertise in the application of technology for health communications would have brought forward emerging evidence of promising technology-based approaches for disseminating our messages. With regards to marketing experts, only one panel member had specific expertise in this area. Public health often neglects to consult with this highly knowledgeable group of professionals. This shortcoming is unfortunate as marketing experts have potential to enhance reach of messages within the target audience and assist in designing visual, graphic and print copy of the final messages.
Third, we did not formally engage a methodologist throughout our process to participate in evaluation of the evidence, and to assess our process [26]. However, herein we report our process as transparently as possible. The objective of AGREE II is to promote transparency in the guideline development process. To ensure transparency in this case study, all of the steps undertaken in developing the messaging recommendation in relation to the AGREE II are outlined in the table included in Additional file 1.
The process of developing recommendations: successes, challenges and future directions
To our knowledge, this case study represents the first application of international standards for guideline development set out in the AGREE II Instrument to the development of practical recommendations specifically aimed to inform health promotion practice. Of benefit, the AGREE II Instrument provided a foundation for guiding the steps in the recommendation development process, for determining the make-up of our expert panel, and for reporting the process. The Instrument was quite easily adapted to suit our objective. Modifications primarily centered around shifting the guideline focus from patient groups to guideline message developers, using a modified evidence-review process, and considering the practical implications of the recommendations versus the direct health implications. With further development and validation, the adapted AGREE II Instrument has potential to become the standard for developing evidence-based health behavior change recommendations and, more generally, knowledge tools that facilitate the application of existing clinical practice guidelines.
We encountered practical challenges developing our messaging recommendations. Final messaging recommendations occurred over 1 year following our consensus meeting. The messaging consensus meeting was held in November 2010; the recommendations were not finalized until July 2011 and evaluated by stakeholders in January 2012 – more than one year following the consensus meeting. The lag could have been addressed by setting and adhering to clear time deadlines for the AGREE II steps following the consensus meeting.
Two factors impaired progress: a) the timeline for finalizing the recommendations and b) the absence of funds to develop messages supporting the guidelines. The timeline for developing recommendations was ambitious. The consensus panel meeting was held in November 2010, recommendations were needed by the key stakeholder groups almost immediately to begin production of messages to accompany the guidelines for a January 2011 launch. This timeline would have been feasible with adequate personnel to support the initiative; however, in the absence of resources, no personnel were available. As a temporary measure, the three key stakeholders were provided with a summary report from the expert panel to use in preparation for the guideline launch.
Finally, at the time of the consensus meeting it seemed promising that some resources would be allocated to developing materials supplementing the guidelines that would apply our recommendations. However, shortly after the meeting, the partnership between the three key stakeholders (CSEP, PHAC, ParticipACTION) dissolved. Plans for developing a comprehensive set of supplemental materials were halted and the immediate need for message construction recommendations was lessened.
As a result of these practical challenges, the application of the recommendations has been limited [27]. Much should be learned from this lack of uptake. While there was substantial interest and even excitement about producing recommendations to facilitate the application of CPAG, the lack of a feasible and sustainable plan for implementation hindered the application of the messaging recommendations. The dissolution of the partnership between the key stakeholders also dampened enthusiasm; the potential for implementation was substantially greater when all key stakeholders were committed to disseminating the CPAG and the accompanying motivational messages developed in accordance with our messaging recommendations in partnership. Our messaging recommendations represent advancement in knowledge translation efforts by researchers and stakeholders but highlight the fact that knowledge translation is a multi-step process that requires an enduring commitment of resources, financial and personnel, from all parties involved.
Conclusions
There is growing demand for evidence-informed decision-making in the design and implementation of health behavior change programming. Practitioners are challenged to meet these demands in the absence of evidence and specifically of recommendations that consolidate available evidence into a usable knowledge tool. This case study documents a two-phased process for translating this research into practical recommendations. To our knowledge, these are the first set of evidence-informed recommendations for constructing and disseminating health behavior change messages supplementing clinical practice guidelines. This project also represents the first application of international standards, the AGREE II, for the development of recommendations specifically aimed to inform behavior change practice. Application of these standards to other health behavior change initiatives has potential to facilitate the process of translating research into practice, and consequently strengthening health promotion programming.
References
Green LW, Ottoson JM, Garcia C, Hiatt RA: Diffusion theory and knowledge dissemination, utilization, and integration in public health. Annu Rev Public Health. 2009, 30: 151-174. 10.1146/annurev.publhealth.031308.100049.
Michie S, Abraham C, Whittington C, McAteer J, Gupta S: Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. 2009, 28 (6): 690-701.
Williams SL, French DP: What are the most effective intervention techniques for changing physical activity self-efficacy and physical activity behaviour–and are they the same?. Health Educ Res. 2011, 26 (2): 308-322. 10.1093/her/cyr005.
Bahtsevani C, Uden G, Willman A: Outcomes of evidence-based clinical practice guidelines: a systematic review. Int J Technol Assess Health Care. 2004, 20 (4): 427-433.
MacDermid JC, Graham I: Knowledge translation: putting the "practice" in evidence-based practice. Hand Clin. 2009, 25: 125-143. 10.1016/j.hcl.2008.10.003.
Cohen MG, Fonarow GC, Peterson ED, Moscucci M, Dai D, Hernandez AF, Bonow RO, Smith SC: Racial and ethnic differences in the treatment of acute myocardial infarction: findings from the Get With The Guidelines–Coronary Artery Disease program. Circulation. 2010, 121: 2294-2301. 10.1161/CIRCULATIONAHA.109.922286.
Hassett MJ, Hughes ME, Niland JC, Ottesen R, Edge SB, Bookman MA, Carlson RW, Theriault RL, Weeks JC: Selecting high priority quality measures for breast cancer quality improvement. Med Care. 2008, 46 (8): 762-770. 10.1097/MLR.0b013e318178ead3.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE: AGREE II: Advancing guideline development, reporting, and evaluation in health care. CMAJ. 2010, 182 (18): 10.1503/cmaj.090449.
Bull F: the Expert Working Groups: Physical activity guidelines in the U.K.: Review and recommendations. 2010, Loughborough: Loughborough University
Tremblay MS, Kho ME, Tricco AC, Duggan M: Process description and evaluation of Canadian Physical Activity Guidelines development. Int J Behav Nutr Phys Act. 2010, 7: 42-10.1186/1479-5868-7-42.
Tremblay MS, Leblanc AG, Carson V, Choquette L, Connor Gorber S, Dillman C, Duggan M, Gordon MJ, Hicks A, Janssen I: Canadian Physical Activity Guidelines for the Early Years (aged 0–4 years). Appl Physiol Nutr Metab. 2012, 37 (2): 345-369. 10.1139/h2012-018.
Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, Macera CA, Heath GW, Thompson PD, Bauman A: Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007, 116 (9): 1081-1093.
The Department of Human Health Services: 2008 Physical activity guidelines for Amercians. Physical activity guidelines for Amercians. 2008
Brawley LR, Latimer AE: Physical activity guidelines for Canadians: strategies for dissemination of the message, expectations for change and evaluation. Appl Physiol Nutr Metab. 2007, 32 (Suppl 2F): S189-205.
Latimer AE, Brawley LR, Bassett RL: A systematic review of three approaches for constructing physical activity messages: What messages work and what improvements are needed?. Int J Behav Nutr Phys Act. 2010, 7 (1): 36-10.1186/1479-5868-7-36.
Rhodes RE, Pfaeffli LA: Mediators of physical activity behaviour change among adult non-clinical populations: a review update. Int J Behav Nutr Phys Act. 2010, 7: 37-10.1186/1479-5868-7-37.
Lubans DR, Foster C, Biddle SJ: A review of mediators of behavior in interventions to promote physical activity among children and adolescents. Prev Med. 2008, 47 (5): 463-470. 10.1016/j.ypmed.2008.07.011.
Berry TR, Witcher C, Holt NL, Plotnikoff RC: A qualitative examination of perceptions of physical activity guidelines and preferences for format. Health Promot Pract. 2010, 11 (6): 908-916. 10.1177/1524839908325066.
Spence JC, Brawley LR, Craig CL, Plotnikoff RC, Tremblay MS, Bauman A, Faulkner GE, Chad K, Clark MI: ParticipACTION: awareness of the participACTION campaign among Canadian adults–examining the knowledge gap hypothesis and a hierarchy-of-effects model. Int J Behav Nutr Phys Act. 2009, 6: 85-10.1186/1479-5868-6-85.
Cameron C, Craig CL, Bull FC, Bauman A: Canada's physical activity guides: has their release had an impact?. Can J Public Health. 2007, 98 (Suppl 2): S161-169.
Wong F, Huhman M, Heitzler C, Asbury L, Bretthauer-Mueller R, McCarthy S, Londe P: VERB™—a social marketing campaign to increase physical activity among youth. Prev Chronic Dis. 2004, 1: A10-
Craig CL, Bauman A, Gauvin L, Robertson J, Murumets K: ParticipACTION: A mass media campaign targeting parents of inactive children; knowledge, saliency, and trialing behaviours. Int J Behav Nutr Phys Act. 2009, 6: 88-10.1186/1479-5868-6-88.
McGuire WJ: Public communication as a strategy for inducing health-promoting behavioral change. Prev Med. 1984, 13 (3): 299-319. 10.1016/0091-7435(84)90086-0.
Glasgow RE, Vogt TM, Boles SM: Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999, 89 (9): 1322-1327. 10.2105/AJPH.89.9.1322.
Huhman ME, Potter LD, Duke JC, Judkins DR, Heitzler CD, Wong FL: Evaluation of a national physical activity intervention for children: VERB campaign, 2002–2004. Am J Prev Med. 2007, 32 (1): 38-43. 10.1016/j.amepre.2006.08.030.
Tremblay MS, Haskell WL: From science to physical activity guidelines. 2012, Champaign: Human Kinetics Publishers
Gainforth HL, Spence JC, Berry T, Craig CL, Faulkner G, Rhodes R, Tremblay MS, Latimer-Cheung AE: Evaluating the uptake of Canada’s New Physical Activity Guidelines. Trans Behav Med. 10.1007/s13142-012-0190-z.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/13/419/prepub
Acknowledgements
The recommendation development process was funded by the Canadian Society for Exercise Physiology (CSEP), with partial support from the Public Health Agency of Canada (PHAC) (contract no. 4500245966). Preparation of the manuscript was supported by the Canadian Institutes of Health Research (CIHR) Canada Research Chair Program (AEL), a Canadian Cancer Society Senior Scientist Award, a CIHR graduate fellowship (HLG) and a Social Sciences and Humanities Research Council (SSHRC) graduate fellowship (MJP). MEK is funded by a CIHR Fellowship award and Bisby Prize. We thank The CPAG Messaging Recommendation Workgroup for participating in the expert panel and review of the recommendations and manuscript. Workgroup members include: Mark Beauchamp (University of British Columbia), Marianne Bernardo (ParticipACTION), Tanya Berry (University of Alberta), Guy Faulkner (University of Toronto), Audrey Hicks (McMaster University), Ian Janssen (Queen’s University), Allana Leblanc (Children’s Hospital of Eastern Ontario Research Institute), Monica LeBarge (Queen’s University), Kathleen Martin Ginis (McMaster University), Don Paterson (Western University), John Spence (Western University), Mark Tremblay (Children’s Hospital of Eastern Ontario Research Institute), Lori Zehr (Camosun College).
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AELC, RER, MEK, and MD participated in the conception, design, and coordination of the study. ALC, RER, MEK and JRT helped to draft the manuscript. HLG assisted with manuscript revision. JRT, HLG, KK, GN, and MJP participated in the acquisition of data and study coordination. The CPAG Messaging Recommendation Workgroup developed and reviewed the recommendations. All authors read and approved the final manuscript.
Electronic supplementary material
12889_2012_5362_MOESM1_ESM.docx
Additional file 1: Table S1: Modifications to AGREE II items. The table lists the AGREE II items and includes descriptions of how the items were modified and applied in the case study. (DOCX 20 KB)
12889_2012_5362_MOESM2_ESM.docx
Additional file 2: Table S2: Resources provided to workgroups. This table lists the references for the materials provided to each workgroup. (DOCX 18 KB)
12889_2012_5362_MOESM3_ESM.docx
Additional file 3: Supporting Evidence for the Messaging Recommendations for the New Canadian Physical Activity Guidelines for Overarching Messages. This file provides the rationale and lists the supporting evidence for each of the overarching messaging recommendations. (DOCX 25 KB)
12889_2012_5362_MOESM4_ESM.docx
Additional file 4: Supporting Evidence for the Messaging Recommendations for the New Canadian Physical Activity Guidelines for Children. This file provides the rationale and lists the supporting evidence for the messaging recommendations for the CPAG for Children. (DOCX 27 KB)
12889_2012_5362_MOESM5_ESM.docx
Additional file 5: Supporting Evidence for the Messaging Recommendations for the New Canadian Physical Activity Guidelines for Youth. This file provides the rationale and lists the supporting evidence for the messaging recommendations for the CPAG for Children. (DOCX 28 KB)
12889_2012_5362_MOESM6_ESM.docx
Additional file 6: Supporting Evidence for the Messaging Recommendations for the New Canadian Physical Activity Guidelines for Adults. This file provides the rationale and lists the supporting evidence for the messaging recommendations for the CPAG for Children. (DOCX 25 KB)
12889_2012_5362_MOESM7_ESM.docx
Additional file 7: Supporting Evidence for the Messaging Recommendations for the New Canadian Physical Activity Guidelines for Older Adults. This file provides the rationale and lists the supporting evidence for the messaging recommendations for the CPAG for Older Adults. (DOCX 28 KB)
12889_2012_5362_MOESM8_ESM.docx
Additional file 8: Table S3: Expert panel. This table lists the names, expertise, and roles of the individuals who participated in the recommendation development meeting. (DOCX 19 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Latimer-Cheung, A.E., Rhodes, R.E., Kho, M.E. et al. Evidence-informed recommendations for constructing and disseminating messages supplementing the new Canadian Physical Activity Guidelines. BMC Public Health 13, 419 (2013). https://doi.org/10.1186/1471-2458-13-419
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-13-419