
Abstract
Background
After total mesorectal excision (TME) for rectal cancer around 10% of patients develops local recurrences within the pelvis. One reason for recurrence might be spillage of cancer cells during surgery. This pilot study was conducted to investigate the incidence of remnant cancer cells in pelvic lavage after resection of rectal cancer. DNA from cells obtained by lavage, were analysed by denaturing capillary electrophoresis with respect to mutations in hotspots of the k-ras gene, which are frequently mutated in colorectal cancer.
Results
Of the 237 rectal cancer patients analyzed, 19 had positive lavage fluid. There was a significant survival difference (p = 0.006) between patients with k-ras positive and negative lavage fluid.
Conclusion
Patients with k-ras mutated cells in the lavage immediately after surgery have a reduced life expectation. Detection of exfoliated cells in the abdominal cavity may be a useful diagnostic tool to improve the staging and eventually characterize patients who may benefit from aggressive multimodal treatment of rectal cancer.
Similar content being viewed by others


Background
Cancer of the rectum is frequent in both genders and the incidence in Norway is still increasing, with a total of 1137 new cases in a population of 4.6 million citizens in 2004 [1]. Survival in cancer of rectum has continuously improved in the past ten year period [1, 2]. The main reasons for this is the introduction of total mesorectal excision (TME) [3] and better staging with adjuvant treatment for patient in high risk groups [4]. In spite of such improvement, local recurrence after potentially curative surgery is a major problem. There are several possible causes for local recurrences including: incomplete resection of the primary carcinoma [4, 5], insufficient removal of involved regional lymph nodes [6], development of a secondary tumour near the suture site and exfoliated cancer cells released at the time of surgery [7]. Dissemination of tumour cells in the presacral space, as well as in tumour lymphatic drainage and in peripheral blood vessels after resection of the tumour, might play a role in the metastasis process, thus affecting the clinical course. Previous reports have indicated that tumours can release DNA into the circulation [8–10]. Hence, recovery of mutated cell by pelvic lavage after resection of rectal cancer was hypothesized to be of prognostic value. One of the most prominent mutated genes in colorectal cancer is Kirsten ras 2 (k-ras), a member of the RAS family. Mutations in the k-ras gene is described as an early event in the process of colorectal carcinogenesis [11]. K-ras mutations are mainly found in exon 1, codon 12, 13 and exon 2, codon 61. Mutations in codon 12 account for 80–90% of k-ras gene alterations with several hotspots [12]. Oncogenic mutations of k-ras are involved in 20–50% of colorectal cancers [13, 14]. The k-ras mutation frequency in rectal cancer has been reported to be 15–33% which is lower than in colon cancer [15, 16]. We used k-ras exon 1 as the only tumour cell-associated marker to determine the presence of disseminated tumour cells in peritoneal lavage samples from patients undergoing surgery for rectal cancer. The aim of this pilot study was to evaluate the method denaturant capillary electrophoresis (DCE), to detect tumour cells in peritoneal lavage fluid of patients undergoing resection for rectal cancer.
Methods
Study population
The University Hospital Rikshospitalet-Radiumhospitalet is a tertiary referral center for locally advanced primary and recurrent rectal cancer. The treatment regime is multimodal and includes preoperative radiotherapy or chemoradiation.
Our patients undergo surgery a median 56 days after end of long course radiation therapy.
Peritoneal lavage from 237 patients and tumour samples from 186 patients (59% men, 41% women) with either locally advanced or local recurrent rectal cancer was collected during surgery at the Norwegian Radium Hospital between 2000 and 2006. Patient's age ranged from 29 to 87 years with a median age of 66. All samples were collected after written informed consent. Possible risk factors for dissemination of cancer cells intraoperatively were registered: resection through the periphery of the cancer as in R1 and R2 resections, tumour perforation or the presence of lymph node metastases in the mesorectum. Penetration of cancer through the serosa and the presence of macroscopic peritoneal carsinomatosis may of course give rise to free cancer cells and were thoroughly registrated. Two cases with registrated peritoneal carsinomatosis were tested as "positive controls". Tumours were pathologically staged according to the TNM classification [17] except for the local recurrences that do not fit into this except for pTo. This is due to the observation that a recurrence usually starts outside the rectal wall and most often there are no lymph nodes to resect [18]. The local surgical achievements were staged as follows: R0 microscopically free circumferential and distal margins, R1 microscopically involved margins, and R2 locally macroscopic residual cancer or no resection. N0; No regional lymph node metastasis. N1; Metastasis in 1 to 3 regional lymph nodes. N2; Metastasis in 4 or more regional lymph nodes. NX; unknown status of lymph nodes.
Sample treatment
After resection of the tumour the pelvis was washed with sterile water 200–600 ml (discarded) subsequently followed by 200–600 ml saline water. Thereafter two specimens of 50 ml were aspirated to 50 ml centrifuge tubes. The second sample of 50 ml most often contained more white blood cells than the first sample because haemostasis was not complete. Cells were harvested by centrifugation at 1200 g for 10 minutes followed by removal of the supernatant. The cell pellets were frozen at -20°C until DNA extractions were performed. QIAamp DNA Kit (Qiagen, Valencia, California, USA) was used for the DNA extraction, following the manufacturers instructions.
Polymerase chain reaction
The target sequences were amplified through a nested PCR protocol to circumvent amplification of a pseudogene. Primers were designed with use of Primer 3 [18, 19]. The first PCR reaction consisted of approximately 50 ng genomic DNA, 0.05 U/μl Taq, polymerase, 0.005 U/μl PFU polymerase, 1× Buffer (ABgene), 2.5 mM MgCl2, and 0.4 mM dNTP mix (ABgene) and 0.15 μM of each primer (5'CTTAAGCGTCGATGGAGGAG3', 5'AGAATGGTCCTGCACCAGTAA3'). The second PCR used a 1:1000 dilution of the first PCR products as template while the polymerase, buffer, MgCl2 and dNTP concentrations stayed the same. Primers, one labelled primer with GC-clamp (5'- 6Fam-CGCCCGCCGCGCCCCGCGCCCGTCCCGCCGCCCCCGCCCGCCTCTATTGTTGGATCATATTC3') at a final concentration of 0.11 μM and one reveres primer (5'CATTATTTTTATTATAAGG3') in a final concentration 0.3 μM were added to the mix. The total volumes of both PCR reactions were adjusted to 10 μl with sterile water. Temperature cycling was performed in a Mastercycler® (Eppendorf, Bergman AS, Lillestrøm, Norway) using the following cycling conditions: denaturation 5 min at 96°C, followed by 35 cycles of 95°C in 30 s, annealing 56°C in 30s (first PCR) and 48°C in 30s (second PCR) and 72°C in 60s.
We also analysed k-ras exon 2, and braf exon 11 and exon 15, but were unable to find any mutations with these markers in the lavage samples.
Mutation detection
Amplified 6-fam labelled PCR products were analysed by denaturant capillary electrophoresis in a MegaBACE 1000 DNA Analysis System (GE Healthcare Bio-Sciences AB, Uppsala, Sweden). The base substitutions were separated by cycling temperature capillary electrophoresis (CTCE), with mean separating temperatures of 48.5°C and amplitudes of 3°C cycled 20 times. K-ras mutations in exon 1 were identified by co-analysis with a mutated internal standard in a similar manner as previously described by Bjørheim et al. [20]. Additionally, samples with a high mutant fraction were sequenced according to standard DNA sequencing protocol (GE Healthcare Bio-Sciences AB).
Follow-up
The patients were followed for five years with X-ray of the chest and CT of the pelvis and abdomen every three to six months for five years or to the end of the study period. Data concerning death was crosschecked with the national health register.
Statistics
Patient's data were prospectively registered in a database. All data was analyzed using the Statistical Package SPSS 12.5 for Windows. The chi-squared tests were used for statistical analysis and differences were considered significant at P < 0.05. For survival analysis, Kaplain-Meiers curves were constructed, and using the log-rank test assessed differences in survival between groups.
Results
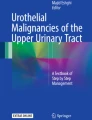
The clinical pathological characteristics of the 237 rectal cancer patients are summarized in Table 1. Of the eleven possible risk factors tested with regard to patients with positive and negative k-ras markers in the lavage fluid, only N- and R-stage were significantly different between the two groups (p = 0.03 and p = 0.002, respectively). This was mainly due to a higher percentage of N0 and R0 stages in the k-ras negative group. We analyzed 186 of the removed tumours for k-ras mutations and 56 of these were k-ras positive. 19 out of 237 patients had a positive k-ras marker in the lavage fluid (Table 2). Of the 19 cases with k-ras positive lavage there were 12 R0, 3 R1 and 4 R2. We have estimated survival rate for the patients with positive and negative marker for lavage fluid by a Kaplan-Meier plot (Figure 1) and a log rank test. Mean observation time was 25 (1–66) months for all patients. Patients positive for the marker in the lavage fluid had a mean survival of 22 months with a Std. Error 3.7 (C.I 14.6–29.1) months compared to 47 months with a Std. Error 2.4 (C.I 43.2–50.8) for patients with a negative marker (p = 0.006). As R1 and R2 resections are more likely to have positive lavage fluid a new log rank test was done with only R0 patients. The result showed that there was still a significant difference between the two groups (p = 0.02).

A. K-ras in lavage samples immediately after surgery related to survival. B. K-ras in tumours samples from rectal cancers patients related to survival.
There was no significant difference (p = 0.3) between k-ras positive and negative tumours with respect to survival (Figure 1b). Likewise when mutational status of k-ras for the tumour was compared for R0, the non-significant role was maintained (p = 0.09).
In two of the cases of R0 resections with k-ras positive lavage the preoperative biopsy was classified as k-ras negative being either a result of non-representative biopsy or a multi-clonal locally advanced tumour.
Discussion
This study accessed the incidence of free colorectal cancer cells or remnants of such cells in the pelvic cavity immediately after surgery, and correlates their presence with several clinicopathological parameters and survival. A significant number of local recurrences following rectal cancer surgery cannot be explained by incomplete resection, lymphatic or vascular invasion [21]. This suggests that viable tumour cells with proliferate and perhaps metastatic potential have been shed from the primary tumour site either before removal of the tumour or during the surgical procedure. In our study we found that 19 rectal cancer patients had disseminated tumour cells in the 237 lavage fluids from the rectal patients. And we found that these patients with invisible tumour material in abdomen immediately after surgery tend to have a worse prognosis than patients without free tumour cells that could not be explained by differences in other risk factors. Only N- and R-stage were statistically significantly different between the k-ras positive and negative groups. In both cases this should be to the advantage of the k-ras negative group containing relatively more N0 and R0 stages.
Gross (R2) or microscopic (R1) positive surgical margins are well known indicators of recurrence and survival. However, our results showed that 12 of the 19 positive k-ras cases were R0 resections, which was an unpredicted result. Resection into the circumference of macroscopic (R2 resection) or microscopic tumour (R1 resection) or into the depth of the tumour can of course contribute to disseminated cells in the peritoneal cavity as well as is in cases with tumour penetration of serosa or in overt peritoneal carcinomatosis. As there were relatively more R0 stage resections in the k-ras negative group this is unlikely to explain our finding. Lymph node metastases might contribute by the shedding of cancer cells from a surgically severed lymphatic vessel. Several groups have observed a relationship between the number of lymph nodes identified at pathological examination and survival in colorectal cancer patients [22, 23]. The higher percentage of N0 stage in the k-ras negative group could not explain the difference either. In our study there was no significant difference in estimated survival, but a possible trend observed between patients with k-ras positive and k-ras negative tumor markers in the solid tumor samples. This may rest upon the fact that the plots are more or less similar until 30 months postoperatively and diverge after this observation time. Thus within the observed period a k-ras mutation in the tumor itself does not explain the prognostic differences of the patients. In this study we have found that patients with tumour cells in abdomen after operation tend to have a worse prognosis than patients without free tumour cells. Our results in this study are similar to those of some studies with regard to survival [24–27], but in conflict with other results [28, 29]. These differences could be related to patient selection and the methods used for detection as well as the follow-up methods.
It has become apparent in recent years that not only do the pathologic characteristics of rectal cancer influence the long-term outcome in terms of local recurrence and survival, but also that the surgeon is an important variable. This previously has been demonstrated by the reports from the Norwegian Rectal Cancer Group [30, 31]. Better treatment, specialist care, recruitment into clinical trials or treatment protocols and any combination of these factors almost certainly influence regional variations in cancer outcome. The Norwegian Radium Hospital is a comprehensive cancer centre with high-volume surgery and the rectal cancers patient population is mostly TNM stage II and III. In this pilot study only rectal cancer patients have been included.
The detection of disseminated tumour cells depends on a number of steps including collection and treatment of samples, cell separation protocols and chosen markers. Technical advancements in detecting free DNA have been made over the years. All methods used depend on the recognition of antigens or gene markers assumed to be exclusively expressed by tumour cells and not by normal tissue in the examined sample. A cytology based method can only detect nanogram quantities of DNA. Immunohistochemistry leads to an increased sensitivity, but without improved specificity. High number of false positives due to non specific labelling was still observed and low sensitivity and specificity contribute to the conflicting results previously reported in detection of disseminated tumour cells [25, 28, 29]. With the introduction of PCR, smaller quantities of DNA could be detected. The robustness of such analysis has been improved by fluorescence-based allelotyping techniques involving capillary electrophoresis. These molecular detection methods can be divided in two groups: Detection of RNA with marker-gene expression (m-RNA) and detection of RNA specific to the tissue. This is a sensitive method with a possible detection of one single mutated cell in up to 108 wild-type cells in an optimal condition. However RNA is unstable in the extracellular environment and its detection in tissue or fluids is thus dependent on the presence of viable tumour cells. Routinely performed clinical sampling methods such as lavage may not be capable to preserve the RNA capacity of the cells. The other method is detection of tumour specific chromosomal abnormalities or mutations. In solid tumours these variations are heterogenous and complex with a need for detecting mutations in a small fraction. We have previously demonstrated that the DCE method used in this study fulfils these criteria with a sensitivity of 4 × 10-3 [32].
The viability of exfoliated cells and the ability of these cells to become implanted and proliferated in the peritoneum have been confirmed by several studies [33, 34]. We have not tested the viability of the tumour cells, because we assume that they are all compromised after the lavage treatment of sterilized water. A high diagnostic certainty is essential for establishing microscopic peritoneal dissemination as a prognostic factor. A standard procedure of peritoneal washing with sterile water subsequently followed by saline water was done after operation. Given the procedure and the sensitivity of the k-ras assay (limit is reported to be 1% for the homoduplexes and 0.1% for the heteroduplexes for a varity of target sequences), minor or moderate bleeding in the surgical area could result in a mutant fraction below the detection limit. One microliter of blood contains an average of 5000 white blood cells, hence if 10 millilitre of blood leaked into the lavage area, 50 000 k-ras positive tumour cells would be required for detection. Albeit this stringent limitation, k-ras mutant positive cells were regularly detected in lavage fluids from the pelvic cavity. There are no known tumour-specific markers for rectal cancer. K-ras is shown to be up-regulated in epithelial tumour cells [35] and was used as a marker for free tumour cells or cell remnants in the peritoneal cavity. The k-ras gene has a small hotspot region, which makes it possible to detect 80–90% of k-ras gene alterations with a simple PCR. However variation (20–50%) of the prevalence of k-ras mutations in small sporadic colorectal adenomas have been reported in the literature [35]. Specific k-ras mutations induce different biological consequences by affecting differently the structural confirmation and the function of the mutated protein [36, 37]. For example, a number of studies have demonstrated an impact of k-ras mutations for cancer progression and predispose to more aggressive biological behaviour in patients with colorectal cancer [36, 38–40]. K-ras mutations have also shown to be predictor of resistance to the anti-epidermal growth factor receptor (cetuximab) therapy and are associated with a an impaired prognosis [41].
In this study we found the frequency of k-ras mutations in tumour to be 30% and one-third of these showed k-ras mutations in the lavage fluid. Thus in 70% of these patients a k-ras mutant is absent. Therefore other gene mutations need to be investigated to obtain increased sensitivity. To date as mention earlier there is no general genetic marker that gives accurate information on the prognostic impact for patients with rectal cancer. New analyses of mutations or combinations of genes that are specific for rectal carcinoma might lead to better candidates. Detection of cancer specific markers in an abdomen without visible tumour deposits and with a proven increased risk of recurrence obviously imposes the question of additional therapy either as intraoperative hyperthermic chemotherapy or systemic chemotherapy or any combination of these. It should be remembered that this is a pilot study that needs to be confirmed in an appropriate multicenter study before therapeutic considerations are carried out.
Conclusion
The overall clinical value of this molecular approach needs further elucidation. The k-ras gene seems to be a good genetic marker for detecting circulating tumour cells from rectal cancer patients. However, studies with gene markers covering a larger number of tumours are important. Examination of lavage fluids before and after surgery will further elucidate the mechanism of inducing exfoliated tumour cells. If our results are confirmed, in the future detection of disseminated cancer cells might enable the selection of high-risk patients with poorer prognosis, who would benefit from adjuvant treatment.
References
The Cancer Registry of Norway. http://www kreftregisteret no/. 2006, [http://www.kreftregisteret.no/]
Wibe A, Carlsen E, Dahl O, Tveit KM, Weedon-Fekjaer H, Hestvik UE, Wiig JN: Nationwide quality assurance of rectal cancer treatment. Colorectal Dis. 2006, 8: 224-229. 10.1111/j.1463-1318.2005.00924.x.
Heald RJ, Husband EM, Ryall RD: The mesorectum in rectal cancer surgery--the clue to pelvic recurrence?. Br J Surg. 1982, 69: 613-616. 10.1002/bjs.1800691019.
Larsen SG, Wiig JN, Dueland S, Giercksky KE: Prognostic factors after preoperative irradiation and surgery for locally advanced rectal cancer. Journal of Surgical Oncology (EJSO). 2008, 34: 410-417. 10.1016/j.ejso.2007.05.012.
Wiig JN, Carlsen E, Søreide O: Mesorectal excision for rectal cancer: a view from Europe. Semin Surg Oncol. 1998, 15: 78-86. 10.1002/(SICI)1098-2388(199809)15:2<78::AID-SSU4>3.0.CO;2-2.
Herrera-Ornelas L, Justiniano J, Castillo N, Petrelli NJ, Stulc JP, Mittelman A: Metastases in small lymph nodes from colon cancer. Arch Surg. 1987, 122: 1253-1256.
Basha G, Penninckx F: Exfoliated tumour cells and locally recurrent colorectal cancer. Acta Chir Belg. 1996, 96: 66-70.
Tong YK, Lo YM: Diagnostic developments involving cell-free (circulating) nucleic acids. Clin Chim Acta. 2006, 363: 187-196. 10.1016/j.cccn.2005.05.048.
Kanellos I, Zacharakis E, Kanellos D, Pramateftakis MG, Betsis D: Prognostic significance of CEA levels and positive cytology in peritoneal washings in patients with colorectal cancer. Colorectal Dis. 2006, 8: 436-440. 10.1111/j.1463-1318.2006.00991.x.
Ziegler A, Zangemeister-Wittke U, Stahel RA: Circulating DNA: a new diagnostic gold mine?. Cancer Treat Rev. 2002, 28: 255-271. 10.1016/S0305-7372(02)00077-4.
Fearon ER, Vogelstein B: A genetic model for colorectal tumorigenesis. Cell. 1990, 61: 759-767. 10.1016/0092-8674(90)90186-I.
Breivik J, Lothe RA, Meling GI, Rognum TO, Børresen-Dale AL, Gaudernack G: Different genetic pathways to proximal and distal colorectal cancer influenced by sex-related factors. Int J Cancer. 1997, 74: 664-669. 10.1002/(SICI)1097-0215(19971219)74:6<664::AID-IJC18>3.0.CO;2-5.
Russo A, Bazan V, Agnese V, Rodolico V, Gebbia N: Prognostic and predictive factors in colorectal cancer: Kirsten Ras in CRC (RASCAL) and TP53CRC collaborative studies. Ann Oncol. 2005, 16 Suppl 4:iv44-iv49.: iv44-iv49. 10.1093/annonc/mdi907.
Boughdady IS, Kinsella AR, Haboubi NY, Schofield PF: K-ras gene mutations in adenomas and carcinomas of the colon. Surg Oncol. 1992, 1: 275-282. 10.1016/0960-7404(92)90088-3.
Servomaa K, Kiuru A, Kosma VM, Hirvikoski P, Rytomaa T: p53 and K-ras gene mutations in carcinoma of the rectum among Finnish women. Mol Pathol. 2000, 53: 24-30. 10.1136/mp.53.1.24.
Frattini M, Balestra D, Suardi S, Oggionni M, Alberici P, Radice P, Costa A, Daidone MG, Leo E, Pilotti S, Bertario L, Pierotti MA: Different genetic features associated with colon and rectal carcinogenesis. Clin Cancer Res. 2004, 10: 4015-4021. 10.1158/1078-0432.CCR-04-0031.
American Joint Committee on Cancer. http://www cancerstaging org/. 2006, [http://www.cancerstaging.org/]
Wiig JN, Larsen SG, Dueland S, Giercksky KE: Preoperative irradiation and surgery for local recurrence of rectal and rectosigmoid cancer. Prognostic factors with regard to survival and further local recurrence. Colorectal Dis. 2008, 10: 48-57. 10.1111/j.1463-1318.2008.01576.x.
Rozen S, Skaletsky H: Primer3 on the WWW for general users and for biologist programmers. Methods Mol Biol. 2000, 132: 365-386.
Bjørheim J, Gaudernack G, Giercksky KE, Ekstrøm PO: Direct identification of all oncogenic mutants in K-ras exon 1 by cycling temperature capillary electrophoresis. Electrophoresis. 2003, 24: 63-69. 10.1002/elps.200390032.
Wu JS, Fazio VW: Management of rectal cancer. J Gastrointest Surg. 2004, 8: 139-149. 10.1016/j.gassur.2003.10.011.
George S, Primrose J, Talbot R, Smith J, Mullee M, Bailey D, du BC, Jordan H: Will Rogers revisited: prospective observational study of survival of 3592 patients with colorectal cancer according to number of nodes examined by pathologists. Br J Cancer. 2006, 95 (7): 841-847. 10.1038/sj.bjc.6603352.
Johnson PM, Porter GA, Ricciardi R, Baxter NN: Increasing negative lymph node count is independently associated with improved long-term survival in stage IIIB and IIIC colon cancer. J Clin Oncol. 2006, 24: 3570-3575. 10.1200/JCO.2006.06.8866.
Lloyd JM, McIver CM, Stephenson SA, Hewett PJ, Rieger N, Hardingham JE: Identification of early-stage colorectal cancer patients at risk of relapse post-resection by immunobead reverse transcription-PCR analysis of peritoneal lavage fluid for malignant cells. Clin Cancer Res. 2006, 12: 417-423. 10.1158/1078-0432.CCR-05-1473.
Hase K, Ueno H, Kuranaga N, Utsunomiya K, Kanabe S, Mochizuki H: Intraperitoneal exfoliated cancer cells in patients with colorectal cancer. Dis Colon Rectum. 1998, 41: 1134-1140. 10.1007/BF02239435.
Lennon AM, Mulcahy HE, Hyland JM, Lowry C, White A, Fennelly D, Murphy JJ, O'Donoghue DP, Sheahan K: Peritoneal involvement in stage II colon cancer. Am J Clin Pathol. 2003, 119: 108-113. 10.1309/J6BDTWM2M792TN2V.
Wang JY, Hsieh JS, Chang MY, Huang TJ, Chen FM, Cheng TL, Alexandersen K, Huang YS, Tzou WS, Lin SR: Molecular detection of APC, K- ras, and p53 mutations in the serum of colorectal cancer patients as circulating biomarkers. World J Surg. 2004, 28: 721-726.
Vogel P, Ruschoff J, Kummel S, Zirngibl H, Hofstadter F, Hohenberger W, Jauch KW: Prognostic value of microscopic peritoneal dissemination: comparison between colon and gastric cancer. Dis Colon Rectum. 2000, 43: 92-100. 10.1007/BF02237250.
Kanellos I, Demetriades H, Zintzaras E, Mandrali A, Mantzoros I, Betsis D: Incidence and prognostic value of positive peritoneal cytology in colorectal cancer. Dis Colon Rectum. 2003, 46: 535-539. 10.1007/s10350-004-6595-0.
Wibe A, Moller B, Norstein J, Carlsen E, Wiig JN, Heald RJ, Langmark F, Myrvold HE, Soreide O: A national strategic change in treatment policy for rectal cancer--implementation of total mesorectal excision as routine treatment in Norway. A national audit. Dis Colon Rectum. 2002, 45: 857-866. 10.1007/s10350-004-6317-7.
Wibe A, Eriksen MT, Syse A, Tretli S, Myrvold HE, Soreide O: Effect of hospital caseload on long-term outcome after standardization of rectal cancer surgery at a national level. Br J Surg. 2005, 92: 217-224. 10.1002/bjs.4821.
Kristensen AT, Bjørheim J, Minarik M, Giercksky KE, Ekstrøm PO: Detection of mutations in exon 8 of TP53 by temperature gradient 96-capillary array electrophoresis. Biotechniques. 2002, 33: 650-653.
Umpleby HC, Fermor B, Symes MO, Williamson RC: Viability of exfoliated colorectal carcinoma cells. Br J Surg. 1984, 71: 659-663. 10.1002/bjs.1800710902.
Skipper D, Cooper AJ, Marston JE, Taylor I: Exfoliated cells and in vitro growth in colorectal cancer. Br J Surg. 1987, 74: 1049-1052. 10.1002/bjs.1800741130.
Barry EL, Baron JA, Grau MV, Wallace K, Haile RW: K-ras mutations in incident sporadic colorectal adenomas. Cancer. 2006, 106: 1036-1040. 10.1002/cncr.21721.
Smakman N, Borel R, Voest EE, Kranenburg O: Control of colorectal metastasis formation by K-Ras. Biochim Biophys Acta. 2005, 1756: 103-114.
Al Mulla F, MacKenzie EM: Differences in in vitro invasive capacity induced by differences in Ki-Ras protein mutations. J Pathol. 2001, 195: 549-556. 10.1002/path.995.
Andreyev HJ, Norman AR, Cunningham D, Oates J, Dix BR, Iacopetta BJ, Young J, Walsh T, Ward R, Hawkins N, Beranek M, Jandik P, Benamouzig R, Jullian E, Laurent-Puig P, Olschwang S, Muller O, Hoffmann I, Rabes HM, Zietz C, Troungos C, Valavanis C, Yuen ST, Ho JW, Croke CT, O'Donoghue DP, Giaretti W, Rapallo A, Russo A, Bazan V, Tanaka M, Omura K, Azuma T, Ohkusa T, Fujimori T, Ono Y, Pauly M, Faber C, Glaesener R, de Goeij AF, Arends JW, Andersen SN, Lovig T, Breivik J, Gaudernack G, Clausen OP, De Angelis PD, Meling GI, Rognum TO, Smith R, Goh HS, Font A, Rosell R, Sun XF, Zhang H, Benhattar J, Losi L, Lee JQ, Wang ST, Clarke PA, Bell S, Quirke P, Bubb VJ, Piris J, Cruickshank NR, Morton D, Fox JC, Al Mulla F, Lees N, Hall CN, Snary D, Wilkinson K, Dillon D, Costa J, Pricolo VE, Finkelstein SD, Thebo JS, Senagore AJ, Halter SA, Wadler S, Malik S, Krtolica K, Urosevic N: Kirsten ras mutations in patients with colorectal cancer: the 'RASCAL II' study. Br J Cancer. 2001, 85: 692-696. 10.1054/bjoc.2001.1964.
Lee JC, Wang ST, Lai MD, Lin YJ, Yang HB: K-ras gene mutation is a useful predictor of the survival of early stage colorectal cancers. Anticancer Res. 1996, 16: 3839-3844.
Benhattar J, Losi L, Chaubert P, Givel JC, Costa J: Prognostic significance of K-ras mutations in colorectal carcinoma. Gastroenterology. 1993, 104: 1044-1048.
Lievre A, Bachet JB, Le Corre D, Boige V, Landi B, Emile JF, Cote JF, Tomasic G, Penna C, Ducreux M, Rougier P, Penault-Llorca F, Laurent-Puig P: KRAS mutation status is predictive of response to cetuximab therapy in colorectal cancer. Cancer Res. 2006, 66: 3992-3995. 10.1158/0008-5472.CAN-06-0191.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2407/8/213/prepub
Acknowledgements
This work received financial support by the Torsteds Legacy and the Norwegian Cancer Society.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare they have no competing interests.
Authors' contributions
ATK participated in the design of the study, performed the experiments, data analyzes and drafted the manuscript. JNW and STG were responsible for all the samples from rectal cancer patient and clinical data, and revised the manuscript. KEG and POE conceived and participated in the design of study, revised the manuscript and supervised the whole process of the study. All the authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Kristensen, A.T., Wiig, J.N., Larsen, S.G. et al. Molecular detection (k-ras) of exfoliated tumour cells in the pelvis is a prognostic factor after resection of rectal cancer?. BMC Cancer 8, 213 (2008). https://doi.org/10.1186/1471-2407-8-213
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2407-8-213