
Abstract
Background
Medulloblastoma is the most common malignant brain tumor of childhood. Improvements in clinical outcome require a better understanding of the genetic alterations to identify clinically significant biological factors and to stratify patients accordingly. In the present study, we applied cytogenetic characterization to guide the identification of biologically significant genes from gene expression microarray profiles of medulloblastoma.
Methods
We analyzed 71 primary medulloblastomas for chromosomal copy number aberrations (CNAs) using comparative genomic hybridization (CGH). Among 64 tumors that we previously analyzed by gene expression microarrays, 27 were included in our CGH series. We analyzed clinical outcome with respect to CNAs and microarray results. We filtered microarray data using specific CNAs to detect differentially expressed candidate genes associated with survival.
Results
The most frequent lesions detected in our series involved chromosome 17; loss of 16q, 10q, or 8p; and gain of 7q or 2p. Recurrent amplifications at 2p23-p24, 2q14, 7q34, and 12p13 were also observed. Gain of 8q is associated with worse overall survival (p = 0.0141), which is not entirely attributable to MYC amplification or overexpression. By applying CGH results to gene expression analysis of medulloblastoma, we identified three 8q-mapped genes that are associated with overall survival in the larger group of 64 patients (p < 0.05): eukaryotic translation elongation factor 1D (EEF1D), ribosomal protein L30 (RPL30), and ribosomal protein S20 (RPS20).
Conclusion
The complementary use of CGH and expression profiles can facilitate the identification of clinically significant candidate genes involved in medulloblastoma growth. We demonstrate that gain of 8q and expression levels of three 8q-mapped candidate genes (EEF1D, RPL30, RPS20) are associated with adverse outcome in medulloblastoma.
Similar content being viewed by others

Background
Medulloblastoma is the most common malignant brain tumor of childhood. Treatment with surgery, radiation, and chemotherapy successfully cures many patients, but survivors can suffer significant long-term toxicities affecting their neurocognitive and growth potential. Despite clinical advances, up to 30% of children with medulloblastoma experience tumor progression or recurrence, for which no curative therapy exists [1]. The lack of more effective, less toxic therapies and the inability to stratify patients biologically result from imperfect understanding of the molecular processes that underlie medulloblastoma growth [1–3].
The advent of genomic technologies has permitted a more global approach to tumor classification, diagnosis, and prognostication [4–6]. Several medulloblastoma series have been analyzed for copy number aberrations (CNAs) with comparative genomic hybridization (CGH), widely considered a standard method for genome-wide screening [7–12]. Using CGH, we have determined that gain of the long arm of chromosome 8 is associated with overall and progression-free survival of medulloblastoma patients.
Despite its limited resolution, chromosomal CGH can guide gene expression analysis, suggesting potential oncogenes or tumor suppressor genes involved in tumor growth. Our identification of 8q gain as clinically significant prompted the search for candidate genes mapped to that chromosomal region. Previous reports have identified MYC amplification and overexpression as clinically significant. However, we did not note such associations in our series. We investigated the possibility of other 8q-mapped candidate genes by exploiting the microarray analysis of an overlapping set of medulloblastoma specimens to complement the scale of our CGH dataset.
Of the 71 tumors we analyzed by CGH, a subset of 27 were among 64 medulloblastomas previously analyzed using gene expression microarrays, which permitted integrated analysis of both sets of data [6]. We identified three 8q-mapped genes overexpressed in tumors with 8q gain and whose expression levels were significantly associated with overall survival in all 64 patients: eukaryotic translation elongation factor 1D (EEF1D), ribosomal protein L30 (RPL30), and ribosomal protein S20 (RPS20). We corroborated the expression of each candidate gene in microarray analysis by quantitative real time-RTPCR (qRT-RTPCR). By analyzing expression microarray data and cytogenetic profiles, we have identified a group of clinically significant genes involved in translational regulation that display relatively small expression changes and previously eluded implication by single platform approaches.
Methods
Patient samples
Seventy-one medulloblastoma samples were obtained following informed consents via Institutional Review Board (IRB)-approved protocols from patients (aged 7 months – 38 years) diagnosed between 1991 and 2004 at Children's Hospital (Boston, MA) and Texas Children's Hospital (Houston, TX). Of these, 27 tumors were also previously analyzed by expression profiling using oligonucleotide microarrays [6] [Figure 1]. All specimens were obtained at the time of diagnosis prior to radiation or chemotherapy and subjected to histopathologic review according to WHO criteria [3]. Tumor samples were snap-frozen and stored in liquid nitrogen.

Experimental design. Genomic characterization of 71 medulloblastomas was performed with CGH and the most frequent CNAs were subjected to survival analysis. Twenty-seven tumors also had gene expression profile data, and were used to identify differentially expressed genes based on tumor chromosomal profiles. For survival analysis, the 64 medulloblastoma patients were stratified according to the expression values for each candidate gene.
All patients were initially treated with maximally feasible surgical resection. Subtotal or partial resection was achieved in eleven patients. Chemotherapy for most patients (n = 50) consisted of repeated cycles of cisplatin and vincristine, with combinations of carboplatin, etoposide, cyclophosphamide and/or lomustine [13–16]. The other twenty-one patients received intensified chemotherapy cycles (vincristine, cisplatin, cyclophosphamide, and etoposide) with autologous stem cell support [17]. Patients greater than 36 months old received craniospinal irradiation 2,400 ± 360 centiGray (cGy) with a tumor dose of 5,300 ± 720 cGy. For the entire group, median follow up was 36 months (mean 39 months, range 4 – 109). All studies were performed with the approval of the Committee for Clinical Investigation and the IRB of Boston Children's Hospital, Harvard Medical School, and the IRB of Baylor College of Medicine for Texas Children's Hospital.
Comparative Genomic Hybridization (CGH) and survival analysis
Tumor DNA was extracted using the DNeasy Tissue Protocol (Qiagen, Valencia, CA). In cases of limited tissue, DNA was extracted using TRIZOL according to the manufacturer's instructions (Invitrogen, Carlsbad, CA), or from paraffin-embedded tissues using standard methods with proteinase K digestion, phenol: chloroform extraction, and ethanol precipitation [18]. Total cellular RNA from a matching portion of frozen tissue was extracted using TRIZOL or RNeasy (Qiagen). The established medulloblastoma cell line Daoy (American Type Culture Collection, Manassas, VA) was maintained to provide control RNA, as previously described [19].
Normal metaphase spreads and chromosomal CGH were performed on 71 tumor specimens as previously described [20]. Briefly, DNA from normal female human placental controls and medulloblastoma samples were labeled by nick-translation with Texas red-5-dUTP and fluorescein (FITC)-12-dUTP, respectively (Dupont NEN, Boston, MA), and co-hybridized onto normal metaphase chromosomes. Images from at least ten to fifteen separate metaphases were captured by CCD camera (SenSys Photometrics, Tucson, AZ) mounted on a Nikon Eclipse 800 microscope. The fluorescence signal ratio (FITC:Texas red) along each chromosome was calculated with Quantitative Image Processing System (Applied Imaging, Santa Clara, CA). The average of fluorescence ratios and their 99% confidence intervals were determined for each tumor specimen. Threshold ratio values greater than 1.2 and lower than 0.8 defined tumor gains and losses, respectively. High-level amplification was defined as fluorescence ratios in excess of 2.0 at the chromosomal site.
For survival analysis of each CNA, patients were stratified into two groups based on the presence or absence of the specific cytogenetic lesion. Only those lesions detected in a minimum of five patients (7%) were analyzed. Clinical outcome measures, including overall and progression-free survival, were determined from the date of diagnosis using the method of Kaplan and Meier (SPSS v.11; SPSS, Inc, Chicago, IL). The significance of survival differences between patient groups was calculated by log-rank test. To test if 8q gain was an independent prognostic factor, we also performed multivariate analysis using Cox proportional hazard model for 8q gain with respect to three other clinical prognostic factors: extent of resection, age relative to 3 years and metastatic stage at diagnosis.
Gene expression microarray analysis and candidate gene identification
Twenty-seven of the 71 tumors characterized by CGH were previously analyzed for their gene expression profiles on Affymetrix HuGeneFL microarrays and were among the series of 64 reported by Pomeroy et al. [6]. We normalized the CEL files of 64 tumors and four normal cerebellar controls. The probe set intensities used for comparisons were calculated by model-based expression index using dCHIP software (v1.3, http://www.dCHIP.org) [21]. Among the 44 tumors that were collected subsequently and not included in the previous report, seven were analyzed on the Affymetrix U133 Plus 2.0 microarrays and their resulting datasets were processed similarly for direct comparison with parallel qRT-RTPCR results.
Differentially expressed candidate genes mapped to 8q were subsequently analyzed for overall and progression-free survival in the larger group of 64 profiled tumors based on their expression levels (Kaplan-Meier test, SPSS). Patients were stratified into two groups based on their tumor expression level relative to that mean value. Candidate genes achieving p values less than 0.05 (log-rank test, SPSS) were validated using qRT-RTPCR. Fisher's exact test was used to calculate the significance of the association between gene expression levels with tumor and clinical variables.
Quantitative Real Time-RTPCR (qRT-RTPCR)
Tumor RNA was analyzed by qRT-RTPCR performed in a Bio-Rad iQ4 Multicolor Real Time iCycler (Bio-Rad Laboratories, Hercules, CA). Total cellular RNA was reverse transcribed with M-MLV Reverse Transcriptase enzyme (Invitrogen) and oligo-(dT)12, according to the manufacturer's recommendations. PCR reactions containing cDNA, iQ Syber Green Supermix (Bio-Rad), and primers for EEF1D, RPL30, RPS20, MYC, or MYCN were performed in triplicate for 40 cycles (95°C 15 sec, 60°C 1 min). Amplification products were verified by melting curves, agarose gel electrophoresis, and sequencing. Copy numbers were internally normalized to GAPDH expression, quantitated relative to the Daoy cell line as a calibrator tissue control, and accounting for differences in primer efficiencies [22]. Results from at least three separate experiments were analyzed. Fisher's exact test was used to calculate the significance of the association between gene expression levels with tumor and clinical variables. We determined correlation coefficients (R2) between expression levels detected by microarray and by qRT-RTPCR using the Pearson method (relative to the Daoy cell line as a tissue control). Primer sequences are: EEF1D, sense 5'-CCCGCGTCCGCCGATTCCTC-3' and antisense 5'-CGCTGGCGCCGTTCTCCTG-3'; RPL30 sense, 5'-TGGTGGCTGCAAAGAAGAC-3' and antisense 5'-GCAGTTGTTAGCGAGAATGAC-3'; RPS20 sense, 5'-CACGCTCCTGCTCCTGACTC-3' and antisense 5'-GCGGCTTGTTAGGCTGATTCG-3'; MYC sense, 5'-TCTGGATCACCTTCTGCTGG-3' and antisense 5'-TGTTGCTGATCTGTCTCAGG-3'; MYCN sense, 5'-AGAGGACACCCTGAGCGATT-3' and antisense 5'-TCTTGGGACGCACAGTGATG-3';GAPDH sense, 5'-AAGGTGAAGGTCGGAGTCAA-3' and antisense, 5'-AATGAAGGGGTCATTGATGG-3'.
Results
Patient analysis and clinical data
We analyzed overall and progression-free survival for patient groups stratified by clinical variables such as age, sex, metastatic (Chang) stage, histologic subtype, and treatment regimens. Not surprisingly, metastatic disease at diagnosis displayed a trend toward worse survival [Table 1]. For other reported risk factors, only age less than three years was weakly associated with adverse clinical outcome, which could be attributed to the lack of craniospinal radiation therapy in these patients. Neither sex nor tumor histology correlated with outcome. Furthermore, different treatment centers and regimens (standard dose chemotherapy plus radiation vs. intensified chemotherapy with autologous stem cell support) were not associated with differences in survival.
Overview of CNAs in medulloblastoma
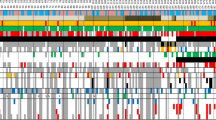
The 71 medulloblastomas analyzed by chromosomal CGH displayed a variety of CNAs [Figure 2; Table 2]. The most frequently observed CNAs involved chromosome 17 (i.e. loss of the short arm, 17q gain). The loss of 17p accompanied by concurrent gain of 17q, consistent with isochromosome 17q (i17q), was detected in 32% of tumors. Losses were more frequently observed than gains and predominated on chromosomes 16, 10, 8, and 11.

Summary of Comparative Genomic Hybridization. Ideogram showing genetic imbalances detected in 71 medulloblastoma by comparative genomic hybridization (CGH). Red bars on the left of the chromosomes represent losses and green bars on the right correspond to gains of chromosomal regions in tumors; amplifications are depicted as bold green bars. Multiple cases with the same CNA are grouped as thick bars, with total number of cases displayed at the top.
We also detected gain of 2p in 22% of tumors, including 5.6% with amplification at 2p23-p24, which was the most common amplification detected in our series (n = 4). Other recurrent amplifications were detected at 2q14, 7q34, and 12p13 in two specimens each and at 8q23-q24 in one tumor. Given the resolution of chromosomal CGH (approximately 10–20 Mb), the 2p23-p24 amplifications and the 8q23-q24 amplification probably include the MYCN (2p24.1) and MYC (8q24.12-q24.13) loci, respectively. Amplifications and low copy number gains at 2p23-p24 or 8q23-q24 were not associated with large cell or anaplastic histology.
CNA-based survival analysis reveals association with gain of 8q
To evaluate the clinical significance of common CNAs, we stratified 71 medulloblastoma patients according to the presence or absence of specific cytogenetic lesions in their tumors. Specific CNAs involving 58 chromosomal regions were observed in a minimum of 7% tumors and used to stratify patients for Kaplan-Meier survival analysis [Table 2]. The most common lesions, including loss of 17p and/or gain of 17q, were not significantly associated with outcome.
Another common CNA, gain of 2p (minimal region 2p23-p24) detected in 22.5% of tumors (n = 16) displayed a trend towards worse overall survival (p = 0.0848) [Table 3, Figure 3]. Amplification at 2p23-p24 seen in 5.6% of tumors (n = 4) was also associated with worse overall survival (p = 0.0152). However, gain of 2p without 2p23-p24 amplification in 17% of tumors (n = 12) was not associated with outcome.

Survival analysis of patients stratified by gain of the long arm of chromosome 2. Kaplan-Meier analysis of overall survival (OS) in 71 patients with medulloblastoma stratified by gain of 2p: sixteen patients with 2p gain compared to 55 others without 2p gain. Follow-up is expressed as time from diagnosis in months.
Gain of 8q (minimal region 8q23-q24, in 10% of tumors) displayed the strongest association with significantly worse overall and progression-free survival (p = 0.0141 and 0.0004, respectively) [Table 3, Figure 4]. The gain of 8q was also associated with adverse outcome in the well described high-risk group of patients were younger than three years of age at diagnosis (n = 14) (p = 0.0023). One of seven tumors with 8q gain also displayed large cell/anaplastic histology with partial loss of 8p23-q22 and amplification at 8q23-q24, which includes the MYC locus (8q24.12-q24.13). When the single case of 8q amplification is excluded from the analysis, the other six patients with gain of 8q22-q24 displayed an even stronger association with overall survival (p = 0.0005).

Survival analysis of patients stratified by gain of the long arm of chromosome 8. Kaplan-Meier analysis of overall survival (OS) in 71 patients with medulloblastoma stratified by gain of 8q: seven patients with 8q gain and 64 others without 8q gain. Follow-up is expressed as time from diagnosis in months.
We performed multivariate analysis to test the significance of 8q gain with regard to outcome. When controlled for widely accepted prognostic factors (i.e. extent of resection, age relative to 3 years and metastatic stage at diagnosis), 8q gain is still significantly associated with both PFS and OS (p = 0.003 and 0.013, respectively) [see Additional file 1].
Adverse outcome is not associated with MYC or MYCNexpression
To address the potential contribution of MYC or MYCN, we screened gene expression microarray data of 27 medulloblastoma specimens that were among 64 previously reported tumors [6]. We did not discern significant upregulation of MYCN or other 2p-mapped gene expression in the seven tumors with 2p gain or amplification relative to the twenty tumors without 2p gain [Table 4]. Nor did we detect an association between MYCN expression and overall survival in the larger group of 64 medulloblastomas. We corroborated the microarray data with qRT-RTPCR in 12 primary medulloblastomas and determined that MYCN was not significantly overexpressed in tumors with gain or amplifications of 2p, compared to others (p = 0.31) [Table 4].
We also examined the possible contribution of MYC expression to the clinical significance of 8q gain. Higher levels of MYC expression correlated with slightly worse outcome among the larger group of 64 medulloblastomas, although failed to achieve statistical significance (in agreement with previous results) [6]. In addition, MYC was not consistently overexpressed in microarray-analyzed tumors with 8q gain (n = 3) [Table 4]. We quantitated MYC in twelve available tumor specimens with qRT-RTPCR and found that MYC was not significantly upregulated in the two tumors with 8q gain (t = 0.49). Not surprisingly, the one tumor with 8q23-q24 amplification displayed the highest MYC level, while low copy number gains of 8q did not correlate with higher MYC levels in either microarray- or qRT-RTPCR-tested specimens. As tested by qRT-RTPCR, relative MYC expression correlated highly with microarray results (R2 = 0.99). Overall, these data suggest that MYC expression, like 8q amplification, is not entirely responsible for the association of 8q gain with survival.
Independent of 8q status, adverse outcome is associated with expression of 8q-mapped genes: EEF1D, RPL30, and RPS20
Since MYC amplification and expression were not associated with overall survival in our series, we analyzed gene expression data to identify other candidate genes affected by this specific CNA. Of the 27 medulloblastomas with both CGH and microarray data, 11% displayed 8q gain, whose expression profiles were compared to the other 89% of tumors. Of the 149 genes with at least 1.5-fold differential expression levels, 27 genes were upregulated in 8q gain tumors and five genes mapped to 8q. Since gene dosage effects related to chromosomal gains may contribute to higher relative gene expression, we sought to define those candidate genes significantly associated with clinical outcome.
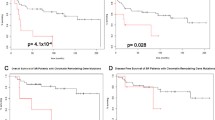
In the larger group of 64 microarray-profiled tumors, the expression levels of three of five 8q-mapped genes were adversely associated with overall and progression-free survival: eukaryotic translation elongation factor 1D (EEF1D;p values, 0.014 (OS) and 0.0085 (PFS), log-rank), ribosomal protein L30 (RPL30;p values, 0.014 (OS) and 0.0018 (PFS)), and ribosomal protein S20 (RPS20;p values, 0.0005 (OS) and 0.0213 (PFS)) [Table 4; Figures 5, 6, 7]. In fact, we detected elevated levels of these genes in many tumors without 8q gain. This suggests that not only do these candidate genes contribute to outcome in patients with 8q gain tumors, but also in those regardless of their cytogenetic profiles. The expression levels of EEF1D, RPL30, and RPS20 did not correlate with MYC expression in the 64 microarray-profiled tumors.

Survival analysis of patients stratified by expression of eukaryotic translation elongation factor 1 delta ( EEF1D ). Kaplan-Meier analysis of overall survival in 64 patients with medulloblastoma based on Hu6800FL array data for the 8q-mapped candidate gene, eukaryotic translation elongation factor 1 delta (EEF1D). We calculated the mean between the median expression level of tumors with 8q gain and the median level of those without it. Patients were stratified into two groups based on their tumor expression level relative to that mean. Follow-up is expressed as time from diagnosis in months.

Survival analysis of patients stratified by expression of ribosomal protein L30 ( RPL30 ). Kaplan-Meier analysis of overall survival in 64 patients with medulloblastoma based on Hu6800FL array data for the 8q-mapped candidate gene, ribosomal protein L30 (RPL30). We calculated the mean between the median expression level of tumors with 8q gain and the median level of those without it. Patients were stratified into two groups based on their tumor expression level relative to that mean. Follow-up is expressed as time from diagnosis in months.

Survival analysis of patients stratified by expression of ribosomal protein S20 ( RPS20 ) expression. Kaplan-Meier analysis of overall survival in 64 patients with medulloblastoma based on Hu6800FL array data for the 8q-mapped candidate gene, ribosomal protein S20 (RPS20). We calculated the mean between the median expression level of tumors with 8q gain and the median level of those without it. Patients were stratified into two groups based on their tumor expression level relative to that mean. Follow-up is expressed as time from diagnosis in months.
Because the 64 tumor specimens profiled on Affymetrix HuGeneFL, were unavailable for further analysis by qRT-RTPCR, we could not validate candidate gene expression directly. Alternatively, we assayed the expression of EEF1D, RPL30, and RPS20 with qRT-RTPCR in twelve available medulloblastoma specimens, including those analyzed by Affymetrix U133 Plus 2.0 microarrays [Table 4]. To corroborate the tumor profiles, we compared the expression of each candidate gene by qRT-RTPCR with the new set of microarray-generated data on Affymetrix U133 Plus 2.0. As expected, each candidate gene demonstrated a broader range of differential expression by qRT-RTPCR than by microarray, consistent with signal compression [23]. Our qRT-RTPCR results correlated well with the expression patterns noted in microarray data (R2, 0.53–0.90) [Table 4], indicating that observed expression levels detected by microarray analysis likely reflect tumor differences.
Discussion
We report the results of our CGH analysis of a large series of medulloblastoma and the application of CNA-based outcome analysis of expression datasets to identify candidate genes. The relative frequencies of various CNAs are consistent with previous CGH reports [7, 9–12]. The most common aberrations involved chromosome 17, including loss of 17p and gain of 17q, which were not significantly associated with outcome in our series. Several reports have studied the clinical significance of CNAs, in particular involving chromosome 17, but with discordant results. Loss of 17p correlated with survival in several series [24–27]. Mendrzyk et al [28] and Pan et al [10] have described adverse outcomes associated with combined 17p loss and 17q gain, as in iso17q, respectively. Negative studies include those of Biegel et al [29], Emadian et al [30], Jung et al [31], and Nicholson et al [32]. In general, these studies evaluated fewer samples or follow-up was limited. In addition, multiple clinical factors probably contribute to discrepancies among different series.
Our CGH-based outcome analysis reveals a significant association between 8q gain (minimal common region 8q23-q24) and worse overall survival, confirmed by multivariate analysis by controlling for three known prognostic factors. We detected 8q gain in only seven cases of the 71 tumor specimens analyzed. The relatively low frequency of 8q gain probably prevented detection of its clinical significance in other series. MYC amplification has been identified as a marker of poor prognosis, but previous studies did not further characterize cytogenetic changes involving 8q. In fact, excluding the only patient with tumor amplification at 8q23-q24 from the outcome analysis actually strengthens the association of 8q gain with overall survival. Although only a minority of specimens was available for confirmatory qRT-RTPCR quantitation, in those tumors tested, MYC levels correlated well with microarray results. MYC expression levels, however, were not associated with survival in our series, in contrast with previous reports [33]. Overall, our results indicate that biological factors associated with 8q gain other than MYC achieve clinical significance in our series of medulloblastoma patients. Due to the relatively low frequency of 8q gain, however, its prognostic significance requires confirmation in studies with larger sample size.
Our CGH and gene expression analysis indicate that other genes mapped to 8q may contribute to clinical outcome. We screened microarray profiles in an overlapping subset of tumors to identify differentially expressed candidate genes overexpressed in specimens with 8q gain. The expression of three candidate genes were associated with overall and progression-free survival: EEF1D, RPL30, and RPS20. By analyzing the larger group of 64 patients, we confirmed the association of these candidate genes with outcome. In fact, among the 64 patients, higher expression of EEF1D, RPL30, and RPS20 correlated with worse overall and progression-free survival regardless of cytogenetic profile. Since we also detected overexpression of these candidate genes in tumor samples without 8q gain, alternate mechanisms of induction may otherwise contribute to tumor phenotype and clinical outcome.
These candidate genes represent a novel group involved in translational regulation and have not been previously associated with outcome in medulloblastoma. Although we previously reported that RPL30 expression was associated with classic histology, the smaller expression differences precluded prior detection and association with survival [6]. In that study, we employed a two-class comparison of array profiles based on an unsupervised clustering algorithm (self-organizing map) to define a multi-gene predictor of adverse outcome. The multi-gene predictor included several other ribosomal genes, but did not include EEF1D, RPL30, or RPS20. All three candidate genes are involved in ribosomal functions: RPS20 encodes a component of the 60S ribosomal subunit, and RPL30 part of the 40S subunit. The EEF1D protein contributes to delivery of t-RNA to ribosomes. The overexpression of EEF1D has been associated with advanced tumor stage in gastrointestinal carcinomas and EEF1D reportedly displays oncogenic properties in vitro [34–36]. This supports the hypothesis that increased expression of ribosomal genes confers a growth advantage [37].
Indeed, accumulating evidence indicates that aberrant regulation of ribosomes, their components, and their functions can be linked to cellular transformation. Several oncogenes and tumor suppressor genes, including MYC and MYCN, regulate the expression of rRNA and ribosomal proteins [37]. Not surprisingly, cancer cells display increased metabolism and protein synthesis, which requires upregulated ribosomal proteins and rRNA [37]. Since ribosomal proteins and translation factors directly regulate protein synthesis, influencing ribosomal biogenesis is one of the possible mechanisms by which cellular growth controls can be disrupted, resulting in increased proliferation. It remains unclear precisely how deregulation of rRNA and ribosomal functions are involved in tumor formation or progression. Nonetheless, our results suggest that better appreciation of the relative contributions of EEF1D, RPL30, RPS20, and their associated regulatory mechanisms will impact our understanding of medulloblastoma biology. The identification of these three candidate genes indicates that specific mechanisms of ribosomal biosynthesis and translational regulation are certainly worthy of future study in medulloblastoma.
Conclusion
In summary, our CGH survey of 71 medulloblastomas indicates that the gain of 8q is adversely associated with overall and progression-free survival in patients with medulloblastoma. We applied our cytogenetic results to guide the expression analysis of a subset of twenty-seven tumors and subsequent outcome analysis in the larger group of 64 tumors. By exploiting these complementary genomic datasets, we have implicated the expression of three 8q-mapped candidate genes (EEF1D, RPL30, and RPS20) as adversely associated with overall and progression-free survival, independent of cytogenetic profile. Our results indicate the potential for hypothesis-generation by integrating these global approaches, so that more selective methods may now be applied in future studies of their contributions to tumor biology and clinical outcome.
Abbreviations
- CGH:
-
comparative genomic hybridization
- CNA:
-
copy number aberration
- EEF1D:
-
eukaryotic translation elongation factor 1D
- qRT-RTPCR:
-
quantitative real-time reverse transcription polymerase chain reaction
- RPL30:
-
ribosomal protein L30
- RPS20:
-
ribosomal protein S20.
References
Strother DR, Pollack IF, Fisher PG, Hunter JV, Woo SY, Pomeroy SL, Rorke LB: Tumors of the Central Nervous System. Principles and Practice of Pediatric Oncology. Edited by: Pizzo P, Poplack D. 2003, 778-785. 4
Ellison D: Classifying the medulloblastoma: insights from morphology and molecular genetics. Neuropathol Appl Neurobiol. 2002, 28: 257-282. 10.1046/j.1365-2990.2002.00419.x.
Giangaspero F, Bigner SH, Giordana MT, Kleihues P, Trojanowski JQ: Medulloblastoma. Pathology and genetics: Tumours of the Nervous System. World Health Organization Classification of Tumors. 2000, 96-103.
Fernandez-Teijeiro A, Betensky RA, Sturla LM, Kim JY, Tamayo P, Pomeroy SL: Combining gene expression profiles and clinical parameters for risk stratification in medulloblastomas. J Clin Oncol. 2004, 22: 994-998. 10.1200/JCO.2004.03.036.
Gilbertson RJ, Gajjar A: Molecular biology of medulloblastoma: will it ever make a difference to clinical management?. J Neurooncol. 2005, 75: 273-278. 10.1007/s11060-005-6750-z.
Pomeroy SL, Tamayo P, Gaasenbeek M, Sturla LM, Angelo M, McLaughlin ME, Kim JY, Goumnerova LC, Black PM, Lau C, Allen JC, Zagzag D, Olson JM, Curran T, Wetmore C, Biegel JA, Poggio T, Mukherjee S, Rifkin R, Califano A, Stolovitzky G, Louis DN, Mesirov JP, Lander ES, Golub TR: Prediction of central nervous system embryonal tumour outcome based on gene expression. Nature. 2002, 415: 436-442. 10.1038/415436a.
Bayani J, Zielenska M, Marrano P, Kwan NY, Taylor MD, Jay V, Rutka JT, Squire JA: Molecular cytogenetic analysis of medulloblastomas and supratentorial primitive neuroectodermal tumors by using conventional banding, comparative genomic hybridization, and spectral karyotyping. J Neurosurg. 2000, 93: 437-448.
Eberhart CG, Kepner JL, Goldthwaite PT, Kun LE, Duffner PK, Friedman HS, Strother DR, Burger PC: Histopathologic grading of medulloblastomas: a Pediatric Oncology Group study. Cancer. 2002, 94: 552-560. 10.1002/cncr.10189.
Biegel JA: Cytogenetics and molecular genetics of childhood brain tumors. Neuro-oncol. 1999, 1: 139-151. 10.1215/15228517-1-2-139.
Pan E, Pellarin M, Holmes E, Smirnov I, Misra A, Eberhart CG, Burger PC, Biegel JA, Feuerstein BG: Isochromosome 17q is a negative prognostic factor in poor-risk childhood medulloblastoma patients. Clin Cancer Res. 2005, 11: 4733-4740. 10.1158/1078-0432.CCR-04-0465.
Gilhuis HJ, Anderl KL, Boerman RH, Jeuken JM, James CD, Raffel C, Scheithauer BW, Jenkins RB: Comparative genomic hybridization of medulloblastomas and clinical relevance: eleven new cases and a review of the literature. Clin Neurol Neurosurg. 2000, 102: 203-209. 10.1016/S0303-8467(00)00112-8.
Tong CY, Hui AB, Yin XL, Pang JC, Zhu XL, Poon WS, Ng HK: Detection of oncogene amplifications in medulloblastomas by comparative genomic hybridization and array-based comparative genomic hybridization. J Neurosurg. 2004, 100: 187-193.
Blaney SM, Boyett J, Friedman H, Gajjar A, Geyer R, Horowtiz M, Hunt D, Kieran M, Kun L, Packer R, Phillips P, Pollack IF, Prados M, Heideman R: Phase I clinical trial of mafosfamide in infants and children aged 3 years or younger with newly diagnosed embryonal tumors: a pediatric brain tumor consortium study (PBTC-001). J Clin Oncol. 2005, 23: 525-531. 10.1200/JCO.2005.06.544.
Duffner PK, Horowitz ME, Krischer JP, Friedman HS, Burger PC, Cohen ME, Sanford RA, Mulhern RK, James HE, Freeman CR, Seidel FG, Kun LE: Postoperative chemotherapy and delayed radiation in children less than three years of age with malignant brain tumors. N Engl J Med. 1993, 328: 1725-1731. 10.1056/NEJM199306173282401.
Packer RJ, Rood BR, Macdonald TJ: Medulloblastoma: present concepts of stratification into risk groups. Pediatr Neurosurg. 2003, 39: 60-67. 10.1159/000071316.
Thomas PR, Deutsch M, Kepner JL, Boyett JM, Krischer J, Aronin P, Albright L, Allen JC, Packer RJ, Linggood R, Mulhern R, Stehbens JA, Langston J, Stanley P, Duffner P, Rorke L, Cherlow J, Friedman HS, Finlay JL, Vietti TJ, Kun LE: Low-stage medulloblastoma: final analysis of trial comparing standard-dose with reduced-dose neuraxis irradiation. J Clin Oncol. 2000, 18: 3004-3011.
Strother D, Ashley D, Kellie SJ, Patel A, Jones-Wallace D, Thompson S, Heideman R, Benaim E, Krance R, Bowman L, Gajjar A: Feasibility of four consecutive high-dose chemotherapy cycles with stem-cell rescue for patients with newly diagnosed medulloblastoma or supratentorial primitive neuroectodermal tumor after craniospinal radiotherapy: results of a collaborative study. J Clin Oncol. 2001, 19: 2696-2704.
Sambrook J, Russell DW: Molecular Cloning, a Laboratory Manual. New York. 2001, 6.7-6.11; 6.27.
Kim JY, Sutton ME, Lu DJ, Cho TA, Goumnerova LC, Goritchenko L, Kaufman JR, Lam KK, Billet AL, Tarbell NJ, Wu J, Allen JC, Stiles CD, Segal RA, Pomeroy SL: Activation of neurotrophin-3 receptor TrkC induces apoptosis in medulloblastomas. Cancer Res. 1999, 59: 711-719.
Rao PH: Comparative genomic hybridization for analysis of changes in DNA copy number in multiple myeloma. Methods Mol Med. 2005, 113: 71-83.
Li C, Wong WH: Model-based analysis of oligonucleotide arrays: expression index computation and outlier detection. Proc Natl Acad Sci USA. 2001, 98: 31-36. 10.1073/pnas.011404098.
Pfaffl MW: A new mathematical model for relative quantification in real-time RT-PCR. Nucleic Acids Res. 2001, 29: e45-10.1093/nar/29.9.e45.
Dallas PB, Gottardo NG, Firth MJ, Beesley AH, Hoffmann K, Terry PA, Freitas JR, Boag JM, Cummings AJ, Kees UR: Gene expression levels assessed by oligonucleotide microarray analysis and quantitative real-time RT-PCR – how well do they correlate?. BMC Genomics. 2005, 6: 59-10.1186/1471-2164-6-59.
Batra SK, McLendon RE, Koo JS, Castelino-Prabhu S, Fuchs HE, Krischer JP, Friedman HS, Bigner DD, Bigner SH: Prognostic implications of chromosome 17p deletions in human medulloblastomas. J Neurooncol. 1995, 24: 39-45. 10.1007/BF01052657.
Cogen PH, McDonald JD: Tumor suppressor genes and medulloblastoma. J Neurooncol. 1996, 29: 103-112. 10.1007/BF00165523.
Gilbertson R, Wickramasinghe C, Hernan R, Balaji V, Hunt D, Jones-Wallace D, Crolla J, Perry R, Lunec J, Pearson A, Ellison D: Clinical and molecular stratification of disease risk in medulloblastoma. Br J Cancer. 2001, 85: 705-712. 10.1054/bjoc.2001.1987.
Lamont JM, McManamy CS, Pearson AD, Clifford SC, Ellison DW: Combined histopathological and molecular cytogenetic stratification of medulloblastoma patients. Clin Cancer Res. 2004, 10: 5482-5493. 10.1158/1078-0432.CCR-03-0721.
Mendrzyk F, Radlwimmer B, Joos S, Kokocinski F, Benner A, Stange DE, Neben K, Fiegler H, Carter NP, Reifenberger G, Korshunov A, Lichter P: Genomic and protein expression profiling identifies CDK6 as novel independent prognostic marker in medulloblastoma. J Clin Oncol. 2005, 23: 8853-8862. 10.1200/JCO.2005.02.8589.
Biegel JA, Janss AJ, Raffel C, Sutton L, Rorke LB, Harper JM, Phillips PC: Prognostic significance of chromosome 17p deletions in childhood primitive neuroectodermal tumors (medulloblastomas) of the central nervous system. Clin Cancer Res. 1997, 3: 473-478.
Emadian SM, McDonald JD, Gerken SC, Fults D: Correlation of chromosome 17p loss with clinical outcome in medulloblastoma. Clin Cancer Res. 1996, 2: 1559-1564.
Jung HL, Wang KC, Kim SK, Sung KW, Koo HH, Shin HY, Ahn HS, Shin HJ, Cho BK: Loss of heterozygosity analysis of chromosome 17p13.1-13.3 and its correlation with clinical outcome in medulloblastomas. J Neurooncol. 2004, 67: 41-46. 10.1023/B:NEON.0000021773.71127.fb.
Nicholson J, Wickramasinghe C, Ross F, Crolla J, Ellison D: Imbalances of chromosome 17 in medulloblastomas determined by comparative genomic hybridisation and fluorescence in situ hybridisation. Mol Pathol. 2000, 53: 313-319. 10.1136/mp.53.6.313.
Eberhart CG, Kratz J, Wang Y, Summers K, Stearns D, Cohen K, Dang CV, Burger PC: Histopathological and molecular prognostic markers in medulloblastoma: c-myc, N-myc, TrkC, and anaplasia. J Neuropathol Exp Neurol. 2004, 63: 441-449.
Joseph P, O'Kernick CM, Othumpangat S, Lei YX, Yuan BZ, Ong TM: Expression profile of eukaryotic translation factors in human cancer tissues and cell lines. Mol Carcinog. 2004, 40: 171-179. 10.1002/mc.20033.
Lei YX, Chen JK, Wu ZL: Blocking the translation elongation factor-1 delta with its antisense mRNA results in a significant reversal of its oncogenic potential. Teratog Carcinog Mutagen. 2002, 22: 377-383. 10.1002/tcm.10034.
Ogawa K, Utsunomiya T, Mimori K, Tanaka Y, Tanaka F, Inoue H, Murayama S, Mori M: Clinical significance of elongation factor-1 delta mRNA expression in oesophageal carcinoma. Br J Cancer. 2004, 91: 282-286. 10.1038/sj.bjc.6601992.
Ruggero D, Pandolfi PP: Does the ribosome translate cancer?. Nat Rev Cancer. 2003, 3: 179-192. 10.1038/nrc1015.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2407/6/223/prepub
Acknowledgements
We thank Linda L. Lin, Darlene G. Skapura, Jack M. Su, Meena Bhattacharjee, Murali Chintagumpala and Michael Sheldon for technical assistance; Cindy L. Nelson and Carolyn Pena for administrative assistance; and Angelo Rosolen for helpful discussions. This work was supported by funding from: Associazione Italiana contro le Leucemie (MDB); the Cancer Fighters of Houston, Inc. (CCL); the John S. Dunn Research Foundation; Hope Street Kids (JYHK); the Robert J. Kleberg, Jr. and Helen C. Kleberg Foundation; the Gillson Longenbaugh Foundation (CCL, JYHK); the National Children's Cancer Foundation/Children's Oncology Group Young Investigator Award (JYHK); NIH grants HD042977 (RCC), CA109467 and CA105607 (SLP), HD041648 and NS043517 (JYHK); and John and Carroll Goodman (JYHK).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
MDB, XYL, JD, LMS, and PHR performed CGH analysis. MDB, RCC, JD, LMS, SLP, CCL, TM, and JYHK contributed to gene expression analysis using microarrays and qRT-RTPCR. MDB, RCC, AMA, LP, SLP, and JYHK analyzed tumor pathology, clinical characteristics and outcomes. MDB, JD, TM, PHR, and JYHK analyzed and integrated genomic data. All of the authors made significant contributions to data interpretation and drafting of the manuscript.
Electronic supplementary material
12885_2006_575_MOESM1_ESM.pdf
Additional File 1: Multivariate Analysis of 8q Gain for Overall and Progression-Free Survival Controlled for Other Prognostic Variables. Multivariate analysis of significance was performed for 8q gain with respect to clinical variables that are widely accepted as prognostically significant: age relative to 3 years old and metastatic stage at diagnosis, and the degree of primary resection. These results confirm the prognostic significance of 8q gain for Overall and Progression-Free Survival (p = 0.013 and p = 0.003. respectively). Abbreviations: CGH8q, 8q gain; age_3, age relative to 3 years; resection, degree of resection; M_status, metastatic (Chang) stage; B, regression coefficient of the model; SE, standard error; df, degrees of freedom; Sig, significance (p value based on Wald statistics); Exp(B), exponential function of B. (PDF 16 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
De Bortoli, M., Castellino, R.C., Lu, XY. et al. Medulloblastoma outcome is adversely associated with overexpression of EEF1D, RPL30, and RPS20 on the long arm of chromosome 8. BMC Cancer 6, 223 (2006). https://doi.org/10.1186/1471-2407-6-223
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2407-6-223