
Abstracts
Background
IL-6 triggers oncogenic/angiogenic signals and the cytokine-dependent pro-cachexia cascade. The prognostic role of the functional IL-6 (promoter) rs1800795 and the IL-6R (receptor) rs8192284 single nucleotide polymorphisms (SNP) was studied in patients with advanced gastric cancer treated with palliative chemotherapy.
Methods
One-hundred-sixty-one patients were genotyped for rs1800795 and rs8192284 SNPs using polymerase chain reaction based restriction fragment length polymorphism (PCR-RFLP) analysis assay. These results were studied for association with overall survival (OS).
Results
In 161 assessable patients, frequencies of rs1800795 G/G, G/C and C/C genotypes were 46%, 42% and 12%, respectively. Frequencies of rs8192284 A/A, A/C and C/C genotypes were 36%, 45% and 19%, respectively. Carriers of the rs1800795 G/G and rs8192284 C/C genotypes showed the worst OS. In the multivariate model, rs1800795 G/G (1.69 hazard ratio; 95% confidence interval 1.18-2.42), and rs8192284 C/C (1.78 hazard ratio; 95% confidence interval 1.12-2.83) confirmed an adverse prognostic impact.
Conclusions
In this population, genetic variants that up-regulate the IL-6 system showed impact on OS. This findings sustain the hypothesis that anti-IL-6 compounds deserve clinical studies as novel therapeutics in the palliative treatment of cancer patients.
Similar content being viewed by others


Background
Interleukin-6 (IL-6) is a four-helical protein of 184 amino acids that belongs to a large family of pleiotropic cytokine involved in numerous functions [1]. On target cells, IL-6 binds to an 80 kDa IL-6 receptor (IL-6R). The complex of IL-6 and IL-6R couples with gp130 protein and triggers intracellular signaling. Whereas gp130 is expressed on all cells, IL-6R is only present on few cells in the body including hepatocytes and some leukocytes [1]. Cells not expressing IL-6R cannot respond to the cytokine, since gp130 alone has no measurable affinity for IL-6. A soluble form of IL-6R (sIL-6R) comprising the extracellular portion of the receptor can bind IL-6 with a similar affinity as the membrane bound IL-6R. The complex of IL-6 and sIL-6R can bind to gp130 on cells, which do not express the IL-6R, and which are unresponsive to IL-6 [1]. This alternative stimulation has been called trans-signaling [2]. There is evidence that IL-6 trans-signaling possess a prevalent pro-inflammatory role, whereas classic IL-6 signaling via the membrane bound IL-6R is needed for regenerative or anti-inflammatory processes [2].
Dysregulation of the IL-6/IL-6R system has been associated with the pathogenesis of several autoimmune and inflammatory diseases in humans, and anti-IL-6 monoclonal antibodies (moAbs) have been successfully developed for the medical treatment of chronic inflammatory diseases, like rheumatoid arthritis [3]. Recently, anti-IL-6 moAbs have drawn attention for their potential effects in cancer patients [4, 5]. On one side, IL-6 and other pro-inflammatory cytokines are involved in the mechanisms that promote cancer cachexia [6]. Also, there is evidence that IL-6 directly induces tumor growth and spread after triggering the canonical JAK/STAT pathway, an SHP-2 driven Ras-Raf-MAPK signaling pathway and angiogenesis [4, 5]. Activation of these pathways has been documented in gastric cancer in experimental models and in vivo[7–16].
There is compelling evidence that circulating IL-6 levels and the levels of its trans-signaling promoting receptor (sIL-6R) are genetically-driven [17]. The single nucleotide polymorphism (SNP) rs1800795 corresponding to -174G/C SNP in the IL-6 gene promoter showed higher transcriptional activity in gene reporter assays [18]. In vivo, higher IL-6 levels were determined in carriers of the common allele in studies including both healthy subjects and patients with inflammatory diseases [18]. A common non-synonymous variant in IL-6R (rs8192284 A-C, also rs2228145) causes an Asp358Ala amino acid substitution within the extracellular cleavage domain of the IL-6R causing proteolytic cleavage of the membrane-bound IL-6R [19]. In in vivo studies, 358Ala carriers showed higher concentrations of the so-called soluble IL-6 receptor (sIL-6R), which is responsible of trans-signaling [19].
In several reports, an up-regulated IL-6/IL6R system has shown a prognostic impact in patients with hematologic malignancies and with solid tumors [20]. This background and the availability of novel IL-6 targeting moAbs [5] prompted us to investigate the possible influence of rs1800795 and rs8192284 on survival of patients with advanced gastric cancer. This information, beyond addressing a novel prognostic factor, may be relevant for the planning of clinical trials with anti-IL-6 therapies in this lethal disease.
Methods
The study population consisted of consecutive patients with locally advanced, relapsed of metastatic gastric cancer who were treated with palliative chemotherapy at three participating Institution in Central Italy. One-hundred-seventy-five patients were homogeneously treated with both first-line and second-line palliative chemotherapy between 1998 and 2006 [21]. In 161 of 175 patients (92%) germline DNA was available from stored blood samples or obtained after DNA extraction from normal mucosa from archival paraffin-embedded tissues. Data on chemotherapy, treatment outcomes, baseline characteristics with routine blood chemistries, and follow-up were fully available for the 161 assessed patients. The study approval by the main hospital research and ethics committee (Azienda Ospedaliera “Ospedali Riuniti Marche Nord”, Pesaro) was granted by those of affiliate Institutions (University of Urbino and Campus Biomedico, Rome). Patients gave their general consent for the storage of their tissues and subsenquent use for research purposes.
Genetic analyses
Patients’ characteristics and their outcomes were unknown to investigators performing genetic analyses. Genomic DNA extraction using the QiaAmp kit (Qiagen, Valencia, CA, USA). A polymerase chain reaction (PCR)–restriction fragment length polymorphism (RFLP) technique was used for determining the IL-6R rs8192284 A/C and the IL-6 rs1800795 G/C genotypes. Genome DNA (10 ng) was used as a template and PCR was carried out using the Diatheva 2×PCR Master Mix (Diatheva, Fano, Italy) with the following conditions: 95°C 10 min ; 95°C 15 sec, 60°C 30 sec, 72°C 30 sec (35 cycles). The two PCR were performed using the following primer sets: rs1800795, forward 5’-TTCCCCCTAGTTGTGTCTTGC-3’ and reverse 5’-TGGGGCTGATTGGAAACCT-3’; rs8192284 forward 5’-CCTCTTCCTCCTCTATCTTCAATTTT-3’ and reverse 5’-AATGTGGGCAGTGGTACTGAA-3’. Primer pairs were designed using the PRIMER3 program (primer3plus.com ). The PCR products were run on a 2% agarose gel after digestion with Nla-III (IL-6, rs1800795 G/C) or Hind-III (IL-6R, rs8192284 A/C) restriction enzymes. The predicted band sizes for the rs1800795 G/C genotypes after Nla-III digestion were G/G = 75 bp; G/C = 75 bp plus 50/25 bp; C/C = 50/25 bp; the predicted band sizes for the rs8192284 A/C genotypes after Hind-III digestion were A/A = 73; A/C = 73 bp plus 43/30 bp; C/C = 43/30 bp. Samples with ambiguous results were analyzed by direct sequencing using ABI PRISM 310 Genetic Analyzer (Applied Biosystems, Foster City CA).
Statistical plan
The primary endpoint of the study was the association between genotypes and overall survival (OS), as calculated from the start of first-line palliative chemotherapy until death. Genotypes were checked for deviation from the Hardy-Weinberg equilibrium using the Pearson X2 test. The X2 test and the Fisher's exact test were used to test associations between genotypes and categorical variables describing the clinico-pathologic features of the study population. Survival curves were plotted using the Kaplan-Meier and compared using the log-rank test. The Cox proportional hazards model was used for multivariate analysis to estimate and test demographic characteristics, clinical and genetic features for their associations with OS. In this exploratory study, no formal correction for multiple comparisons was adopted. However, all the following variables were included in multivariate Cox model: age, sex, ECOG performance status, weight loss (>5% in the four weeks before starting chemotherapy), anemia, albumin level, CEA level, tumor grading, histologic subtype according to Lauren’s classification, tumor location, liver involvement, presence of peritoneal carcinomatosis, number of metastatic sites and response to first-line chemotherapy. Assuming a 20% lowest frequency for an unfavorable genotype, 157 events would allow to detect an Hazard Ratio (HR) of 1.75 associated with this group (80% power and 5% type I error for a two-tailed test). All results were considered significant at two-sided p < .05 value. All analyses were performed by using the MedCalc software version 11.1 (MedCalc Software, Ostend, Belgium).
Results
Characteristics of patients and genotyping
One-hundred-sixty-one patients were analyzed. All of them received first and second-line chemotherapy and died after gastric cancer progression. First-line chemotherapy was oxaliplatin or cisplatin plus a fluoropyrimidne in 150 patients, or bolus/infusional 5-Fluorouracil in 11 patients. Second-line chemotherapy was 5-Fluorouracil coupled with cisplatin or oxaliplatin in 48 patients, with CPT-11 in 45 patients, with anthracycline in 33 patients, with paclitaxel or docetaxel in 25 patients, with VP-16 in 10 patients. Median survival time in the whole group was 9.4 months (range 0.4-34 months).
Carriers of the rs1800795 G/G, G/C and C/C genotypes were 74 (46%), 68 (42%) and 19 (12%), respectively. Carriers of the rs8192284 A/A, A/C and C/C genotypes were 58 (36%), 73 (45%) and 30 (19%), respectively. These frequencies did not show deviation from Hardy-Weinberg equilibrium and they are comparable with frequencies commonly observed in Caucasian populations.
Details of the characteristics of enrolled patients together with their distribution according to rs1800795 and rs8192284 genotypes are shown in Table 1. No significant association was observed except for liver involvement and rs8192284 genotypes. In particular, rs8192284 C/C carriers were prevalent in patients with liver metastases, while rs8192284 A/A carriers were prevalent in patients without liver metastases (Table 1).
Survival analyses
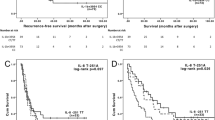
Survival curves of carriers of the rs1800795 and rs8192284 genotypes are shown in Figure 1. In carriers of the rs1800795 G/G, G/C and C/C genotypes, median survival times were 8.4, 11 and 12.6 months, respectively (p = 0.01). In carriers of the rs8192284 A/A, A/C and C/C genotypes median survival times were 11.7, 10.1 and 8.6 months, respectively (p = 0.01).

Survival analysis with distribution of patients according to rs1800795 genotypes (Panel A) and rs8192284 genotypes (Panel B).
The recessive model was adopted in the multivariate analysis with rs1800795 G/G and rs8192284 C/C defined as the risk genotypes. As shown in Table 2, harboring rs1800795 G/G (1.69 hazard ratio with 95% confidence interval 1.18-2.42), or rs8192284 C/C (1.78 hazard ratio with 95% confidence interval 1.12-2.83) confirmed an adverse impact on OS. Unfavorable survival outcomes were also significantly associated with poor performance status, lack of tumor response to first-line chemotherapy, >2 metastatic sites and the presence of peritoneal carcinomatosis.
An additional explorative survival analysis was addressed to the distribution of the rs1800795 G and rs8192284 C risk alleles. There were 16 patients (10%) who were carriers of both unfavorable rs1800795 G/G and rs8192284 C/C genotypes (4 risk alleles group). Eight patients (5%) with rs1800795 C/C and rs8192284 A/A genotypes were classified without risk alleles (0 risk allele group). Twenty-nine (18%), 68 (42%) and 40 (25%) patients were grouped as carriers of 1 risk allele, 2 risk alleles, or 3 risk alleles. As shown in Figure 2, patients with 4 risk alleles showed the worst OS.

Exploratory survival analysis with classification of patients in five groups according to the number of risk alleles as defined after the primary survival analysis.
Discussion
Clinical studies have demonstrated that increased serum IL-6 concentrations are associated with advanced tumor stages and short survival in patients with solid neoplasms [20]. IL-6 is a potent pleyotropic cytokine that may enhance a pro-inflammatory status and promote mechanisms leading to cancer cachexia in the host [1]. Also, IL-6 directly induces tumor growth and spread after triggering the canonical JAK/STAT pathway, as well as the SHP-2 driven Ras-Raf-MAPK signaling pathway and tumor angiogenesis [2–5]. Because of the restricted expression of the membrane-bound IL-6 receptor, lymphocytes and hepatocytes are the main IL-6 target cells. This pattern of receptor expression should limit the amount of cells that can respond to IL-6. However, the expression of the membrane-bound IL-6R may increase in cancer cells and alternative mechanisms may induce detrimental activation of the IL-6 system [22]. In fact, shedding of the membrane bound form into the local microenvironment, with production of the soluble form of the IL-6 receptor (sIL-6R) triggers trans-signalling, which in turn greatly increases the range of cells that can respond to IL-6 [22]. Some data indicate that sIL-6R may also act as an “orphan” molecule without complexing with IL-6 and gp130 [2]. However, the main effects of the sIL-6R seem to be agonistic with activation of trans-signaling in the presence of IL-6 [23].
There is evidence that the level of activity of IL-6 and its receptor are regulated by functional polymorphisms in the corresponding genes [17]. The common allele of a SNP in IL-6 promoter (rs1800795 G > C) enhances serum concentrations of IL-6 [18], while the minor allele in IL6R (rs8192284 A > C) is a strong inducer of the soluble form of the IL-6 receptor (sIL-6R) [19]. The minor IL6R allele also causes an increase in IL-6 circulating levels, but it seems an indirect effect resulting from reduced IL-6 clearance through membrane-bound IL-6R [19]. Carriers of genetic variants that up-regulate IL-6 and sIL-6R secretion may represent sub-groups of patients with a host-related feature that favors tumor growth, metastatic spread and cancer cachexia. Notably, we found that the common G allele of the IL-6 promoter variant (rs1800795) showed association with poor survival of patients with advanced gastric cancer treated with palliative chemotherapy. The minor IL-6R C allele (rs8192284) showed a weaker prognostic role than the IL-6 promoter variant. However, in support of a “dynamic” modulation of the IL-6/sIL-6R system, we observed a possible additive effect with worst survival outcomes in the presence of both IL-6 and IL-6R unfavorable genotypes (Figure 2).
The different distribution of patients with and without liver metastasis according to the sIL-6R genotypes would also support the role of the IL-6/IL-6R system in the acquisition of a specific pattern of metastatic spread [24]. In experimental and in vivo models, IL-6 increases the metastatic potential of circulating tumor cells and modulates tissue homeostasis in a target organ of metastasis such as the liver [25]. Also, sIL-6R-mediated trans-signaling displays pro-invasive and pro-metastatic signals [1, 2]. It is maximized in rs8192284 IL-6R minor allele carriers and it is likely to promote hematogenous spread, causing a specific pattern of metastatic disease [26].
The common G allele of the rs1800795 IL-6 promoter variant showed association with unfavorable survival outcomes of patients with ovarian cancer [27], breast cancer [28, 29], neuroblastoma [30] and hematologic malignancies [31]. To the best of our knowledge, there is only one published study reporting the results of a prognostic analysis of IL-6 polymorphisms in gastric cancer patients [32]. Liao et al [32] showed a significant association between high IL-6 circulating levels and poor survival of stage II-III, surgically resected patients, but the rs1800796 IL-6 variant did not show prognostic role. Notably, they could not investigate the IL-6 rs1800795 because of the rarity of the variant allele in Asiatic populations [32], while the functional effects of the IL-6 rs1800796 are less extensively studied compared with the IL-6 rs1800795.
Less information is available on the clinical impact of the rs8192284 IL-6R genetic variant. In multiple myeloma patients the minor rs8192284 C allele showed association with lower overall survival [33], but in neuroblastoma patients it did not show prognostic role [31]. According to the physiology of trans-signaling and recent data on agonistic and antagonistic properties of sIL-6R [34], it is likely that sIL-6R and IL-6R genetic variants may display variable clinical effects depending on tumor type, tumor stage, concomitant treatments, host related features involving the immune system and the fine tuning of other cytokines.
Clinical data on the activation of the IL-6/IL-6R system should be considered beyond the possible prognostic role. In fact, the effects of IL-6/IL-6R may contribute to explain different sensitivity and clinical outcomes of patients treated with novel target therapies. At the same time, IL-6/IL-6R analyses could offer the opportunity of developing an alternative therapeutic strategy. In patients with metastatic renal cell cancer, high IL-6 serum levels were predictive of improved progression-free survival from the multi-kinase inhibitor Pazopanib compared with placebo [35]. In experimental models, IL-6 showed induction of cancer stem cells and epithelial-mesenchimal transition phenotype, which are possible condition for resistance to the anti-HER-2 compounds trastuzumab and lapatinib [36, 37]. High IL-6 levels showed association with toxicity from Vorinostat in prostate cancer patients [38]. Anti-IL-6 molecules may counteract this, and other detrimental effects enhanced by the up-regulation of the IL-6 system. Tocilizumab, Sirukumab and Siltuximab are three MoAbs currently under investigations in clinical trials in cancer patients [5]. Ando et al [39] and Hirata et al [40] in recently published case reports, described the favorable effects on cancer cachexia and disease-related symptoms of Toclizumab in an heavily pre-treated cancer patients. Preliminary data from Phase I-II studies of anti-IL-6 in patients with multiple myeloma, castration-resistant prostate cancer and other solid tumors indicate the possible development of anti-IL-6 in cancer patients [41–43].
Conclusion
Limitations of this study are its retrospective nature and the lack of a concomitant analysis of the cytokines circulating levels. Therefore, additional studies are needed for confirming the prognostic role of IL-6 analyses, and for corroborating the hypothesis that subjects with elevated baseline IL-6 levels and/or an IL-6 enhancing genetic profile may represent the target population for evaluating the effects of the anti-IL-6 MoAbs in cancer patients.
Abbreviations
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- ECOG PS:
-
Eastern Cooperative Oncology Group Performance Status
- RR:
-
Response rate
- CR:
-
Complete response
- PR:
-
Partial response
- SD:
-
Stable disease
- PD:
-
Progressive disease
- Mets:
-
metastasis
- LA/LR:
-
Locally advanced/local relapse.
References
Scheller J, Chalaris A, Schmidt-Arras D, Rose-John S: The pro- and anti-inflammatory properties of the cytokine interleukin-6. Biochim Biophys Acta. 1813, 2011: 878-888.
Rose-John S: IL-6 trans-signaling via the soluble IL-6 receptor: importance for the pro-inflammatory activities of IL-6. Int J Biol Sci. 2012, 8: 1237-1247. 10.7150/ijbs.4989.
Tanaka T, Kishimoto T: Targeting interleukin-6: all the way to treat autoimmune and inflammatory diseases. Int J Biol Sci. 2012, 8: 1227-1236. 10.7150/ijbs.4666.
Guo Y, Xu F, Lu T, Duan Z, Zhang Z: Interleukin-6 signaling pathway in targeted therapy for cancer. Cancer Treat Rev. 2012, 38: 904-910. 10.1016/j.ctrv.2012.04.007.
Sansone P, Bromberg J: Targeting the interleukin-6/Jak/stat pathway in human malignancies. J Clin Oncol. 2012, 30: 1005-1014. 10.1200/JCO.2010.31.8907.
Fearon KC, Glass DJ, Guttridge DC: Cancer cachexia: mediators, signaling, and metabolic pathways. Cell Metab. 2012, 16: 153-166. 10.1016/j.cmet.2012.06.011.
Kinoshita H, Hirata Y, Nakagawa H, Sakamoto K, Hayakawa Y, Takahashi R, Nakata W, Sakitani K, Serizawa T, Hikiba Y, Akanuma M, Shibata W, Maeda S, Koike K: Interleukin-6 mediates epithelial-stromal interactions and promotes gastric tumorigenesis. PLoS One. 2013, 8: e60914-10.1371/journal.pone.0060914.
Okamoto W, Okamoto I, Arao T, Yanagihara K, Nishio K, Nakagawa K: Differential roles of STAT3 depending on the mechanism of STAT3 activation in gastric cancer cells. Br J Cancer. 2011, 105: 407-412. 10.1038/bjc.2011.246.
Mejías-Luque R, Peiró S, Vincent A, Van Seuningen I, de Bolós C: IL-6 induces MUC4 expression through gp130/STAT3 pathway in gastric cancer cell lines. Biochim Biophys Acta. 2008, 1783: 1728-1736. 10.1016/j.bbamcr.2008.05.020.
Jackson CB, Judd LM, Menheniott TR, Kronborg I, Dow C, Yeomans ND, Jackson CB, Judd LM, Menheniott TR, Kronborg I, Dow C, Yeomans ND, Boussioutas A, Robb L, Giraud AS: Augmented gp130-mediated cytokine signalling accompanies human gastric cancer progression. J Pathol. 2007, 213: 140-151. 10.1002/path.2218.
Lin MT, Lin BR, Chang CC, Chu CY, Su HJ, Chen ST, Jeng YM, Kuo ML: IL-6 induces AGS gastric cancer cell invasion via activation of the c-Src/RhoA/ROCK signaling pathway. Int J Cancer. 2007, 120: 2600-2608. 10.1002/ijc.22599.
Howlett M, Judd LM, Jenkins B, La Gruta NL, Grail D, Ernst M, Giraud AS: Differential regulation of gastric tumor growth by cytokines that signal exclusively through the coreceptor gp130. Gastroenterology. 2005, 129: 1005-1018. 10.1053/j.gastro.2005.06.068.
Huang SP, Wu MS, Shun CT, Wang HP, Lin MT, Kuo ML, Lin JT: Interleukin-6 increases vascular endothelial growth factor and angiogenesis in gastric carcinoma. J Biomed Sci. 2004, 11: 517-527. 10.1007/BF02256101.
Huang SP, Wu MS, Wang HP, Yang CS, Kuo ML, Lin JT: Correlation between serum levels of interleukin-6 and vascular endothelial growth factor in gastric carcinoma. J Gastroenterol Hepatol. 2002, 17: 1165-1169. 10.1046/j.1440-1746.2002.02873.x.
Kim DK, Oh SY, Kwon HC, Lee S, Kwon KA, Kim BG, Kim SG, Kim SH, Jang JS, Kim MC, Kim KH, Han JY, Kim HJ: Clinical significances of preoperative serum interleukin-6 and C-reactive protein level in operable gastric cancer. BMC Cancer. 2009, 9: 155-10.1186/1471-2407-9-155.
Kim HK, Song KS, Park YS, Kang YH, Lee YJ, Lee KR, Kim HK, Ryu KW, Bae JM, Kim S: Elevated levels of circulating platelet microparticles, VEGF, IL-6 and RANTES in patients with gastric cancer: possible role of a metastasis predictor. Eur J Cancer. 2003, 39: 184-191. 10.1016/S0959-8049(02)00596-8.
Smith AJ, Humphries SE: Cytokine and cytokine receptor gene polymorphisms and their functionality. Cytokine Growth Factor Rev. 2009, 20: 43-59. 10.1016/j.cytogfr.2008.11.006.
Woo P, Humphries SE: IL-6 polymorphisms: a useful genetic tool for inflammation research?. J Clin Invest. 2013, 123: 1413-1414. 10.1172/JCI67221.
Ferreira RC, Freitag DF, Cutler AJ, Howson JM, Rainbow DB, Smyth DJ, Kaptoge S, Clarke P, Boreham C, Coulson RM, Pekalski ML, Chen WM, Onengut-Gumuscu S, Rich SS, Butterworth AS, Malarstig A, Danesh J, Todd JA: Functional IL6R 358Ala allele impairs classical IL-6 receptor signaling and influences risk of diverse inflammatory diseases. PLoS Genet. 2013, 9: e1003444-10.1371/journal.pgen.1003444.
Lippitz BE: Cytokine patterns in patients with cancer: a systematic review. Lancet Oncol. 2013, 14: e218-28. 10.1016/S1470-2045(12)70582-X.
Catalano V, Graziano F, Santini D, D'Emidio S, Baldelli AM, Rossi D, Vincenzi B, Giordani P, Alessandroni P, Testa E, Tonini G, Catalano G: Second -line chemotherapy for patients with advanced gastric cancer: who may benefit?. Br J Cancer. 2008, 99: 1402-1407. 10.1038/sj.bjc.6604732.
Lo CW, Chen MW, Hsiao M, Wang S, Chen CA, Hsiao SM, Chang JS, Lai TC, Rose-John S, Kuo ML, Wei LH: IL-6 trans-signaling in formation and progression of malignant ascites in ovarian cancer. Cancer Res. 2011, 71: 424-434. 10.1158/0008-5472.CAN-10-1496.
Waetzig GH, Rose-John S: Hitting a complex target: an update on interleukin-6 trans-signalling. Expert Opin Ther Targets. 2012, 16: 225-236. 10.1517/14728222.2012.660307.
Van den Eynden GG, Majeed AW, Illemann M, Vermeulen PB, Bird NC, Høyer-Hansen G, Eefsen RL, Reynolds AR, Brodt P: The multifaceted role of the microenvironment in liver metastasis: biology and clinical implications. Cancer Res. 2013, 73: 2031-2043. 10.1158/0008-5472.CAN-12-3931.
Li S, Wang N, Brodt P: Metastatic cells can escape the proapoptotic effects of TNF-α through increased autocrine IL-6/STAT3 signaling. Cancer Res. 2012, 72: 865-875. 10.1158/0008-5472.CAN-11-1357.
Ashizawa T, Okada R, Suzuki Y, Takagi M, Yamazaki T, Sumi T, Aoki T, Ohnuma S, Aoki T: Clinical significance of interleukin-6 (IL-6) in the spread of gastric cancer: role of IL-6 as a prognostic factor. Gastric Cancer. 2005, 8: 124-131. 10.1007/s10120-005-0315-x.
Hefler LA, Grimm C, Ackermann S, Malur S, Radjabi-Rahat AR, Leodolter S, Beckmann MW, Zeillinger R, Koelbl H, Tempfer CB: An interleukin-6 gene promoter polymorphism influences the biological phenotype of ovarian cancer. Cancer Res. 2003, 63: 3066-3068.
DeMichele A, Martin AM, Mick R, Gor P, Wray L, Klein-Cabral M, Athanasiadis G, Colligan T, Stadtmauer E, Weber B: Interleukin-6-174G- > C polymorphism is associated with improved outcome in high-risk breast cancer. Cancer Res. 2003, 63: 8051-8056.
DeMichele A, Gray R, Horn M, Chen J, Aplenc R, Vaughan WP, Tallman MS: Host genetic variants in the interleukin-6 promoter predict poor outcome in patients with estrogen receptor-positive, node-positive breast cancer. Cancer Res. 2009, 69: 4184-4191. 10.1158/0008-5472.CAN-08-2989.
Lagmay JP, London WB, Gross TG, Termuhlen A, Sullivan N, Axel A, Mundy B, Ranalli M, Canner J, McGrady P, Hall B: Prognostic significance of interleukin-6 single nucleotide polymorphism genotypes in neuroblastoma: rs1800795 (promoter) and rs8192284 (receptor). Clin Cancer Res. 2009, 15: 5234-5239. 10.1158/1078-0432.CCR-08-2953.
Hohaus S, Giachelia M, Di Febo A, Martini M, Massini G, Vannata B, D’Alo’ F, Guidi F, Greco M, Pierconti F, Larocca LM, Voso MT, Leone G: Polymorphism in cytokine genes as prognostic markers in Hodgkin's lymphoma. Ann Oncol. 2007, 18: 1376-1381. 10.1093/annonc/mdm132.
Liao WC, Lin JT, Wu CY, Huang SP, Lin MT, Wu AS, Huang YJ, Wu MS: Serum interleukin-6 level but not genotype predicts survival after resection in stages II and III gastric carcinoma. Clin Cancer Res. 2008, 14: 428-434. 10.1158/1078-0432.CCR-07-1032.
Stephens OW, Zhang Q, Qu P, Zhou Y, Chavan S, Tian E, Williams DR, Epstein J, Barlogie B, Shaughnessy JD: An intermediate-risk multiple myeloma subgroup is defined by sIL-6r: levels synergistically increase with incidence of SNP rs2228145 and 1q21 amplification. Blood. 2012, 119: 503-512. 10.1182/blood-2011-07-367052.
Knüpfer H, Preiss R: sIL-6R: more than an agonist?. Immunol Cell Biol. 2008, 86: 87-91. 10.1038/sj.icb.7100113.
Tran HT, Liu Y, Zurita AJ, Lin Y, Baker-Neblett KL, Martin AM, Figlin RA, Hutson TE, Sternberg CN, Amado RG, Pandite LN, Heymach JV: Prognostic or predictive plasma cytokines and angiogenic factors for patients treated with pazopanib for metastatic renal-cell cancer: a retrospective analysis of phase 2 and phase 3 trials. Lancet Oncol. 2012, 13: 827-837. 10.1016/S1470-2045(12)70241-3.
Korkaya H, Kim GI, Davis A, Malik F, Henry NL, Ithimakin S, Korkaya H, Kim GI, Davis A, Malik F, Henry NL, Ithimakin S, Quraishi AA, Tawakkol N, D'Angelo R, Paulson AK, Chung S, Luther T, Paholak HJ, Liu S, Hassan KA, Zen Q, Clouthier SG, Wicha MS: Activation of an IL6 inflammatory loop mediates trastuzumab resistance in HER2+ breast cancer by expanding the cancer stem cell population. Mol Cell. 2012, 47: 570-584. 10.1016/j.molcel.2012.06.014.
Sullivan NJ, Sasser AK, Axel AE, Vesuna F, Raman V, Ramirez N, Oberyszyn TM, Hall BM: Interleukin-6 induces an epithelial-mesenchymal transition phenotype in human breast cancer cells. Oncogene. 2009, 28: 2940-2947. 10.1038/onc.2009.180.
Bradley D, Rathkopf D, Dunn R, Stadler WM, Liu G, Smith DC, Pili R, Zwiebel J, Scher H, Hussain M: Vorinostat in advanced prostate cancer patients progressing on prior chemotherapy (National Cancer Institute Trial 6862): trial results and interleukin-6 analysis: a study by the Department of Defense Prostate Cancer Clinical Trial Consortium and University of Chicago Phase 2 Consortium. Cancer. 2009, 115: 5541-5549. 10.1002/cncr.24597.
Ando K, Takahashi F, Motojima S, Nakashima K, Kaneko N, Hoshi K, Takahashi K: Possible role for tocilizumab, an anti-interleukin-6 receptor antibody, in treating cancer cachexia. J Clin Oncol. 2013, 31: e69-72. 10.1200/JCO.2012.44.2020.
Hirata H, Tetsumoto S, Kijima T, Kida H, Kumagai T, Takahashi R, Otani Y, Inoue K, Kuhara H, Shimada K, Nagatomo I, Takeda Y, Goya S, Yoshizaki K, Kawase I, Tachibana I, Kishimoto T, Kumanogoh A: Favorable Responses to Tocilizumab in Two Patients With Cancer-Related Cachexia. J Pain Symptom Manage. 2013, 46: e9-e13. 10.1016/j.jpainsymman.2013.01.009.
Kurzrock R, Voorhees PM, Casper C, Furman RR, Fayad L, Lonial S, Kurzrock R, Voorhees PM, Casper C, Furman RR, Fayad L, Lonial S, Borghaei H, Jagannath S, Sokol L, Usmani SZ, van de Velde H, Qin X, Puchalski TA, Hall B, Reddy M, Qi M, van Rhee F: A Phase I, Open-Label Study of Siltuximab, anAnti-IL-6 Monoclonal Antibody, in Patients with B-cell Non-Hodgkin Lymphoma, Multiple Myeloma, or Castleman Disease. Clin Cancer Res. 2013, 19: 3659-3670. 10.1158/1078-0432.CCR-12-3349.
Hudes G, Tagawa ST, Whang YE, Qi M, Qin X, Puchalski TA, Reddy M, Cornfeld M, Eisenberger M: A phase 1 study of a chimeric monoclonal antibody against interleukin-6, siltuximab, combined with docetaxel in patients with metastatic castration-resistant prostate cancer. Invest New Drugs. 2013, 31: 669-676. 10.1007/s10637-012-9857-z.
Bayliss TJ, Smith JT, Schuster M, Dragnev KH, Rigas JR: A humanized anti-IL-6 antibody (ALD518) in non-small cell lung cancer. Expert Opin Biol Ther. 2011, 11: 1663-1668. 10.1517/14712598.2011.627850.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2407/14/357/prepub
Acknowledgements
This work was supported by FanoAteneo, Diatheva srl and POR MARCHE FESR 2007–2013.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declared that they have no competing interests.
Authors’ contributions
AR, EC, EG, MM and FG conceived and designed the experiments. VC, DS, GT, BV, GF and FG provided the samples. AR, EC, EG, MM and FG analyzed and interpreted the data. AR, EG, MM and FG contributed in the writing of the manuscript. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Ruzzo, A., Catalano, V., Canestrari, E. et al. Genetic modulation of the interleukin 6 (IL-6) system in patients with advanced gastric cancer: a background for an alternative target therapy. BMC Cancer 14, 357 (2014). https://doi.org/10.1186/1471-2407-14-357
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2407-14-357