
Abstract
Background
This study aimed to elucidate the phenotypic, immunologic, and clinical characteristics of Korean patients with nontuberculous mycobacterial (NTM) lung disease and compare them with non-NTM bronchiectasis (BE) patients.
Methods
We prospectively recruited patients between 20 and 80 years of age who had nodular BE type NTM lung disease. Phenotypic, immunologic, and clinical characteristics were evaluated through physical examination, laboratory tests, pulmonary function tests, and radiographic examinations. Questionnaires were also answered. The results of the evaluations were compared with the results of non-NTM BE patients.
Results
A total of 84 patients with NTM lung disease and 47 non-NTM BE patients participated in the study. Mycobacterium avium complex lung disease and M. abscessus lung disease were most common. Patients with NTM lung disease had lower body mass index than non-NTM BE patients. Scoliosis was observed more frequently in patients with NTM lung disease than in non-NTM BE patients.
Conclusions
Significant similarities were seen between Korean patients with NTM lung disease and patients from other countries. Differences in phenotypic and clinical characteristics between NTM lung disease and non-NTM BE patients suggest differences in the immunopathogenesis of NTM lung disease and non-NTM BE.
Trial registration information
ClinicalTrials.gov Registration number; NCT01616745
Similar content being viewed by others


Background
Nontuberculous mycobacteria (NTM) are environmentally ubiquitous organisms, and rarely cause disease in healthy individuals. Rates of NTM isolation, as well as the number of patients with NTM lung disease, have been increasing worldwide [1]; however, the fact that only a small number of people contract NTM despite ubiquitous exposure suggests the presence of identifiable risk factors associated with NTM infection.
While the immunopathogenesis of NTM lung disease remains largely unknown, certain phenotypic and immunologic characteristics of patients with NTM lung disease have been observed. A single nucleotide polymorphism in TLR2 has been linked to NTM lung diseases [2], and IFN-γ and IL-10 secretions have been reported to be suppressed among patients with NTM lung disease [3]. Furthermore, patients with NTM lung disease tend to be taller and leaner on average, with relatively high frequencies of scoliosis, pectus excavatum, and mitral valve prolapse [4].
While the incidence of tuberculosis has been in steady decline across South Korea, the rate of NTM isolation has increased rapidly [5]. The aim of this study was to elucidate the phenotypic, immunologic, and clinical characteristics of Korean patients with NTM lung diseases through comparisons with non-NTM bronchiectasis (BE) patients.
Methods
Study cohort
Beginning July 1, 2011 we prospectively recruited patients between 20 and 80 years of age at Seoul National University Hospital, Seoul, South Korea, who met the diagnostic criteria for NTM lung disease set forth by the American Thoracic Society [6]. Patients previously treated for NTM lung disease were excluded from this study. NTM patients with nodular BE types were included but those with upper lobe cavitary types were excluded. All patients provided written informed consent before enrollment. The study protocol was approved by the Institutional Review Board of Seoul National University Hospital. The clinical trial registration number is NCT 01616745 (www.ClinicalTrials.gov).
Control group
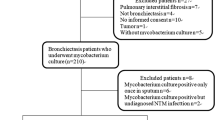
Beginning January 1, 2012 we began recruiting patients ≥ 20 years old diagnosed with BE in the absence of NTM infection (non-NTM) to serve as a control group. BE was diagnosed based on low dose computed tomography (CT) findings that included dilatation of an airway lumen, rendering it more than 1.5 times the width of a nearby vessel, lack of tapering of an airway toward the periphery, varicose constrictions along airways, and ballooned cysts at the end of a bronchus [7]. Two separate sputum mycobacterial cultures were performed to exclude patients with active NTM infections. The median interval between the two cultures was 24 months (interquartile range: 9–55 months).
Physical examinations
Physical examinations were performed by board-certified physicians. Height and weight were measured by a team of two nurses.
Microbiological tests
Sputum was collected for bacterial and mycobacterial cultures. Samples of sputum were homogenized by incubation at 37°C for 15 min with an equal volume of 0.1% dithiothreitol (Sputolysin; Calbiochem Corp., San Diego, CA, USA). Homogenized sputum was sequentially diluted and placed in phosphate-buffered saline and plated on blood, chocolate, and MacConkey agar plates. Sputum isolates were classified as potential pathogens or as normal flora. Potential pathogens were Haemophilus influenzae, Moraxella catarrhalis, Streptococcus pneumoniae, Pseudomonas aeruginosa, Staphylococcus aureus, and other gram-negative rods; other bacterial species were classified as normal flora [8].
Sputum and bronchial washing fluid were decontaminated with 4% sodium hydroxide, homogenized, and concentrated by centrifugation at 3000 × g for 20 min. The specimens were stained using the Ziehl–Nielsen method [6]. Concentrated specimens were cultured in 3% Ogawa medium and observed weekly for 9 weeks after inoculation. Following isolation of a suspected mycobacterial species, confirmation of NTM was performed by analyzing the sequences of three genes; 16S rRNA, rpoB and tuf. Polymerase chain reaction and subsequent sequencing were performed, and the resulting sequences were compared with the reference database using basic local alignment search tools. Mycobacterial species were identified using 16S rRNA sequences, using the algorithm described in Clinical and Laboratory Standards Institute guideline MM18-A [9].
Laboratory tests
Laboratory tests consisted of the following: leukocyte count including differential counts, hematocrit, hemoglobin, platelet count, total cholesterol, total protein, albumin, total and direct bilirubin, alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, blood urea nitrogen, creatinine, electrolytes, erythrocyte sedimentation rate, C-reactive protein, fluorescent antinuclear antibody test (FANA), rheumatoid factor, serum immunoglobulins (IgG, IgA, IgM), and IFN-γ release assay (IGRA).
Pulmonary function tests and radiographic examination
Pulmonary function tests, including forced expiratory volume at 1 second (FEV1), forced vital capacity (FVC), FEV1/FVC ratio, and diffusing capacity (DLCO) were performed. Simple posterior–anterior chest radiography, paranasal sinus radiography, and CT of the chest were carried out. Radiographic findings on CT scans were evaluated with regard to the presence of cavitations, nodule, and bronchiectasis. The anatomical distributions were also analyzed. Lesions were classified as showing either upper lobe cavitary disease or nodular bronchiectatic disease by radiographic type. When the disease did not belong to either the upper lobe cavitary form or the nodular bronchiectatic form, it was categorized as unclassifiable. The extent of bronchiectasis was scored in each of the six lobes (right upper lobe, right middle lobe, right lower lobe, upper division of the left upper lobe, lingular division of the left upper lobe, left lower lobe) according to the proportion of lung involvement. Extent scores ranged from 0 to 18; 0 if < 25%, 1 if 25–49%, 2 if 50–74%, 3 if ≥ 75% [10]. Scoliosis was determined from the posterior–anterior chest radiograph. Pectus excavatum was determined from CT scans of the chest using the Haller index and defined as a Haller index greater than 3.5 [11].
Questionnaires
All participants were asked to complete the St. George’s respiratory questionnaire and Hospital Anxiety and Depression Scale (HADS) questionnaire. The HADS is a 14 item questionnaire measuring levels of anxiety (HADS-A, seven items) and depression (HADS-D, seven items). Each item is scored from 0–3; a cut-off point of 8 out of 21 is suggested for both the anxiety and depression sections [12].
Analysis
Baseline characteristics were summarized using descriptive statistics such as proportion, median, and interquartile range. Student’s t-tests and Mann–Whitney U-tests were used for comparison of continuous variables. Categorical variables were compared using chi-square or Fisher’s exact tests, as appropriate. A P-value of ≤ 0.05 was considered to indicate statistical significance. All statistical analyses were performed using SPSS 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics
A total of 127 patients with NTM lung disease were enrolled in the study, with eight patients withdrawing consent prior to study completion. Among them, 84 patients with nodular BE type NTM lung disease were included in the study. In addition, 50 patients with non-NTM BE were initially enrolled in the study; three patients withdrew consent. The median ages were 67 and 64 years for NTM lung disease and non-NTM BE groups, respectively (P = 0.16). Of the patients with NTM lung disease, 54 (64.3%) were female, compared with 29 (61.7%) in the non-NTM BE group. Among comorbidities, cancer was more common among the NTM lung disease group (21.4% vs. 6.4%, P = 0.03) (Table 1). Weight loss was more common among the NTM lung disease group although it failed to reach the conventional P-value of 0.05. (15.5% vs. 4.3%, P = 0.08) (Table 1).
Microbiology analysis of patient sputum
Of the 84 patients with NTM lung disease, 47 (60.0%) were infected with species belonging to the Mycobacterium avium complex; 11 (13.1%) were infected with M. abscessus complex species. Multiple NTM species were isolated in 20 (23.8%) patients (Table 2). Bacterial colonization by non-mycobacterial species was observed in 17 (20.2%) and 12 (25.5%) of NTM lung disease and non-NTM BE patients, respectively (P = 1.00). The trend that P. aeruginosa was more commonly isolated from non-NTM BE patients (5 patients, 10.6%) than NTM patients (2 patients, 2.4%) was observed (P = 0.10) (Table 3).
Phenotypic characteristics of the participants
No difference in height was observed between NTM lung disease and non-NTM BE patients (160.0 vs. 159.0 cm, P = 0.23). However, patients with NTM lung disease were of lower body weight than those with non-NTM BE (54.0 vs. 55.5 kg, P = 0.04); consequently, the body mass index (BMI) of NTM lung disease patients was also lower than that of non-NTM BE patients (BMI = 20.8 vs. 22.2 kg/m2, P < 0.001). Scoliosis was more common among patients with NTM lung disease than those with non-NTM BE (23.8% vs. 8.5%, P = 0.04) (Table 4).
Immunologic parameters of participants
Positive rheumatoid factor was detected more frequently in patients with non-NTM BE than with NTM lung disease (23.4% vs. 6.0%, P = 0.01); however, differences in mean rheumatoid factor levels were not statistically significant. No differences were seen regarding the presence of FANA, nor in FANA titers. Serum immunoglobulin levels were also similar between the two groups. Likewise, the proportion of IGRA-positive patients were similar in NTM lung disease patients and non-NTM BE patients (45.2 vs. 55.3%, P = 0.28) (Table 5).
Radiological characteristics
The extent of BE was greater in the non-NTM BE group than in nodular bronchiectatic NTM lung disease patients (4 vs. 3 points, P = 0.001). Tubular BE was most common in both groups (Table 6).
Pulmonary function
No differences in FVC were observed between NTM lung disease patients and non-NTM BE patients in terms of either absolute volume (2.8 vs. 2.7 L, P = 0.13) although percentage of predicted volume were smaller among non-NTM BE patients (94% vs. 87%, P = 0.02). Both absolute volume of FEV1 (2.1 vs. 1.8 L, P = 0.001) and percentage of predicted volume (101% vs. 86%, P = 0.001) were smaller among non-NTM BE patients. However, the proportion of patients who met criteria for chronic obstructive pulmonary disease was not different between two groups (13.6% vs. 23.9%, P = 0.15) (Table 7).
Quality of life and emotional status
Median St. George’s respiratory questionnaire scores were similar between the two groups (19.5 vs.18.1, P = 0.34). Twenty patients (23.8%) with NTM lung disease and 10 patients (21.3%) with non-NTM BE reported anxiety (P = 0.83). Twenty-three 23 patients (27.4%) with NTM lung disease and 10 patients (21.3%) with non-NTM BE reported symptoms of depression (P = 0.53).
Discussion
Through this prospective study, we collected phenotypic, immunologic, and other clinical data from patients with nodular BE type NTM lung disease and compared them with those of BE patients. These data confirmed several known characteristics of patients with NTM lung disease in the Korean population.
The phenotypic characteristics of patients with NTM lung disease in this study were similar to those described in previous reports [3, 4, 13, 14]. Patients with NTM lung disease were leaner than non-NTM BE patients in our study. Although the underlying mechanism for the association between NTM lung disease and low BMI is not well understood, decreased leptin and increased adiponectin, and/or decreased estrogen in older women with low BMI may account for the increased susceptibility of these individuals to NTM infections [3]. In addition to low BMI, scoliosis and pectus excavatum are also frequently observed among NTM lung disease; a higher rate of scoliosis in patients with NTM lung disease was also seen in our study. These skeletal abnormalities may be indicative of an underlying genetic predisposition, though a precise mechanism linking the two has not been proposed [15].
M. avium complex and M. abscessus were the most common organisms isolated, consistent with a previous report on Korean patients with NTM lung disease [16]. Frequent isolation of M. abscessus is one of the characteristics of Korean patients that differ from patients from other countries [4]. Mixed infection by two or more NTM species was observed in 23.8% (20/84) of our patients; this observation confirmed our previous retrospective study showing high rates of mixed NTM infections [17]. Further examination will be necessary to determine the clinical significance of these mixed NTM infections.
We assessed several immunological markers, including FANA, rheumatoid factor, and serum immunoglobulins, and compared them with those of BE patients. Although most immunological markers were similar between the NTM lung disease and non-NTM BE groups, rheumatoid factor was found more commonly in patients with non-NTM BE. Given that the prevalence of rheumatoid arthritis and FANA were similar in both groups, the higher frequency of rheumatoid factor among patients with BE may be interpreted as a false positive. Various clinical settings have been shown to cause false positive results for rheumatoid factor [18].
NTM lung disease patients in our cohort were less likely to harbor P. aeruginosa than BE patients. Previous studies have also reported lower incidence of P. aeruginosa in BE or cystic fibrosis patients with NTM colonization. The underlying mechanism driving this phenomenon is not yet understood, but the observation that decontamination of P. aeruginosa yielded the cultivation of NTM colonization suggests a level of antagonism between P. aeruginosa and NTM [8, 19]–[22].
A considerable number of NTM lung disease and non-NTM BE patients in our study reported feelings of anxiety (23.8% and 21.3%, respectively) as well as depression (27.4% and 21.3%, respectively). Given that the lifetime prevalence of depression and anxiety disorders in South Korea are 5.6% and 6.9%, respectively [23], rates reported here appear significantly higher than those in the general population. A similar study conducted in the United States showed that 20% of BE patients had elevated depression-related scores and 38% had elevated anxiety-related scores [24]. Consistently higher rates of depression and anxiety among NTM lung disease patients and non-NTM BE patients may stem from increased respiratory symptoms as well as other comorbidities.
Conclusions
In conclusion, the characteristics of Korean NTM lung disease patients in this study were similar to those of patients in other countries. The fact that some phenotypic and clinical characteristics of NTM lung disease patients were different from those of non-NTM BE patients suggests differences in the immunopathogenesis of NTM lung disease and non-NTM BE.
References
Martin-Casabona N, Bahrmand AR, Bennedsen J, Thomsen VO, Curcio M, Fauville-Dufaux M, Feldman K, Havelkova M, Katila ML, Koksalan K, Pereira MF, Rodrigues F, Pfyffer GE, Portaels F, Urgell JR, Rusch-Gerdes S, Tortoli E, Vincent V, Watt B, Spanish Group for Non-Tuberculosis M: Non-tuberculous mycobacteria: patterns of isolation: a multi-country retrospective survey. Int J Tuberc Lung Dis. 2004, 8: 1186-1193.
Yim JJ, Kim HJ, Kwon OJ, Koh WJ: Association between microsatellite polymorphisms in intron II of the human Toll-like receptor 2 gene and nontuberculous mycobacterial lung disease in a Korean population. Hum Immunol. 2008, 69: 572-576.
Kartalija M, Ovrutsky AR, Bryan CL, Pott GB, Fantuzzi G, Thomas J, Strand MJ, Bai X, Ramamoorthy P, Rothman MS, Nagabhushanam V, McDermott M, Levin AR, Frazer-Abel A, Giclas PC, Korner J, Iseman MD, Shapiro L, Chan ED: Patients with nontuberculous mycobacterial lung disease exhibit unique body and immune phenotypes. Am J Respir Crit Care Med. 2013, 187: 197-205.
Kim RD, Greenberg DE, Ehrmantraut ME, Guide SV, Ding L, Shea Y, Brown MR, Chernick M, Steagall WK, Glasgow CG, Lin J, Jolley C, Sorbara L, Raffeld M, Hill S, Avila N, Sachdev V, Barnhart LA, Anderson VL, Claypool R, Hilligoss DM, Garofalo M, Fitzgerald A, Anaya-O'Brien S, Darnell D, DeCastro R, Menning HM, Ricklefs SM, Porcella SF, Olivier KN, et al: Pulmonary nontuberculous mycobacterial disease: prospective study of a distinct preexisting syndrome. Am J Respir Crit Care Med. 2008, 178: 1066-1074.
Park YS, Lee CH, Lee SM, Yang SC, Yoo CG, Kim YW, Han SK, Shim YS, Yim JJ: Rapid increase of non-tuberculous mycobacterial lung diseases at a tertiary referral hospital in South Korea. Int J Tuberc Lung Dis. 2010, 14: 1069-1071.
Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, Holland SM, Horsburgh R, Huitt G, Iademarco MF, Iseman M, Olivier K, Ruoss S, Von Reyn CF, Wallace RJ, Winthrop K, Subcommittee ATSMD, American Thoracic S, Infectious Disease Society of A: An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007, 175: 367-416.
Barker AF: Bronchiectasis. N Engl J Med. 2002, 346: 1383-1393.
Sethi S, Evans N, Grant BJ, Murphy TF: New strains of bacteria and exacerbations of chronic obstructive pulmonary disease. N Engl J Med. 2002, 347: 465-471.
Clinical and Laboratory Standards Institute: Interpretive criteria for microorganism identification by DNA target sequencing; approved guideline. CLSI document MM18-A. 2008, Wayne, PA: Clinical and Laboratory Standard Institute
Smith IE, Jurriaans E, Diederich S, Ali N, Shneerson JM, Flower CD: Chronic sputum production: correlations between clinical features and findings on high resolution computed tomographic scanning of the chest. Thorax. 1996, 51: 914-918.
Haller JA, Kramer SS, Lietman SA: Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report. J Pediatr Surg. 1987, 22: 904-906.
Bjelland I, Dahl AA, Haug TT, Neckelmann D: The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002, 52: 69-77.
Okumura M, Iwai K, Ogata H, Ueyama M, Kubota M, Aoki M, Kokuto H, Tadokoro E, Uchiyama T, Saotome M, Yoshiyama T, Yoshimori K, Yoshida N, Azuma A, Kudoh S: Clinical factors on cavitary and nodular bronchiectatic types in pulmonary Mycobacterium avium complex disease. Intern Med. 2008, 47: 1465-1472.
Griffith DE: Nontuberculous mycobacterial lung disease. Curr Opin Infect Dis. 2010, 23: 185-190.
Chan ED, Iseman MD: Underlying host risk factors for nontuberculous mycobacterial lung disease. Semin Respir Crit Care Med. 2013, 34: 110-123.
Koh WJ, Kwon OJ, Lee KS: Diagnosis and treatment of nontuberculous mycobacterial pulmonary diseases: a Korean perspective. J Korean Med Sci. 2005, 20: 913-925.
Lim HJ, Park CM, Park YS, Lee J, Lee SM, Yang SC, Yoo CG, Kim YW, Han SK, Yim JJ: Isolation of multiple nontuberculous mycobacteria species in the same patients. Int J Infect Dis. 2011, 15: e795-e798.
Elkayam O, Segal R, Lidgi M, Caspi D: Positive anti-cyclic citrullinated proteins and rheumatoid factor during active lung tuberculosis. Ann Rheum Dis. 2006, 65: 1110-1112.
Bange FC, Kirschner P, Bottger EC: Recovery of mycobacteria from patients with cystic fibrosis. J Clin Microbiol. 1999, 37: 3761-3763.
Fowler SJ, French J, Screaton NJ, Foweraker J, Condliffe A, Haworth CS, Exley AR, Bilton D: Nontuberculous mycobacteria in bronchiectasis: prevalence and patient characteristics. Eur Respir J. 2006, 28: 1204-1210.
Hayes D: Mycobacterium abscessus and other nontuberculous mycobacteria: evolving respiratory pathogens in cystic fibrosis: a case report and review. South Med J. 2005, 98: 657-661.
Wickremasinghe M, Ozerovitch LJ, Davies G, Wodehouse T, Chadwick MV, Abdallah S, Shah P, Wilson R: Non-tuberculous mycobacteria in patients with bronchiectasis. Thorax. 2005, 60: 1045-1051.
Cho MJ, Chang SM, Hahm BJ, Chung IW, Bae A, Lee YM, Ahn JH, Won S, Son J, Hong JP, Bae JN, Lee DW, Cho SJ, Park JI, Lee JY, Kim JY, Jeon HJ, Lee HW: Lifetime risk and age of onset distributions of psychiatric disorders: analysis of national sample survey in South Korea. Soc Psychiatry Psychiatr Epidemiol. 2012, 47: 671-681.
Olveira C, Olveira G, Gaspar I, Dorado A, Cruz I, Soriguer F, Quittner AL, Espildora F: Depression and anxiety symptoms in bronchiectasis: associations with health-related quality of life. Qual Life Res. 2013, 22: 597-605.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2334/13/558/prepub
Acknowledgements
This work was supported by Grant No. 04-2011-0670 from the Seoul National University College of Medicine Research Fund (Seoul, Republic of Korea).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
Study concept and design: JJY. Acquisition of data: ARL, MWS, SAK, MK, KOC. Analysis and interpretation of data: ARL, JL, SMC, JJY. Drafting of the manuscript: ARL. Critical revision of the manuscript for important intellectual content: ARL, JL, SMC, MOS, JJY. Statistical analysis: ARL, JJY. Study supervision: JJY. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Lee, AR., Lee, J., Choi, SM. et al. Phenotypic, immunologic, and clinical characteristics of patients with nontuberculous mycobacterial lung disease in Korea. BMC Infect Dis 13, 558 (2013). https://doi.org/10.1186/1471-2334-13-558
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2334-13-558