
Abstract
Background
Data on the epidemiology and costs related to herpes zoster (HZ) and postherpetic neuralgia (PHN) in Spain are scarce; therefore, studies are needed to evaluate the epidemiological and economic impact of HZ and its most common complication, PHN. The present study aimed to estimate the clinical and economic burden of HZ and PHN in Valencia (Spain).
Methods
We prospectively analyzed the burden of HZ and PHN and their attributable costs in patients from 25 general practices in the Autonomous Community of Valencia serving 36,030 persons aged > 14 years. All patients with a clinical diagnosis of HZ who attended these centers between December 1st 2006 and November 30th 2007 were asked to participate. Patients included were followed for 1 year.
Results
Of the 130 cases of HZ followed up, continued pain was experienced by 47.6% (95% confidence interval (CI) = 35.6-56.7%) at 1 month after rash onset, by 14.5% (95% CI = 7.8-1.2%) at 3 months, by 9.0% (95% CI = 3.7-14.3%) at 6 months, and by 5.9% (95% CI = 1.5-10.3%) at 12 months. The percentage of patients with PHN increased with age, from 21.4% (95% CI = 8.3-40) in patients < 50 years to 59.2% (95% CI = 44.4-74) in patients ≥ 70 years. The estimated total cost for the 130 HZ cases during the follow-up period was €49,160 ($67,349). Mean cost per patient was €378 (range 53-2,830) ($517, range 73-3,877).
Conclusions
This study shows that PHN is a relatively common complication of HZ and that both conditions combined give rise to a significant clinical and economic burden for patients and providers.
Similar content being viewed by others

Background
Herpes zoster (HZ) is caused by the reactivation of a latent infection with varicella zoster virus (VZV) after primary chickenpox. HZ is characterized by a localized eruption of vesicular lesions following the trajectory of a sensory nerve, and by the presence of pain and inflammation of the affected nerve root [1].
The most frequent and debilitating complication of HZ is postherpetic neuralgia (PHN), defined as neuropathic pain that appears in the dermatomes affected by the VZV infection. Pain associated with PHN can be very severe and disabling and has a significant impact on a patient's quality of life [2].
Studies carried out in a number of countries have shown that the incidence and severity of both HZ and PHN increase significantly with age. The annual incidence of HZ reported in population-based studies from several countries ranged from 1.2 to 4.8 cases per 1,000 inhabitants/year. The lifetime risk of HZ can be as high as 30% and increases markedly with age, affecting 50% of people living to 85 years of age [3–11]. PHN affects 10-70% of patients with HZ. This wide range is partly due to differences in the definition of PHN used in different studies and to the age range of the study populations from which these estimates were obtained. Thus, in older patients, the prevalence of PHN among patients with HZ is likely to be closer to the upper boundary of that range [12].
In a previous study we reported an annual incidence of HZ of 4.1 per 1,000 persons > 14 years of age (95% confidence interval (CI) = 3.4-4.7) and described the clinical and epidemiological characteristics of HZ in Spain [13]. Our results were consistent with previous findings by other authors in Spain [14, 15], and in other European [16–25] and non-European [8, 10, 11, 26–28] published studies.
Data on the epidemiology of HZ and PHN in Spain, and on the associated costs are scarce; therefore, studies are needed to evaluate the epidemiological and economic impact of HZ and its most common complication, PHN. The present study aimed to estimate the clinical and economic burden of HZ and PHN in the primary health care system in Spain.
Methods
Design and setting
During a 1-year period (from 1st December 2006 to 30th November 2007), a prospective study was carried out in 25 primary care general practitioner (GP) offices of the public healthcare system of the Autonomous Community of Valencia, Spain. We selected a convenience sample of 25 GP offices from rural (n = 6), urban (n = 10) and semiurban (n = 9) areas that were considered to be representative of this Autonomous Community.
Study population
During the study period, all patients > 14 years of age who attended the investigators' offices and were clinically diagnosed with HZ were considered to be eligible for inclusion. All patients who agreed to participate in the study signed an informed consent form prior to their participation.
For each patient, information was collected on demographic attributes, personal clinical history, clinical characteristics of the HZ episode and associated complications, medical visits and medication used to treat the episode or its complications, and work absenteeism of the patients or their carers. The information was obtained by interview with the patient and by review of their medical records. No further medical visits were planned for study purposes. Patients were telephoned the day after the diagnosis, and four times during follow-up (at 1, 3, 6 and 12 months after diagnosis). If the patients reported pain, they were contacted monthly until disappearance of the pain. In those cases where patients could not be accessed by phone, they were visited at home by the study investigators in order to establish their clinical status.
One hundred and forty six patients were diagnosed and invited to participate. Those who declined to participate (n = 16; 10.9%) were anonymously counted as HZ cases to allow a real estimate of the incidence of the disease. Of the 130 participants, 1-year complete data was obtained in 118 patients (90.8%). Thus, we had incomplete follow-up data for 12 patients (9.2%): six died because of factors unrelated to HZ, two withdrew voluntarily from the study and four patients were lost to follow-up.
Study measures and definitions
For the purpose of the present study we considered a case of HZ as a localized eruption of vesicular lesions following the trajectory of a sensory nerve as well as pain and inflammation of the affected nerve root. This definition was purely clinical since no other confirmatory test was necessary. A diagnostic test was performed only if the GP determined that it was necessary.
We defined PHN as the presence of any pain, without specifying a numerical threshold of intensity. We believe that this definition is in accordance with most publications in this setting [27, 29–32]. PHN is defined as pain that persists beyond the acute phase of an HZ episode. For this study, we considered PHN1, PHN3, PHN6 and PHN12 as pain persisting 1, 3, 6 or 12 month(s), respectively, after the onset of the rash. We defined "recurrence" as the development of cutaneous lesions on the site of a previous eruption or at a different site, which occurred beyond 3 months after the index HZ episode was diagnosed. Recurrent HZ was not counted as a new case.
Direct costs were evaluated as those derived from medical care and medications, and included: 1) the number of medical visits: primary care visits, primary care emergency consultations, specialist visits, other professional visits, hospitalizations, hospital emergencies; 2) medications prescribed and/or consumed; and 3) diagnostic tests. We included the costs arising from symptoms occurring in the time period preceding the vesicular rash, and all patients were asked, as per protocol, about these outpatient or hospital visits during the initial interview.
The unit costs for the medical care variables were obtained from the Valencian Community Official Registries (Presupuestos del Ejercicio 2008 de la Generalitat Valenciana) [33] and the cost of medications was obtained from the Vademecum® 2007 Edition as a reference for each medication price [34]. Indirect costs were defined as the productivity losses of patients and/or their carers, which were calculated from the number of hours of work missed related to HZ. The cost for an effective working hour in 2007 was obtained from the Spanish National Institute of Statistics [35]. For the present analysis we also took into consideration whether patients were active workers (for which 60% of the cost of medications is reimbursed by Spanish Social Security) or pensioners (for which 100% is reimbursed) [36]. All costs are presented in 2007 Euros (€).
The study was approved by the Clinical Research Ethics Committee of the Dirección General de Salud Pública/Centro Superior de Investigación en Salud Pública (CSISP) de la Comunidad Valenciana.
Sample size calculation: Statistical analysis
Based on an expected incidence of HZ in the adult population of 0.4% and a precision of 0.08%, we calculated that a minimum population of 23,600 people > 14 years of age should be monitored [6]. The study population assigned to the 25 participating investigators represented a total of 36,030 individuals. This population comprised 21,500 patients aged 15-49 years, 4,893 patients aged 50-59 years, 4,057 patients aged 60-69 years, and 5,580 patients aged ≥ 70 years. The age and gender distribution of patients recruited in our study was similar to that observed in the general population (based on data from national Spanish registries [37]).
The percentage of patients with persisting pain during follow-up was analyzed using the Kaplan-Meier method. The incidence was calculated globally by gender and by predefined age groups (< 50 years, 50-59 years, 60-69 years, and ≥ 70 years of age). Comparisons between groups were performed using Student's t-test for continuous variables with Gaussian distribution.
Logistic regression was used to identify predictors of the occurrence of PHN at 1 and 3 months (dependent variable). We considered as covariates those variables that showed a P-value of ≤ 0.25 in the univariable analysis (presence of PHN versus no PHN) and those clinically relevant in previous studies (age, gender, prodromal pain, extremities localization, sacrum localization, time from symptoms onset until diagnosis, and time from rash onset until diagnosis). We used an "enter" variable selection method. We obtained the odds ratio (OR) and 95% CI. Model calibration was tested with the Hosmer-Lemeshow test. Model discrimination was evaluated with the analysis of the area under the ROC (Receiver Operating Characteristic) curve. All P-values < 0.05 were considered to be statistically significant. All statistical analyses were performed using the SPSS software package, version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Epidemiology of PHN
Baseline characteristics of study patients are presented in Table 1. A total of 146 HZ patients were diagnosed within the 1-year period, an annual incidence of 4.1 cases per 1,000 persons > 14 years (95 CI % = 3.4-4.7). Median age was 63.5 years (range 19-94; interquartile range 51-75 years) and the highest incidence was observed in older patients (≥ 70 years of age), namely 11.1/1,000 population.
In the present study, only one case (1/130) of recurrence at the same site was reported at 7 months. No recurrences (0/130) at different sites were observed. Pain continued to be experienced by 47.6% of patients at 1 month after rash onset (95% CI = 35.6-56.7%), by 14.5% (95% CI = 7.8-21.2%), at 3 months, by 9.0% (95% CI = 3.7-14.3%) at 6 months, and by 5.9% (95% CI = 1.5-10.3%) at 12 months (Figure 1). The median duration of pain was 26.5 days (95% CI = 20-34). Figure 2 shows the percentage of patients with PHN at 1 month and 3 months in each age group. The mean age of patients who fulfilled the PHN definition at 1 month was 66.7 years, and 61.7% of the patients were female. In the case of PHN at 3 months, the mean age was 70.1 years, and 50% of the patients with PHN were female. The percentage of patients developing PHN (at 1 month) increased with age from 21.4% (95% CI = 8.3-40) in patients < 50 years to 59.2% (95% CI = 44.4-74) in patients ≥ 70 years (Figure 2).

Kaplan-Meier method showing the percentage of patients with persisting pain during the follow-up.

Percentage of patients developing postherpetic neuralgia (PHN) at 1 and 3 months per age groups (95% confidence intervals are presented).
In the multivariate model, age (years) (OR = 1.04, P < 0.01) and time interval (days) between symptom onset and clinical diagnosis (OR = 1.11, P < 0.01) were both independently associated with PHN at 1 month. At 3 months, only age (OR = 1.04, P = 0.03) was found to be associated with PHN. However, we did not observe a significant association of gender or antiviral drug use (both P > 0.05) with the occurrence of PHN.
Health care and medication costs of HZ disease
During the follow-up period, 130 cases of HZ generated a total of 308 primary care visits (mean per patient = 2.37; standard deviation (SD) = 1.99), 86 visits to the Emergency Room in Primary Care Centers (mean per patient = 0.66; SD = 1.04), 38 Specialist visits (mean per patient = 0.29; SD = 1.08), 40 other professional (nurse, physiotherapist and alternative medical practitioner) visits (mean per patient = 0.31; SD = 2.82), 23 hospital Emergency Room visits (for first medical contact for the diagnosis of HZ before being attending the GP office, and for episodes of severe pain) (mean per patient = 0.18; SD = 0.52), and 29 diagnostic tests (including X-ray studies (thorax and abdomen), blood and urine tests, electrocardiograms and ultrasound scans in patients with pain but no cutaneous manifestations, before the HZ rash appeared) (mean per patient = 0.22; SD = 0.64). No confirmation molecular tests were performed. No hospitalizations for HZ disease were observed during the study follow-up.
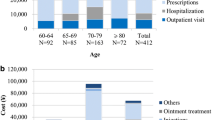
The total cost for the management of the 130 patients included in the analysis during the 1-year follow-up period was €40,234 (US$55,120) for a Third-Party Payer (TPP) perspective (Spanish Social Security), and €49,160 ($67,349) from a societal perspective, yielding an average cost per patient of €309, SD = 308 ($423, SD = 422) and €378, SD = 431 ($518, SD = 590), respectively. The most important factor that contributed to the economic burden of disease (Table 2) was medication (33% and 37% of the cost from the TPP perspective and the societal perspective, respectively) followed by GP visits (29% and 23% of the cost from the TPP perspective and the societal perspective, respectively), and Emergency in Primary Care visits (18% and 15% of the cost from the National Payer perspective and the societal perspective, respectively) (Table 2).
Ninety-one percent of patients were prescribed antivirals, representing 77% of the total cost of medication. Other medications used were anticonvulsants (12.2%), analgesics (4.7%), antidepressants (0.6%), opioids (0.5%) and corticoids (0.4%), accounting all together for 18.4% of the total costs of medications. Total and mean costs per age groups are summarized in Table 3.
Our study patients lost a total of 565 hours of work (mean per patient = 4.35; SD = 25.99) and their carers lost 6 hours of work (mean per patient = 0.05; SD = 0.53).
Cost of PHN1
Total cost of the management of patients with PHN1 was significantly (P < 0.001) higher (total cost, €32,974 ($45,110); mean per patient, €549 ($752), SD = €580 ($795)) compared with the cost for patients without PHN (total costs, €16,186 ($22,175)); mean per patient, €231 ($316); SD = €107 ($147)). The most important factor that contributed to the cost was medication (€10,923 ($14,964); mean per patient, €182 ($249), SD = €182 ($249) followed by GP visits (€6,686 ($9,160); mean per patient, €111 ($152), SD = €69 ($95)) and Emergency in Primary Care visits (€4,173 ($5,717); mean per patient, €70 ($96), SD = €111 ($152)) (Table 4).
Cost of PHN3
Total cost of management of patients with PHN3 was significantly higher (P < 0.001) (total costs, €14,786 ($20,257); mean per patient, €821 ($1,125), SD = €681 ($941)) compared with the cost for patients without PHN (total costs, €34,373 ($47,091); mean per patient, €307 ($421), SD = €328 ($449)). The most important factor that contributed to the cost was medication (€5,730 ($7,850); mean per patient, €318 ($436), SD = €280 ($384)) followed by Emergency in Primary Care visits (€2,421 ($3,317); mean per patient, €134 ($184), SD = €165 ($226)) and GP visits (€2,393 ($3,278); mean per patient, €133 ($182), SD = €91 ($125)) (Table 5). None of the study patients was treated by pain clinics during the one year follow-up. Table 6 presents detailed information regarding the consumption of resources by patients with PHN1 and PHN3.
Discussion
No previous study has provided current HZ epidemiological data and a detailed estimate of the associated costs in Spain. It is important to highlight that our study was prospectively designed and patients' symptoms were monitored periodically by phone until PHN resolution. As mentioned above, no medical visits were planned for study purposes in order to allow for a more accurate estimate of healthcare resource consumption associated with HZ management. Moreover, this is the first study in Spain that provides information about the cost of HZ and PHN on an outpatient basis. Others have reported the cost of HZ in patients admitted to hospital [38].
In our study the 1-year incidence of HZ was 4.1 per 1000 persons (95% CI = 3.4-4.7) in those aged > 14 years. The incidence of PHN was 47.6% at 1 month. This percentage was higher than the figures reported in retrospective studies in Europe (14.3% [all ages of subjects] [39] to 19.5% [≥ 50 years of age] [24]) but similar to that in a prospective study (51.2%) recently published in a Mediterranean country [40]. In the USA, a groundbreaking study by Yawn [27] reported that the incidence of HZ in subjects > 22 years in the US was 3.6 per 1000 person-years (95% CI = 3.4-3.7). The incidence of PHN in the same population was 82% when defined as pain of at least 1 month duration. In the case of 3-month PHN (PHN3), our results (14.5%) were similar to those reported in other observational studies in Europe [23, 24, 40], and also to those reported in the USA [4, 27].
Although differences were observed with regard to PHN1 between our study and that of Yawn [27], the incidence of HZ and PHN at 3 months was similar though determined in slightly different populations (> 22 vs. > 14 years). We do not have a reason for the 1-month difference as both study populations showed a similar distribution of age and gender, both of which have an effect on the incidence of PHN. Nevertheless, the different study designs might have an impact in this regard. The study by Yawn [27] was retrospective and the present investigation was prospective to better estimate the occurrence of PHN.
The main risk factor for developing PHN among immunocompetent subjects in our study was age. An increase in 1 year of age yielded a 4.2% increase in the risk of PHN at 1 and 3 months. This finding has been previously observed by other authors [23, 24].
There is controversy as to whether gender can be considered an actual risk factor for PHN as some studies found an association [24, 39] while others did not [23]. Differences between genders, regarding perception and response to pain, may explain the disparities [41], or a higher GP attendance by women may play a part.
In our study the overall percentage of patients treated with antivirals was high, namely 91%, when compared with the proportion of patients (58.8%) in whom treatment was initiated within 72 hours of the onset of rash (following the current treatment recommendations). However, this proportion was not substantially different to that observed in other previously published studies, such as the Oxman study [4]. In that study, the percentage of patients treated with antiviral drugs ranged from 85.7% to 87.3%. Differences in study design might have influenced the small differences between the studies.
In our study the prescription of antiviral therapy was not associated with the occurrence of PHN, although it should be stressed that a high percentage of patients (41.2%) received antivirals beyond 72 hours after rash onset. After adjusting for other co-variates, such as age and presence of chronic illness, it was not found that antivirals would act as a preventive measure for the development of PHN.
This study also provides a recent estimate of the economic burden of HZ and PHN in a developed country. Given that the size of Spanish population age > 14 years in 2007 was 38,443,352 inhabitants, and that the prevalence of HZ was 4.1 cases per 1,000 persons > 14 years (95% CI = 3.4-4.7), we estimate a national cost of €59.6 million per year (95% CI = 49.4-68.3), which represents 0.06‰ of the 2007 gross national product (GNP).
In comparing with other European studies, our investigation found the cost of HZ to be €378 per patient, roughly double the cost reported by Gautier [24] (103 GB Pounds [£] equivalent to €151), but was lower than those reported by Davies [42] (£770, equivalent to €1132), Edmunds [43] (£306 equivalent to €450) and Scott [23] (£524, equivalent to €770). The high cost reported by Davies [42] could be due to the fact that the patients attended a tertiary referral center with a specialist pain clinic. We report a cost per PHN episode of 549 € using the 1-month definition, similar to that reported by Gautier [24] (£341, equivalent to €501). Applying the 3-month PHN definition, we report a total cost equal to €821 per patient while it was of £397 (€584) in Gautier's study [24].
In the USA, the comparable study by Yawn [44] found that the mean HZ-attributable cost was $782 (€531) for those patients in an outpatient setting. In our study (no hospitalizations were recorded) the mean cost was €378, significantly lower than that reported in the Yawn study [44]. For those patients who developed PHN, a mean cost of $4,388 per patient (€3203) was obtained in the Yawn study [44]. Again, this figure was substantially higher than our estimate (€821). Noteworthy in the Yawn's study there were 66 HZ-related hospitalizations, (with a mean length of stay of 5.1 days) compared to none hospitalizations in our study. This could explain, at least partially, the observed differences.
Comparisons between different studies from different countries are controversial due to substantial disparities in economic, demographic, cultural and institutional (health sector) structures [45]. Moreover, the different rate of antiviral prescribing (50% in the Gautier [24] study vs. 91% in the present study) might have accounted for some of the differences in the total cost between the studies. This issue is in contrast with the current recommendations of clinical consensus reports and needs to be studied in detail separately [46].
In line with Gautier's study in Europe [24] and Yawn's study in the USA [44], the most important factor that contributed to the economic burden was medication, followed by general practitioner visits.
HZ and PHN have an important impact for the Spanish Health Service, society and the individual. Current therapies and options do not completely alleviate the acute pain, and fail to prevent PHN, and thus provides preventive measures such as vaccination may be warranted. Zoster vaccine has been shown to reduce the burden of HZ by decreasing the incidence and symptom severity, and it has also been shown to reduce the incidence of PHN compared with placebo [4].
Our study has some limitations. First, those patients with HZ who may have gone to a private practitioner might not be detected in our study, leading to an underestimate of the disease; however, it can be presumed that this proportion of patients would be small given the free health care provision in Spain and the reimbursement of drugs prescribed in public GP offices. In Spain many patients directly attend Accident & Emergency (A&E) departments when they perceive a disease as "serious". This might have underestimated our incidence result. Any way, we consider that this underestimation should not be of considerable importance as in the Valencian Community, usually patients diagnosed by the A&E departments physicians or private specialists, in addition, attend to their primary care GP for prescription and reimbursement of medication, thus being susceptible to be recruited in the study.
Second, our study is not a population-based study but is based on a convenience sample of primary healthcare GP offices, so extrapolation of our results to the general adult population should be made with caution. Finally, in our study the costs related to working time lost showed a wide range of variation as indicated by a high standard deviation, thus making interpretation difficult.
Conclusions
HZ and PHN are prevalent diseases in Spain whose incidence increases with age. HZ and PHN have a significant clinical and economic burden. Randomized controlled trials would be appropriate and necessary to investigate the role of antiviral therapy in preventing PHN when prescribed more than 72 hours after rash onset.
Abbreviations
- HZ:
-
herpes zoster
- VZV:
-
varicella zoster virus
- PHN:
-
postherpetic neuralgia
- CI:
-
confidence interval
- GP:
-
general practitioner PHN1: PHN at 1 month
- PHN3:
-
PHN at 3 months
- PHN6:
-
PHN at 6 months
- PHN12:
-
PHN at 12 months
- €:
-
euros
- $:
-
US dollars
- OR:
-
odds ratio
- SD:
-
standard deviation
- TPP:
-
Third-Party Payer
- £:
-
GB pounds
- GPN:
-
gross national product
- A&E:
-
Accident and emergency departments.
References
Thomas SL, Wheeler JG, Hall AJ: Contacts with varicella or with children and protection against herpes zoster in adults: a case-control study. Lancet. 2002, 360: 678-682.
Ly Pen D, Manzano Espinosa L: Neuralgia postherpética: incidencia, prevención y tratamiento. Rev Clin Esp. 2007, 207: 23-28.
Schmader K: Herpes zoster in older adults. Clin Infect Dis. 2001, 32: 1481-1486.
Oxman MN, Levin MJ, Johnson GR, Schmader KE, Straus SE, Gelb LD, Arbeit RD, Simberkoff MS, Gershon AA, Davis LE, Weinberg A, Boardmand KD, Williams HM, Hongyuan Zhang J, Peduzzi PN, Beisel CE, Morrison VA, Guatelli JC, Brooks PA, Kauffman CA, Pachucki CT, Neuzil KM, Betts RF, Wright PF, Griffin MR, Brunell P, Soto NE, Marques AR, Keay SK, Goodman RP, for the Shingles Prevention Study Group, et al: A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med. 2005, 352: 2271-2284.
Brisson M, Edmunds WJ, Gay NJ, Law B, De Serres G: Modelling the impact of immunization on the epidemiology of varicella zoster virus. Epidemiol Infect. 2002, 125: 651-669.
Thomas SL, Hall AJ: What does epidemiology tell us about risk factors for herpes zoster?. Lancet Infect Dis. 2004, 4: 26-33.
Hope-Simpson RE: The nature of Herpes Zoster: a long-term study and a new hypothesis. Proc R Soc Med. 1965, 58: 9-20.
Yih WK, Brooks DR, Lett SM, Jumaan AO, Zhang Z, Clements KM, Seward JF: The incidence of varicella and herpes zoster in Massachusetts as measured by the Behavioral Risk Factor Surveillance System (BRFSS) during a period of increasing varicella vaccine coverage, 1998-2003. BMC Public Health. 2005, 5: 68-77.
De Melker H, Berbers G, Hahné S, Rümke H, van den Hof, De Wit A, Boot H: The epidemiology of varicella and herpes zoster in The Netherlands: Implications for varicella zoster virus vaccination. Vaccine. 2006, 24: 3946-3952.
Jumaan AO, Yu O, Jackson LA, Bohlke K, Galil K, Seward JF: Incidence of herpes zoster, before and after varicella-vaccination-associated decreases in the incidence of varicella, 1992-2002. J Infect Dis. 2005, 19: 2002-2007.
Mullooly JP, Riedlinger K, Chun C, Weinmann S, Houston H: Incidence of herpes zoster, 1997-2002. Epidemiol Infect. 2005, 133: 245-253.
Oster G, Harding G, Dukes E, Edelsberg J, Cleary PD: Pain, medication use, and health-related quality of life in older persons with postherpetic neuralgia: results from a population-based survey. J Pain. 2005, 6: 356-363.
Cebrián-Cuenca AM, Díez-Domingo J, Rodríguez MS, Puig-Barberá J, Navarro-Pérez J: "Herpes Zoster Research Group of the Valencian Community". Epidemiology of herpes zoster infection among patients treated in primary care centres in the Valencian Community (Spain). BMC Fam Pract. 2010, 6: 11-33.
García Cenoz M, Castilla J, Montes Y, Morán J, Salaberri A, Elía F, Floristán Y, Rodrigo I, Irisarri F, Arriazu M, Zabala A, Barricarte A: Incidencia de la varicela y el herpes zoster antes de la introducción de la vacunación sistemática infantil en Navarra, 2005-2006. An Sist Sanit Navar. 2008, 31: 71-80.
Pérez-Farinós N, Ordobás M, García-Frenández C, García-Comas L, Cañellas S, Rodero I, Gutiérrez-Rodríguez A, García-Gutiérrez J, Ramírez R: Varicella and Herpes zoster in Madrid, based on the Sentinel General Practitioner Network: 1997-2004. BMC Infect Dis. 2007, 7: 59-64.
McGregor RM: Herpes zoster, chicken-pox, and cancer in general practice. BMJ. 1957, 1: 84-87.
Fleming DM, Norbury CA, Crombie DL: Annual and seasonal variation in the incidence of common diseases. 1991, Birmingham: Royal College of General Practitioners
McCormick A, Fleming D, Charlton J: Morbidity statistics from general practice: 4th national study 1991-92. A study carried out by the Royal College of General Practitioners, the Office of Population Censuses and Surveys, and the Department of Health. 1995, London: HM Stationery Office
Chidiac Ch, Bruxelle J, Daures JP, Hoang Xuan T, Morel P, Leplège A, El Hasnaoui A, de Labareyre C: Characteristics of patients with herpes zoster on presentation to practitioners in France. Clin Infect Dis. 2001, 33: 62-69.
Di Luzzio Paparati U, Arpinelli F, Viscona G: Herpes zoster and its complications in Italy: an observational survey. J Infection. 1999, 38: 116-119.
Opstelten W, Van Essen GA, Schellevis F, Verheij T, Moons K: Gender as independent risk factor for herpes zoster: a population based study. Ann Epidemiol. 2006, 16: 692-695.
Brisson M, Edmunds WJ: Epidemiology of varicella zoster virus in England and Wales. J Med Virol. 2003, 70: 9-14.
Scott FT, Johnson RW, Leedham-Green M, Davies E, Edmunds WJ, Breuer J: The burden of Herpes Zoster: A prospective population based study. Vaccine. 2006, 24: 1308-1314.
Gautier A, Breuer J, Carrington D, Martin M, Rèmy V: Epidemiology and cost of herpes zoster and post-herpetic neuralgia in the United Kingdom. Epidemiol Infect. 2009, 137: 38-47.
Czernichow S, Dupuy A, Flahault A, Chosidow O: Herpes zoster: incidence study among Sentinel practitioners. Ann Dermatol Venereol. 2001, 128: 497-501.
Richards P: Shingles in one family practice. Arch Fam Med. 1996, 5: 42-46.
Yawn BP, Saddier P, Wollan PC, St. Sauver JL, Kurland MJ, Sy L: A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction. Mayo Clin Proc. 2007, 82: 1341-1349.
Insinga R, Itzler RF, Pellissier JM, Saddier P, Nikas AA: The incidence of Herpes Zoster in a United States Administrative Database. J Gen Intern Med. 2005, 20: 748-753.
Watson CP, Watt VR, Chipman M, Birkett N, Evans RJ: The prognosis with postherpetic neuralgia. Pain. 1991, 46: 195-9.
Dworkin RH, Portenoy RK: Pain and its persistence in herpes zoster. Pain. 1996, 67: 241-51.
Helgason S, Petursson G, Gudmundsson S, Sigurdosson JA: Prevalence of postherpetic neuralgia after a single episode of herpes zoster: prospective study with long term follow up. BMJ. 2000, 321: 1-4.
Dworkin RH, Schmader KE: The epidemiology and natural history of herpes zoster and postherpetic neuralgia. Herpes zoster and postherpetic neuralgia, second revised and enlarged edition. Edited by: Watson CPN, Gershon AA. 2001, Amsterdam: Elsevier, 11: 39-64.
Ley 15/2007, de 27 de diciembre, de la Generalitat Valenciana, de Presupuestos para el ejercicio 2008 (DOCV 5670, de 31 de diciembre de 2007).
Vademécum Internacional: Medicom. Madrid. 2007, 48
Website of Spanish National Statistics Institute, Encuesta de Trimestre Laboral. [http://www.ine.es/jaxi/menu.do?type=pcaxis&path=/t22/p187&file=inebase&N=&L=]
Website of Conselleria de Sanitat de la Generalitat Valenciana. [http://www.san.gva.es/prof/dgf/farmacia/receta.html]
Website of Spanish National Statistics Institute. [http://www.ine.es/jaxi/tabla.do?path=/t20/e245/p04/a2007/l0/&file=00000003.px&type=pcaxis&L=0]
Gil A, Gil R, Alvaro A, San Martín M, González A: Burden of Herpes Zoster requiring hospitalization in Spain during a seven-year period (1998-2004). BMC Infect Dis. 2009, 9: 55-60.
Dieleman JP, Kerklaan J, Huygen FJ, Bouma PA, Sturkenboom MC: Incidence rates and treatment of neuropathic pain conditions in the general population. Pain. 2008, 137: 681-688.
Parrutti G, Tontodonati M, Rebuzzi C, Polilli E, Sozio F, Consorte A, Agostinone A, Di Masi F, Congedo G, D'Antonio D, Grnachelli C, D'Amario C, Carunchio C, Pippa L, Manzoli L, Volpi A, VZV Pain Study Group: Predictors of pain intensity and persistence in a prospective Italian cohort of patients with herpes zoster: relevance of smoking, trauma and antiviral therapy. BMC Medicine. 2010, 8: 58-68.
Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL: Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. 2009, 10: 447-485.
Davies L, Cossins l, Bowsher D, Drummond M: The cost of treatment for post-herpetic neuralgia in the UK. Pharmacoeconomics. 1994, 6: 142-148.
Edmunds J, Brisson M, Rose JD: The epidemiology of herpes zoster and potential cost-effectiveness of vaccination in England and Wales. Vaccine. 2001, 19: 3076-3090.
Yawn B, Itzler R, Wolan P, Pellissier J, Sy L, Saddier P: Health care utilization and cost burden of herpes zoster in a community population. Mayo Clin Proc. 2009, 84 (9): 787-94.
Schieber GJ, Poullier JP: International health care spending. Health Aff (Millwood). 1986, 5: 111-122.
Dworkin RH, Johnson RW, Breuer J, Gnann JW, Levin MJ, Backonja M, Betts RF, Gershon AA, Haanpaa ML, McKendrick MW, Nurmikko TJ, Oaklander AL, Oxman MN, Pavan-Langston D, Petersen KL, Rowbotham MC, Schmader KE, Stacey BR, Tyring SK, Wijck van AJ, Wallace MS, Wassilew SW, Whitley RJ: Recommendations for the management of herpes zoster. Clin Infect Dis. 2007, 44 (Suppl 1): S1-26.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2334/11/302/prepub
Acknowledgements
The authors would like to thank the members of the Herpes Zoster Research Group of the Valencian Community (Grupo de Herpes Zóster de la Comunidad Valenciana): Carlos Momparler-Martínez and José Manuel Navarrete-Villalta, Consultorio Auxiliar Chile (Valencia); Carlos García-García and José Francisco Guillem-Miralles, Centro de Salud de Nazaret (Valencia); Inmaculada Pereiró-Berenguer, Centro de Salud de Trafalgar (Valencia); Nidia Ruiz-Varea, Consultorio Auxiliar L'Alger (Valencia); Leonor Vives-Rebollar and Carmen Feliú-Morte, Centro de Salud de Serrería II (Valencia); Marta Álvarez-Martínez and Julia Cañada-Blasco, Centro de Salud de Guillem de Castro (Valencia); Elena Picón-García, José Antonio Pla-García, Ester Robles-Pastor and Francisca Cantos Fillols, Centro de Salud de Ayora (Valencia); Inmaculada Cervera-Pérez, Centro de Salud de Utiel (Valencia); Margarita Colomer-Paché, Antonio Roig López-De los Mozos and José Enrique Mir-Mora, Centro de Salud de Liria (Valencia); Marco Antonio Latorre-Atienza, Centro de Salud de Requena (Valencia); Daniel Matoses-Nácher, Centro de Salud de Almassera (Valencia); Lorenzo Pascual-López, Centro de Salud de Manises (Valencia); Roberto Gorgues-Comás, centro de salud de Ribarroja (Valencia); and Francisca Juan i Espert, Centro de Salud de Alaquás (Valencia).
We also would like to thank to Susana Iglesias and Mara Garcés for their support in following up the patients.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
Unrestricted grants from Conselleria de Sanitat of the Generalitat Valenciana reference number: A.P. 021/06 (Diari official de la Generalitat Valenciana (DOGV) number 5.373 from 24/October/2006) and Sanofi Pasteur MSD were used to support this research, but this financial support did not influence the analysis or interpretation of the data. JDD has received research funding from Sanofi Pasteur MSD and GlaxoSmithKline and also payments for attending advisory board meetings. JPB is principal investigator in clinical trials with GlaxoSmithKline vaccines. MSR is a staff member of Sanofi Pasteur MSD. The following authors declare that they have no competing interests: ACC and JNP.
Authors' contributions
ACC and JDD contributed to protocol preparation, patient recruitment, data collection, data analysis, results discussion and manuscript preparation. JPB and JNP contributed to results discussion and the critical revision of the manuscript. MSR contributed to data analysis and manuscript preparation. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Cebrián-Cuenca, A.M., Díez-Domingo, J., San-Martín-Rodríguez, M. et al. Epidemiology and cost of herpes zoster and postherpetic neuralgia among patients treated in primary care centres in the valencian community of Spain. BMC Infect Dis 11, 302 (2011). https://doi.org/10.1186/1471-2334-11-302
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2334-11-302