
Abstract
Background
In adults, impaired myocardial repolarization and increased risk of arrhythmia are known consequences of open heart surgery. Little is known, however, about post-operative consequences of cardiopulmonary bypass surgery in children. The aim of this study was to assess ventricular repolarization and coronary perfusion after bypass surgery for atrial septal defect (ASD) repair in children.
Methods
Twelve patients with ASD were assessed one day before and 5–6 days after ASD repair. Myocardial repolarization (corrected QT interval, QTc, QT dispersion, QTd, and PQ interval) was determined on 12-lead electrocardiograms. Coronary flow in proximal left anterior descending artery (peak flow velocity in diastole, PFVd) was assessed by transthoracic Doppler echocardiography.
Results
Ten of the 12 (83%) children had normal myocardial repolarization before and after surgery. After surgery, QTc increased 1-9% in 5 (42%) patients, decreased 2-11% in 5 (42%) patients and did not change in 2 (16%) patients. Post-op QTc positively correlated with bypass time (R=0.686, p=0.014) and changes in PFVd (R=0.741, p=0.006). After surgery, QTd increased 33-67% in 4 (33%) patients, decreased 25-50% in 6 patients (50%) and did not change in 2 (16%) patients. After surgery, PQ interval increased 5-30% in 4 (33%) patients, decreased 4-29% in 6 (50%) patients and did not change in 1 (8%) patient. Post-op PQ positively correlated with bypass time (R=0.636, p=0.027). As previously reported, PFVd significantly increased after surgery (p<0.001).
Conclusions
Changes in QTc, PQ and PFVd are common in young children undergoing surgery for ASD repair. Post-op QTc significantly correlates with bypass time, suggesting prolonged cardiopulmonary bypass may impair ventricular repolarization. Post-op QTc significantly correlates with PFVd changes, suggesting increased coronary flow may also impair ventricular repolarization. The clinical significance and reversibility of these alternations require further investigations.
Similar content being viewed by others


Background
Cardiopulmonary bypass remains the main approach to surgical repair of most congenital heart diseases. Little, however, is known about potential hemodynamic and electrophysiological consequences of this procedure, especially in young children. Myocardial function and output are usually impaired in congenital heart disease, but may become more so after surgery. Coronary flow increases after cardiopulmonary bypass surgery [1, 2]. In adults, impaired myocardial repolarization and increased risk of arrhythmia are well known consequences of open heart surgery [3]. Early postoperative arrhythmia occurs in about 14% children [4].
QTd (the difference between maximal and minimal QT intervals on a standard ECG) is a risk factor for post-operative ventricular arrhythmia in patients with Tetralogy of Fallot [5, 6]. QTc and QTd increase in left ventricular diastolic dysfunction [7]. Prolonged QRS duration, on the other hand, may result from right or left ventricular dilatation, predicting malignant ventricular arrhythmias [8]. PQ interval increases in diastolic dysfunction, independent of the severity or cause. Moreover, P wave dispersion correlates with left ventricular ejection fraction and is significantly higher in dilated cardiomyopathy and mitral stenosis [9]. Of note, the pattern of ventricular repolarization in male and female infants and children is the same [10, 11].
We recently reported that cardiopulmonary bypass surgery in children leads to increased coronary flow in the first week of surgery [1]. Profound adverse effects (e.g., atrial fibrillation and ventricular arrhythmia) on myocardial repolarization in the same period are also reported in adults [12]. The primary aim of this study was to compare myocardial repolarization (QTc, QTd, and PQ intervals) and coronary flow (PFVd) measurements before and within the first week after cardiopulmonary bypass surgery for ASD repair in children. The secondary aim was to correlate the ECG and PFVd changes with bypass and aortic cross-clamp times.
Methods
Study population
Twelve children who had open heart surgery under cardiopulmonary bypass for ASD repair were included in this study. The mean age was 3.5 ± 1.9 years (range, 1–7). The study was approved by the ethics committee for human research at the Lund University. Written consent was obtained from the guardians/parents of patients enrolled in the study. The study protocol conformed to the principles outlined in the declaration of Helsinki [13]. The exclusion criteria were clinical signs of an infectious illness, C-reactive protein >0.8 mg/L before surgery, heart failure, and preoperative therapy with vasoactive drugs.
The cardio pulmonary bypass surgeries were performed under a body temperature of 28-32°C; cold (+4°C) hyperkalemic blood cardioplegic solution was used. All patients had the same protocol for cardioplegia and anterograde perfusion of the coronary arteries with retrograde filling through the coronary sinus every 20 min. The post-operative intensive care stay was uneventful with no observed arrhythmias.
Patients were not taking beta-blockers, angiotensin 1-converting enzyme inhibitors, angiotensin 1-converting enzyme receptor blockers, lanoxine, phenylepherine or other vasoactive drugs (including nitrate or dopamine). Patients received intravenous ketobemidone hydrochloride for pain during the first 2–3 days. Oral oxicodon, with a half-life of 4.5 hours, was then given on postoperative days 3 and 4. These medications were stopped at least one day before postoperative evaluations (echocardiography and ECG) on day 5 or 6, which were performed when patients were ready for discharge.
ECG measurements
Surface (12-lead) electrocardiograms (ECG Machine-GE Marquette, 12 lead ecg system) were done one day before and 5 or 6 days after surgery. PQ interval and indexes of myocardial repolarization (QTc and QTd) were measured by one investigator. QT was measured manually in leads II, V4, and V5. QTc was calculated using the Bazett’s formula [14]. Three consecutive ECG cycles (whenever possible) in each of the three leads were measured and the mean interval was used. The precedent RR interval to the measured QT was used to calculate the heart rate for QTc interval in milliseconds (ms). QTd was set as the difference between the maximum and minimum QTc, using lead V1 [5].
Transthoracic Doppler echocardiography
Echocardiographic examinations were made with Sequoia™ C512 (Acuson Mountain View, CA, USA) machine with pulsed wave Doppler frequency of 7/10 MHz. Standard M- and B-modes and 2D transthoracic Doppler Echocardiography (TTDE) for cardiac output, left ventricular function and left anterior descending (LAD) coronary artery flow measurements were done one day before and 5 or 6 days after surgery. The diameter of the aortic ring was measured in a long axis view by M-mode in accordance to the recommendations of the American Society of Echocardiography [15]. Left ventricular fractional shortening was computed according to the standard formula [16]. The flow velocity measurements across aortic valve were averaged over three consequent cardiac cycles. Adjustments in the ultrasound machine for measuring diastolic peak flow velocity (PFVd) in the LAD coronary artery were as previously described [1].
Statistics
The data were expressed as mean and standard deviation (±SD). Analyses (standard crosstabs, Pearson correlation coefficients, and linear regression) were performed using SPSS version 20.0 (SPSS Incorporated, Chicago, Illinois). P-values <0.05 were considered significant.
Normality of PFVd, QTc, QTd and PQ changes was confirmed by the Shapiro-Wilk test. Thus, the paired t-test was used to compare pre- and post-operative changes in the measured parameters.
Adequacy of the sample size (n = 12) for detecting true changes, if any, between the pre- and post-operative values of PFVd, QTc, QTd and PQ by paired t-test was assessed. For this purpose, true standard deviations of differences were assumed to be close to the observed standard deviations. Smallest mean differences (pre- vs. post-operative) for detecting with a power of 90% and 5% significance were computed. The smallest mean difference for PFVd was 13.28 cm.s-1 (assumed standard deviation = 13.0 cm.s-1), for QTc was 20.59 ms (assumed standard deviation = 20.0 ms), QTd 15.44 ms (assumed standard deviation = 15.0 ms), and for PQ was 25.74 ms (assumed standard deviation = 25.0 ms).
Results
All children, except patients 11 and 12, had normal myocardial repolarization (QTc and QTd intervals) before and after surgery. Patient 11 had the longest aortic cross-clamp duration (67 min), bypass time (106 min), pre-operative PQ interval (200 ms) and pre-operative QTc (444 ms); PQ and QTc decreased after surgery by 6% and 3%, respectively (Table 1).
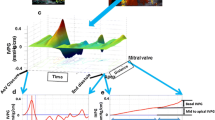
Patient 12 had long post-operative QTc (448 ms) with relatively short aortic cross-clamp time (25 min). This patient had post-operative increase in PQ interval (by 10%), but still within the normal limits. These parameters increased 6-12% compared with the pre-op values. After surgery, QTc increased 1-9% in 5 of 12 (42%) patients, decreased 2-11% in 5 of 12 (42%) patients and did not change in 2 of 12 (16%) patients (Table 1). Post-op QTc positively correlated with bypass time (R=0.686, p=0.014) and changes in PFVd (R=0.741, p=0.006), Figure 1A-C.

A-D. Correlations between post-operative ECG parameters vs. cardiopulmonary bypass time, Δ-LAD PFV and aorta cross clamp time. A; Correlation between post-op QTc and QTd and bypass time. B; Correlation between post-op QTc and QTd and Δ-LAD PFV. C; Correlation between post-op QTc and QTd and aortic cross-clamp time. D; Correlation between post op PQ duration and bypass time and aortic cross-clamp time.
After surgery, QTd increased 33-67% in 4 (33%) patients, decreased 25-50% in 6 (50%) patients and did not change in 2 (16%) patients. The correlations between post-op QTd and PFVd or aortic cross-clamp time were insignificant (Figure 1A-C).
After surgery, PQ interval increased 5-30% in 4 (33%) patients, decreased 4-29% in 6 (50%) patients and did not change in 1 (8%) patient. Post-op PQ positively correlated with bypass time (R=0.634, p=0.027), Figure 1D. The correlations between post-op PQ and PFVd or aortic cross-clamp time were insignificant (Figure 1D).
LAD coronary artery PFVd significantly increased after surgery (p<0.001). Otherwise, the paired t-tests for QTc, QTd and PQ were insignificant.
Hemodynamic and echocardiography data before and after surgery showed no significant changes, except for the systolic blood pressure (p=0.04, Table 2). Cardiac output and its related velocity time integral in the aorta were insignificantly decreased (p = 0.302 and 0.770, respectively) after surgery (Table 2). Left ventricular fraction shortening was the same before and after surgery. There were no significant correlations between postoperative cardiac function (including cardiac output) and myocardial repolarization parameters.
Discussion
The study describes early changes in ventricular repolarization (QTc, QTd), PQ interval and coronary flow (PFVd) shortly after cardiopulmonary bypass for ASD repair in children. This surgical procedure was associated with significant changes in these parameters in most patients. Some changes were partially related to the bypass and aortic cross-clamp times (Figure 1). Thus, prolonged intra-operative procedure may have an adverse impact on myocardial repolarization, imposing some risk of arrhythmia after surgery. This possibility needs further investigation, especially with extended time following surgery.
The cross clamp duration shown here is comparable with that reported for ASD repair (35 ± 17 vs. 24 ± 16 min) [17]. Three of our 12 patients had associated congenital heart defects, such as partial anomalous pulmonary venous return. For these children, the cardiopulmonary bypass time was >100 min. Otherwise, the bypass time for the remaining 8 children was 61 ± 12 min, which is comparable with published report (42 ± 16 min) [17].
ASD causes right atrial dilatation and right ventricular volume overload. These alterations along with incision made through the right atrium and bypass time during surgery likely impact the myocardial repolarization. The overall effects are variable and their clinical significance remains uncertain. Further studies are needed to address reversibility and significance of these changes.
Impaired myocardial repolarization (and its associated risk of arrhythmia) in the immediate post-operative period perhaps could be deduced from the significant correlations between duration of bypass and post-op QTc or PQ intervals (Figure 1). A recent study of various congenital heart diseases showed persistently prolonged QTc >3 days after surgery in about one-third of the patients [18]. A transient prolongation of QTc is also reported in adults during myocardial infarction and balloon coronary angioplasty [19, 20].
The post-operative increase of coronary artery flow could have a mechanistic link to ventricular repolarization, accounting (at least partially) for the significant correlation between PFVd changes and post-op QTc (Figure 1B). This finding is in line with the animal study by Zhang et al., where increased coronary flow was associated with prolonged duration of transmural ventricular repolarization [21]. The underlying mechanism of flow-induced lengthening of ventricular repolarization is unclear, but synthesis and release of nitric oxide from the coronary endothelium may play a role [22]. The right ventricular volume and pressure are increased in ASD, raising the demand for oxygen. The coronary flow, thus, is expected to increase in these patients. These findings become more prominent after cardiopulmonary bypass surgery [23]. Patients with limited coronary flow reserve (e.g., prolonged aortic cross-clamping duration and enhanced microcirculatory changes), however, may fail to execute adequate oxygen supply to the myocardium. Such patients may have complicated post-op course, particularly with sepsis. Therefore, assessing coronary flow is important in critically-ill children.
Conclusions
Changes in myocardial repolarization (QTc), PQ interval and coronary perfusion (PFVd) are common in young children undergoing cardiopulmonary bypass surgery for ASD repair. Post-op QTc significantly correlates with bypass time, suggesting prolonged cardiopulmonary bypass may impair ventricular repolarization. Post-op QTc also significantly correlates with PFVd changes, suggesting the post-op increase in coronary flow may impair ventricular repolarization. The clinical significance and reversibility of these alternations require further investigations.
Limitations of the study
The study was conducted in a small cohort. To avoid stress on child and parents, the coronary flow reserve was not done.
Abbreviations
- ASD:
-
Atrial septal defect
- QTc:
-
Corrected QT interval
- QTd:
-
QT dispersion
- LAD:
-
Left anterior descending
- PFVd:
-
Peak flow velocity in diastole
- ECG:
-
Electrocardiogram
- TTDE:
-
Transthoracic doppler echocardiography
- SD:
-
Standard deviation
- SV:
-
Sinus venosus
- VTI:
-
Velocity time integral
- VTId+s:
-
Velocity time integral in diastole and systole
- BP:
-
Blood pressure
- HR:
-
Heart rate
- RPP:
-
Rate pressure product
- FS:
-
Fractional shortening
- LVM:
-
Left ventricular mass
- CO:
-
Cardiac output
- CPB:
-
Cardiopulmonary bypass
- VTId+s:
-
Velocity time integral in diastole and systole
- BF:
-
Blood flow
- TTDE:
-
Transthoracic doppler echocardiography.
References
Aburawi EH, Berg A, Liuba P, Pesonen E: Effects of cardiopulmonary bypass surgery on coronary flow in children assessed with transthoracic Doppler echocardiography. Am J Physiol Heart Circ Physiol. 2007, 293: H1138-1143. 10.1152/ajpheart.00025.2007.
Aburawi EH, Pesonen E: Pathophysiology of coronary blood flow in congenital heart disease. Int J Cardiol. 2011, 151: 273-277. 10.1016/j.ijcard.2010.05.048.
Steeds RP, Okley D: Predicting late sudden death from ventricular arrhythmia in adults following surgical repair of tetralogy of Fallot. Q J Med. 2004, 97: 7-13. 10.1093/qjmed/hch004.
Valsangiacomo E, Schmid ER, Schüpbach RW, Schmidlin D, Molinari L, Waldvogel K, Bauersfeld U: Early postoperative arrhythmias after cardiac operation in children. Ann Thorac Surg. 2002, 74: 792-796. 10.1016/S0003-4975(02)03786-4.
Rekawek J, Kansy A, Miszczak-Knecht M, Manowska M, Bieganowska K, Brzezinska-Paszke M, Szymaniak E, Turska-Kmieć A, Maruszewski P, Burczyński P, Kawalec W: Risk factors for cardiac arrhythmias in children with congenital heart disease after surgical intervention in the early postoperative period. J Thorac Cardiovasc Surg. 2007, 133: 900-904. 10.1016/j.jtcvs.2006.12.011.
Gatzoulis MA, Till JA, Redington AN: Depolarization-repolarization inhomogeneity after repair of tetralogy of Fallot. The substrate for malignant ventricular tachycardia?. Circulation. 1997, 95: 401-404. 10.1161/01.CIR.95.2.401.
Gunduz H, Akdemir R, Binak E, Tamer A, Uyan C: Relation between stage of left ventricular diastolic dysfunction and QT dispersion. Acta Cardiol. 2003, 58: 303-308. 10.2143/AC.58.4.2005287.
Helbing WA, Roest AA, Niezen RA, Vliegen HW, Hazekamp MG, Ottenkamp J, de Roos A, van der Wall EE: ECG predictors of ventricular arrhythmias and biventricular size and wall mass in tetralogy of Fallot with pulmonary regurgitation. Heart. 2002, 88: 515-519. 10.1136/heart.88.5.515.
Senen K, Turhan H, Riza Erbay A, Basar N, Saatci Yasar A, Sahin O, Yetkin E: P-wave duration and P-wave dispersion in patients with dilated cardiomyopathy. Eur J Heart Fail. 2004, 6: 567-569.
Stramba-Badiole M, Spagniolo D, Bosi G, Schwartz PJ: Are gender differences in QTc present at birth?. Am J Cardiol. 1995, 75: 1277-1278. 10.1016/S0002-9149(99)80781-4.
Rautaharju PM, Zhou SH, Wong S, Calhoun HP, Berenson GS, Prineas R, Davignon A: Sex differences in the evolution of the electrocardiographic QT interval with age. Can J Cardiol. 1992, 8: 690-695.
Lamm G, Auer J, Weber T, Berent R, Ng C, Eber B: Postoperative white blood cell count predicts atrial fibrillation after cardiac surgery. J Cardiothorac Vasc Anesth. 2006, 20: 51-56. 10.1053/j.jvca.2005.03.026.
World Medical Association Declaration of Helsinki: Recommendations guiding physicians in biomedical research involving human subjects. Cardiovasc Res. 1997, 35: 2-3.
Bazette H: An analysis of the time-relation of electrocardiograms. Heart. 1920, 7: 353-367.
Postema PG, De Jong JS, Van der Bilt IA, Wilde AA, AccurateLang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al: Chamber quantification writing group; American society of Echocardiography's guidelines and standards committee; European association of echocardiography. Recommendations for chamber quantification: a report from the American society of Echocardiography's guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the European association of echocardiography, a branch of the European society of cardiology. J Am Soc Echocardiogr. 2005, 18: 1440-1463. 10.1016/j.echo.2005.10.005.
Lewis RP, Sandler H: Relationship between changes in the left ventricular dimension and ejection fraction in man. Circulation. 1971, 44: 548-457. 10.1161/01.CIR.44.4.548.
Stavinoha PL, Fixler DE, Mahony L: Cardiopulmonary bypass to repair an atrial septal defect does Not affect cognitive function in children. Circulation. 2003, 107: 2722-2725. 10.1161/01.CIR.0000070620.97086.65.
Punn R, Lamberti JJ, Balise RR, Seslar SP: QTc prolongation in children following congenital cardiac disease surgery. Cardiol Young. 2011, 21: 400-410. 10.1017/S1047951111000175.
Kenigsberg DN, Khanal S, Kowalski M, Krishnan SC: Prolongation of the QTc interval is seen uniformly during early transmural ischemia. J Am Coll Cardiol. 2007, 49: 1299-1305. 10.1016/j.jacc.2006.11.035.
Kawabata M, Hirao K, Takeshi S, Sakurai K, Inagaki H, Hachiya H, Isobe M: Torsades de pointes related to transient marked QT prolongation following successful emergent percutaneous coronary intervention for acute coronary syndrome. J Electrocardiol. 2008, 41: 117-122. 10.1016/j.jelectrocard.2007.09.009.
Zhang Y-Z, He B, Wang L-X: Effect of an increase in coronary perfusion on transmural ventricular repolarization. Physiol Res. 2007, 56: 285-290.
Li JT, Wang LX: Prolonged action potential duration of ventricular myocytes. Arch Med Res. 2006, 37: 27-30. 10.1016/j.arcmed.2005.05.016.
Aburawi EH, Berg A, Pesonen E: Coronary flow before and after surgical versus device closure of atrial septal defect. Int J Cardiol. 2009, 135: 14-20. 10.1016/j.ijcard.2008.03.046.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2261/13/67/prepub
Acknowledgments
The authors would like to thank the personnel of Skane University Hospital, Lund and the Faculty of Medicine, Lund University. We would extend our gratitude to Samariten Foundation (Sweden) for their financial support of this study (EHA). We thank Annica Maxedius, registered research nurse, for assistance in patient recruitment.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
There are no potential, perceived, or real conflicts of interest.
Authors’ contributions
EHA, PL and EP designed the study and get the ethical approval. EHA and A-KS analyzed the data and prepared the first draft of the manuscript. PL and EP revised and edited the manuscript. TZ performed the statistical analysis. All authors have read and approved the final version of the manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Aburawi, E.H., Souid, AK., Liuba, P. et al. Early changes in myocardial repolarization and coronary perfusion after cardiopulmonary bypass surgery for ASD repair in children. BMC Cardiovasc Disord 13, 67 (2013). https://doi.org/10.1186/1471-2261-13-67
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2261-13-67