
Abstract
Background
The association between the human cytotoxic T lymphocyte-associated antigen-4 (CTLA4) gene and insulin-dependent diabetes mellitus (IDDM) is unclear in populations. We therefore investigated whether the gene conferred susceptibility to IDDM in a Russian population. We studied two polymorphic regions of the CTLA4 gene, the codon 17 dimorphism and the (AT)n microsatellite marker in the 3' untranslated region in 56 discordant sibling pairs and in 33 identical by descent (IBD) affected sibships.
Results
The Ala17 allele of the CTLA4 gene was preferentially transmitted from parents to diabetic offspring (p < 0.0001) as shown by the combined transmission/disequlibrium test (TDT) and sib TDT (S-TDT) analysis. A significant difference between diabetic and non-diabetic offspring was also observed for the transmission of alleles 17, 20, and 26 of the dinucleotide microsatellite. Allele 17 was transmitted significantly more frequently to affected offspring than to other children (p = 0.0112) whereas alleles 20 and 26 were transmitted preferentially to non-diabetic sibs (p = 0.045 and 0.00068 respectively). A nonrandom excess of the Ala17 CTLA4 molecular variant (maximum logarithm of odds score (MLS) of 3.26) and allele 17 of the dinucleotide marker (MLS = 3.14) was observed in IBD-affected sibling pairs.
Conclusion
The CTLA4 gene is strongly associated with, and linked to IDDM in a Russian population.
Similar content being viewed by others


Introduction
The cytotoxic T lymphocyte-associated antigen 4 gene (CTLA4) encodes the T cell receptor involved in the control of T cell proliferation and mediates T cell apoptosis [1]. The receptor protein is a specific T lymphocyte surface antigen that is detected on cells only after antigen presentation. Thus, CTLA4 is directly involved in both immune and autoimmune responses and may be involved in the pathogenesis of multiple T cell-mediated autoimmune disorders.
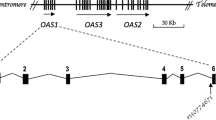
The human CTLA4 gene was mapped to chromosome 2q33 [2]. It consists of three exons. The first encodes a V-like domain of 116 amino acids. An A-to-G substitution at nucleotide 49 in exon 1 results in an amino acid substitution (Thr/Ala) in the leader peptide of the protein [3]. The Ala allele has been shown to predispose the individual carrying it to the development of various immune diseases including Graves' disease [3, 4], Hashimoto's thyroiditis [5], Addison's disease [5], rheumatoid arthritis [6, 7], celiac disease [8, 9], and others [10].
The Thr17Ala dimorphism and the polymorphic (AT)n microsatellite starting at position 642 of the 3' untranslated region flanking exon 4 of the CTLA4 gene and located 5.3 kb 3' of the biallelic codon 17 were shown to be linked to, and associated with, insulin-dependent diabetes mellitus (IDDM) in Italian diabetic families [11]. This led Nistico et al. [11] to refer to the susceptibility to diabetes associated with CTLA4 as IDDM12. Further evidence for an IDDM susceptibility locus on chromosome 2 in 2q33, the region containing the CTLA4 gene, has been provided from various ethnic groups including Caucasians (British, Spanish, French, Swedish, and Belgian), Mexican-Americans, and Asians (Korean, Chinese, Japanese) [3, 12–17]. In contrast, a lack of association of the CTLA4 gene with IDDM was observed in other Caucasian populations including Sardinians [12], Germans [18], Danish [19], and U.S. whites [20].
We therefore decided to investigate whether this gene conferred susceptibility to IDDM in a Russian population. We carried out family studies using two polymorphic markers at the CTLA4 gene locus: codon 17 dimorphism and the dinucleotide microsatellite in the 3' untranslated region.
Results
We observed preferential transmission of the Ala allele of the CTLA4 gene from parents to diabetic offspring (Table 1). The observed difference in transmission was highly significant, as shown by the transmission disequilibrium test (TDT) and combined TDT and sib TDT (S-TDT) analysis (p < 0.0001).
For another polymorphic marker of the CTLA4 gene, the dinucleotide microsatellite, we detected 17 alleles from 92 to 130 bp in length. Alleles were designated according to the number of repeat units. For instance, the smallest allele contained 11 AT repeats and was referred to as allele 11. A significant difference between diabetic and non-diabetic offspring was observed for the transmission of three alleles numbers 17, 20, and 26, in combined TDT and S-TDT analysis (Table 2). Allele 17 was transmitted significantly more frequently to affected than to unaffected sibs (P = 0.0112) whereas alleles 20 and 26 were preferentially transmitted to non-diabetic sibs (P = 0.045 and 0.00068).
We assessed the linkage to IDDM of both polymorphic markers of the CTLA4 gene in affected sibling pairs (ASPs), identical by descent (IBD), by assessing the significance of the deviation of the observed IBD allele distribution from a random distribution (Table 3). A nonrandom excess of the Ala17 allele was observed in IDDM ASPs (χ2 = 24.892, df = 1, p = 0.000015), with a logarithm of odds (LOD) score of 3.54. After correction for the number of alleles at this marker (2), our maximum LOD score (MLS) was reduced to 3.24 (Table 3). For the dinucleotide microsatellite, a MLS of 4.37 was obtained for the allele 17. Correction for the number of observed alleles (17) decreased the value to 3.17. Allele 17 displayed a distribution in APSs differed significantly from a random distribution (χ2 = 64.884, df = 2, p < 0.000001).
Discussion and conclusion
TDT and S-TDT analyses revealed that both markers within the CTLA4 gene were significantly associated with IDDM in a Russian population. Both TDT and combined tests showed a clear association of the Thr17Ala dimorphism in the gene (Table 1). For the second polymorphic marker tested, the dinucleotide microsatellite, a significant difference in the transmission of the three alleles was observed, even after correction for multiple alleles (Table 2). This suggests that the (AT)n repeat polymorphism of the CTLA4 gene is associated with IDDM in this Russian population.
Transmission disequilibrium analysis in discordant sibling pairs showed that the Ala17 variant of the CTLA4 gene and allele 17 at the intragenic dinucleotide microsatellite were associated with a high risk of IDDM. The maximum LOD scores were also sufficient to indicate that the CTLA-4 region of chromosome 2q33 is linked to, and associated with, IDDM in a Russian population.
Thus, our findings are consistent with those of earlier family studies showing a positive association between the CTLA4 gene and IDDM in most populations tested and role of the Ala17 allele is predisposing the individual to the disorder [3, 11–17]. Linkage analysis with a CTLA4 dinucleotide marker in 48 Italian IDDM families gave a ML of 3.22 which is consistent with our results [11]. Our findings suggest that allele 17 is a common 'predisposition' allele of the dinucleotide marker. Our data are consistent with those of Marron et al. [12] who reported a significantly higher frequency of allele 17 to affected siblings in pooled diabetic pedigrees from multiple ethnic groups than of other alleles of the dinucleotide marker. Allele 17 was in strong linkage disequilibrium with the Ala allele in the Russian population and in other populations tested (data not shown) [12].
The CTLA4 gene (IDDM12) is located in the vicinity of two other IDDM susceptibility regions, IDDM7 (2q31) [21] and IDDM13 (2q34) [22], and the genes encoding CD28, IA-2 and islet tyrosine phosphatase, which may be considered to be candidate IDDM susceptibility genes [23]. This closeness to other IDDM susceptibility regions and putative susceptibility genes may account for the weakness or absence of association of the CTLA4 gene with IDDM in some populations.
A functional significance of the CTLA4 codon 17 dimorphism is unknown. The amino acid substitution thought unlikely to affect the function of the CTLA-4 molecule. The CTLA4 microsatellite (AT)n repeat may affect RNA stability, for the AT-rich sequences in 3' untranslated regions of mRNA molecules for example [24, 25]. Linkage between the two CTLA4 polymorphic markers has been shown [26]. This may indirectly affect CTLA4 signal transduction or intracellular sorting [27]. The Ala17 allele is probably correlated with rapid-onset insulin deficiency, and functional studies with Ala/Ala homozygous patients may elucidate the functional significance of codon 17 dimorphism in T-cell regulation [28].
CTLA4 is known to be involved in the fine tuning of the immune response, the disruption of which may result in autoimmunity. Recent animal model-based studies have shown that CTLA4Ig injection can prevent relapse of the autoimmune process in BB rats [28]. This suggests that CTLA4 may be a suitable target for the specific prevention of β-cell autoimmunity [27].
Our data, showing the linkage and association of the CTLA4 gene with IDDM, together with many other population-based fundings, suggest that the chromosome 2q33 region (IDDM12) is a true IDDM susceptibility locus. The CTLA4 region may function as a common locus for HLA.genes and genes conferring susceptibility to autoimmunity in general. A number of findings, including our studies of association between CTLA4 codon 17 and Graves' disease [29], support this view.
Materials and methods
Subjects
Fifty-six Russian families, each consisting of two siblings (one affected with IDDM diagnosed before the age of 18 years and one non-diabetic sibling) were studied. Sixteen families were recruited from The Samara Diabetic Center, the other families being recruited from the Endocrinological Research Center in Moscow. Thirty-three nuclear diabetic families, recruited from the Endocrinological Research Center and consisting of two unaffected parents and two sibs with IDDM, were also analysed.
DNA typing
Human DNA was extracted from whole blood using a phenol-chloroform technique [30]. A polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) assay was used to detect Thr17Ala dimorphism as described by Donner et al. [3]. The dinucleotide repeat polymorphism was studied by PCR, as described by Polymeropoulos et al. [31]. DNA fragments were separated by electrophoresis in 12% polyacrylamide gels and stained with silver nitrate [32].
Statistical analysis
We carried out linkage disequilibrium analysis in discordant sibling pairs by combined TDT and S-TDT analysis [33, 34]. For TDT, we estimated the significance of deviations from a random pattern of allele transmission was estimated using the χ2 test. For both S-TDT and the combined test, a z score was calculated for each allele. A nominal P value of less than 0.05 after correction for multiple alleles was considered significant.
Linkage between polymorphic markers and susceptibility to IDDM was assessed in APSs by assessment of the extent to which the observed distribution of shared alleles, identical by descent, differed from a random distribution (1:2:1 for sharing of 2, 1, and 0 alleles would be expected). Parents homozygous for an allele were considered to be genetically uninformative. χ2 was calculated using Roff & Bentzen's algorithm [35] to determine the significance of the degree of excess allele sharing by ASPs. The logarithm of odds score was calculated as described by Risch [36] using correction for the number of alleles tested [37]. A LOD score of 3.0 or more was considered to indicate significant linkage.
References
Waterhouse P, Penninger JM, Timms E, Wakeham A, Stahinaian A, Lee KP, Thompson CB, Griesser H, Mak TW: Lymphoproliferative disorders with early lethality in mice deficient in Ctla-4. Science. 1995, 270: 985-988.
Dariavach P, Mattei M-G, Golstein P, Leframc M-P: Human Ig superfamily CTLA-4 gene localization and organization. Cytogenet Cell Genet. 1989, 51: 983-
Donner H, Rau H, Walfish PG, Braun J, Siegmund T, Finke R, Herwig J, Usadel KH, Badenhoop K: CTLA4 alanine-17 confers genetic susceptiblity to Graves' disease and type 1 diabetes mellitus. J Clin Endocrinol Metab. 1997, 82: 143-146.
Yanagawa T, Taniyama M, Enomoto S, Gomi K, Maruyama H, Ban Y, Saruta T: CTLA4 gene polymorphism confers genetic suspectiblity to Graves' disease in Japanese. Thyroid. 1997, 7: 843-846.
Donner H, Braun J, Seidl C, Rau H, Finke R, Ventz M, Walfish PG, Usadel KH, Badenhoop K: Codon 17 polymorphism of the cytotoxic T lymphocyte antigen 4 gene in Hashimoto's thyroiditis and Addison's disease. J Clin Endocrinol Metab. 1997, 82: 4130-4132.
Seidl C, Donner H, Fischer B, Usadel KH, Sefried E, Kaltwasse JP, Badenhoop K: CTLA4 codon dimorphism in patients with reumathoid arthritis. Tissue Antigens. 1998, 51: 62-66.
Gonzales-Esribano MF, Rodriguez R, Valenzuela A, Garcia A, Garcia-Lozano JR, Nunez-Roldan A: CTLA4 polymorphism in Spanish patients with reumathoid arthritis. Tissue Antigens. 1999, 53: 296-300. 10.1034/j.1399-0039.1999.530311.x.
Djilali-Saiah I, Schmitz J, Harfouch-Hammoud E, Mougenot J-F, Bach J-F, Caillat-Zucman S: CTLA-4 gene polymorphism is associated with predisposition to celiac disease. Gut. 1998, 43: 187-189.
Naluai AT, Nillsson S, Samuellson L, Gudjonsdottir AH, Ascher H, Ek J, Hallberg B, Kristiansson B, Martinsson T, Nerman O, Sollid LM, Walhstrom J: The CTLA4/CD28 gene region on chromosome 2q33 confers suspectibility to celiac disease in a way possibly distinct from that of type 1 diabetes and other chronic inflammatory disorders. Tissue Antigens. 2000, 56: 350-355. 10.1034/j.1399-0039.2000.560407.x.
Sayegh MH: Finally, CTLA4Ig graduates to the clinic. J Clin Invest. 1999, 103: 1223-1225.
Nistico L, Buzzetti R, Pritchard LE, Van der Auvera B, Giovannini C., Bosi E, Martinez-Larrad MT, Serrano-Rios M, Chow CC, Kockram CS, Jacobs K, Mijovic C, Bain SC, Barnett A, Vandevalle CL, Schuit F, Gorus FK, Tosi R, Pozzilli P, Todd JA: The CTLA-4 region of chromosome 2q33 is linked to, and associated with, type 1 diabetes. Hum Mol Genet. 1996, 5: 1075-1080. 10.1093/hmg/5.7.1075.
Marron MP, Raffel LJ, Garchon HJ, Jacob CO, Serrano-Rios M, Martinez-Larrad MT, Teng VP, Park J, Zhang ZX, Goldstein DR, Tao JW, Beaurain G, Bach JF, Huang HS, Luo DF, Zeidler A, Rotter JI, Yang MC, Modilevsky T, Maclaren NK, She JX: Insulin-dependent diabetes mellitus (IDDM) is associated with CTLA4 polymorphisms in multiple ethnic groups. Hum Mol Genet. 1997, 6: 1275-1282. 10.1093/hmg/6.8.1275.
Marron MP, Zeidler A, Raffel LJ, Eckenrode SE, Yang JJ, Hopkins DJ, Garchon HJ, Jacob CO, Serrano-Rios M, Martinez-Larrad MT, Park Y, Bach JF, Rotter JL, Yang MC, She XC: Genetic and physical mapping of a type 1 diabetes susceptibility gene (IDDM12) to a 100-kb phagemid artificial chromosome clone containing D2S72-CTLA4-D2S105 on chromosome 2q33. Diabetes. 2000, 49: 492-499.
Awata T, Kurihara S, Iitaka M, Takei SI, Inoe I, Ishii C, Negishi K, Izumida T, Yoshida Y, Hagura R, Kuzuya N, Knazawa Y, Katayama S: Association of CTLA-4 gene A-G polymorphism (IDDM12) locus with acute-onset and insulin-depleted IDDM as well as autoimmune thyroid disease (Graves' disease and Hashimoto's thyroiditis) in the Japanese population. Diabetes. 1998, 47: 128-129.
Abe T, Takino H, Yamasaki H, Ozaki M, Sera Y, Kondo H, Samasaki H, Kawasaki E, Awata T, Yamaguchi Y, Eguchi K: CTLA4 gene polymorphism correlates with the mode of onset and presence of ICA52 Ab in Japanese type 1 diabetes. Diabetes Res Clin Pract. 1999, 46: 169-175. 10.1016/S0168-8227(99)00084-4.
Lee YJ, Huang FY, Lo FS, Wang WC, Hsu CH, Kao HA, Yang TJ, Chang JG: Association of CTLA4 gene A-G polymorphism with type 1 diabetes in Chinese children. Clin Endocrinol. 2000, 52: 153-157. 10.1046/j.1365-2265.2000.00929.x.
Lowe RM, Sund SG, Graham KI, Lamdin-Olsson M, Lernmark A: The 3'-end CTLA4 gene (AT) microsatellite is associated with type 1 diabetes in 0–34 year old Swedish patients and controls. Diabetes. 1998, 47 (Suppl 2): A204-
Badenhoop K, Donner H, Pani M, Rau H, Siegmund T, Braun J: Genetic susceptibility to type 1 diabetes: clinical and molecular heterogeneity of IDDM1 and IDDM12 in a German population. Exp Clin Endocrinol Diabetes. 1999, 107 (Suppl 3): S89-92.
Larsen ZM, Kristiansen OP, Mato E, Johannesen J, Puig-Domingo M, de Leiva A, Nerup J, Pociot F: IDDM12 (CTLA4) on 2q33 and IDDM13 on 2q34 in genetic susceptibility to type 1 diabetes (insulin-dependent). Autoimmunity. 1999, 31: 35-42.
Owerbach D, Naya FJ, Tsai MJ, Allander SV, Powell DR, Gabbay KH: Analysis of candidate genes for susceptibility to type 1 diabetes: a case-control and family-association study of genes on chromosome 2q31-35. Hum Mol Genet. 1997, 46: 1275-1282.
Owerbach D, Gabbay KH: The HOXD8 locus (2q31) is linked to type 1 diabetes: interaction with chromosome 6 and 11 disease susceptibility genes. Diabetes. 1995, 44: 132-136.
Morahan G, Huang D, Tait BD, Colman PG, Harrison IC: Markers on distal chromosome 2q linked to insulin-dependent diabetes mellitus. Science. 272: 1811-1813.
Lan MS, Modi WS, Xie H, Notkins AL: Assignment of the IA-2 gene encoding an autoantigen in IDDM to chromosome 2q35. Diabetologia. 1996, 39: 1001-1012. 10.1007/s001250050545.
Yanagawa T, Hidaka Y, Guimaraes V, Soliman M, DeGroot LJ: CTLA-4 gene polymorphism associated with Graves' disease in a Caucasian population. J Clin Endocrinol Metab. 1995, 80: 41-45.
Shaw G, Kamen R: A conserved AU sequence from the 3' untranslated region of GM-CSF gene mediates selective mRNA degradation. Cell. 1986, 46: 659-667.
Donner H, Seidl H, Braun J, Siegmund T, Herwig J, Seifried E, Usadel KH, Badenhoop K: CTLA4 gene haplotypes cannot protect from IDDM in the presence of high risk HLA DQ8 or DQ2 alleles in German families. Diabetes. 1998, 47: 1158-1160.
Badenhoop K: CTLA4 variants in type 1 diabetes: some stirrups serve better backing endocrine autoimmunity. Clin Endocrinol. 2000, 52: 139-140. 10.1046/j.1365-2265.2000.00953.x.
Uchikoshi F, Yang ZD, Rostami S, Yokoi Y, Capocci P, Barker CF, Naji A: Prevention of autoimmune recurrence and rejection by adenovirus-mediated CTLA4Ig gene transfer to the pancreatic graft in BB rat. Diabetes. 1999, 48: 652-657.
Chistiakov DA, Savost'anov KV, Turakulov RI, Petunina NA, Trukhina LV, Kudinova AV, Balabolkin MI, Nosikov VV: Complex association analysis of Graves disease using a set of polymorphic markers. Mol Genet Metab. 2000, 70: 214-218. 10.1006/mgme.2000.3007.
Mathew CGP: The isolation of high molecular weight eukaryotic DNA. In Methods of Molecular Biology. Edited by: Walker J. 1984, Humana Press, 2: 31-34. 10.1385/0-89603-064-4:31.
Polymeropoulos MH, Xiao H, Rath DS, Merril CR: Dinucleotide repeat polymorphism at the human CTLA4 gene. Nucleic Acids Res. 1991, 19: 4018-
Budowle B, Chakraborty R, Giusti AM, Eisenberg AJ, Allen RC: Analysis of the VNTR locus D1S80 by PCR followed by high-resolution PAGE. Am J Hum Genet. 1991, 48: 137-144.
Spielman RS, Ewens WJ: A sibship test for linkage in the presence of association: the sib transmission/disequilibrium test. Am J Hum Genet. 1998, 62: 450-458. 10.1086/301714.
Spielman RS, McGinnis RE, Ewens WJ: Transmission test for linkage disequilibrium: the insulin gene region and insulin-dependent diabetes mellitus (IDDM). Am J Hum Genet. 1993, 52: 506-516.
Roff DA, Bentzen P: The statistical analysis of mitochondrial DNA polymorphisms: χ2 and problem of small samples. Mol Biol Evol. 1989, 6: 539-545.
Risch N: Linkage strategies for genetically complex traits. II The power of affected relative pairs. Am J Hum Genet. 1990, 46: 229-241.
Kidd KK, Ott J: Power and sample size in linkage studies. Cytogenet Cell Genet. 1984, 37: 510-511.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chistiakov, D.A., Savost'anov, K.V. & Nosikov, V.V. CTLA4 gene polymorphisms are associated with, and linked to, insulin-dependent diabetes mellitus in a Russian population. BMC Genet 2, 6 (2001). https://doi.org/10.1186/1471-2156-2-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2156-2-6