
Abstract
Introduction
Although bDMARDs are effective in the treatment of RA, they are associated with dose-dependent side effects, patient burden, and high costs. Recently, many studies have investigated the possibility of discontinuing or tapering bDMARDs when patients have reached their treatment goal. The aim of this review is to provide a narrative overview of the existing evidence on bDMARD dose reduction and to provide answers to specific dose-reduction-related questions that are of interest to clinicians.
Methods
We systematically searched for relevant studies in four scientific databases. Furthermore, we screened the references of reviews and relevant studies.
Results
Our searches resulted in 45 original studies of bDMARD dose reduction in RA patients (15 RCTs and 30 observational studies). Current evidence shows that bDMARD dose reduction can be considered in all RA patients who achieve stable (e.g., ≥6 months) low disease activity or remission. The best strategies seem to be disease-activity-guided dose optimization and fixed dose reduction, since direct bDMARD discontinuation (without restarting) results in a high flare rate, worse physical functioning, and more joint damage. When tapering the bDMARD treatment of a patient, disease activity should be monitored closely, and if a flare occurs, the dose should be increased to the lowest effective dose. Current evidence shows that restarting bDMARD treatment is effective and safe. Unfortunately, no clear predictors of successful dose reduction have been identified so far.
Conclusion
The current evidence and rising healthcare costs urge that dose reduction should be considered for eligible patients. However, the decision to start dose reduction should be made in shared decision-making. Future research should focus not only on a better understanding of the effects of dose reduction on clinical outcomes but also on the perspectives of patients and physicians as well as the implementation of this new treatment principle.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Background
The introduction of biological disease-modifying antirheumatic drugs (bDMARDs) almost two decades ago has improved the treatment of patients with rheumatoid arthritis (RA) by offering more treatment options to be used according to the tight control principle. bDMARDs improve clinical, functional, and radiographic outcomes, and are a welcome—although not clearly superior—addition to existing therapies with synthetic DMARDs (sDMARDs) such as methotrexate, leflunomide, and prednisone [1]. bDMARDs can be categorized into those that act as an inhibitor of tumor necrosis factor (TNFi) and those that have another mechanism of action (non-TNFi).
Although bDMARDs are effective in the treatment of RA, they are associated with high costs, patient burden, and dose-dependent side effects, such as an increased risk of infection [2,3,4,5]. Because of these downsides, many studies have recently investigated the possibility of discontinuing or tapering bDMARDs when patients have reached their treatment goal, which is most often low disease activity (LDA) or remission [6, 7]. Based on evidence from these studies, the EULAR and ACR have incorporated the option of dose reduction into their latest guidelines, the central axiom being “maintenance of treatment goal does not necessarily mean maintenance of treatment intensity” [8, 9].
For clinical practice, however, several questions about the optimal strategy for dose reduction/discontinuation need to be answered in order to properly implement bDMARD dose optimization. Therefore, the goal of this review is to provide a narrative overview of the existing evidence on this topic, to provide answers to specific dose-reduction-related questions that are of interest to clinicians, and to suggest topics for future research.
Questions
We aimed to answer the following clinically relevant questions when considering dose reduction of a bDMARD in an individual RA patient with low disease activity:
-
1.
What are the mechanisms behind the possibility of bDMARD dose reduction in RA patients?
-
2.
In which patients and when should we consider dose reduction?
-
3.
What is the best dose-reduction strategy?
-
4.
What proportion of the patients can be stopped or tapered, and can we predict successful dose reduction using patient or treatment characteristics?
-
5.
What are the effects of dose reduction on function, quality of life, adverse events, and radiographic damage?
-
6.
Which flare criterion is best to use when deciding whether to restart/re-escalate treatment, and how often should the patient be monitored?
-
7.
Is it effective and safe to restart treatment?
-
8.
What is the cost-effectiveness of dose reduction?
-
9.
How can dose reduction best be implemented in clinical practice?
-
10.
What is the patient perspective on bDMARD dose reduction?
Methods
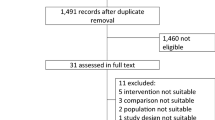
To find relevant studies for this review, we searched CENTRAL, MEDLINE, EMBASE, and Web of Science (only for TNFi) from January 1, 1995 to August 17, 2016. We performed separate searches for TNFi bDMARDs and non-TNFi bDMARDs. To be included in this review, studies had to address RA, dose reduction/discontinuation/tapering of bDMARDs after LDA or remission, and at least one of the topics that we identified for this review. Articles describing original research, ≥20 participants, and a follow-up of ≥6 months were included. Furthermore, we identified relevant reviews on the topic of bDMARD dose reduction. The search strategies are provided in Appendix 1 of the Electronic supplementary material (ESM).
We also sought relevant studies by screening the references included in reviews of this field and those included in the studies that had already been accepted for inclusion in this work. In addition, studies that were already known to the authors from previous research, meetings/conferences, or personal communications were considered for inclusion. No meta-analyses were performed because our aim was to answer several questions in a narrative manner and not to obtain summarized estimates for one or two outcomes. For the same reason, and also due to feasibility, we did not formally assess the risk of bias in the included studies.
Since this article is based on previously conducted studies, and does not involve any new studies of human or animal subjects performed by any of the authors, no ethical approval was necessary.
Results
General Results
Our searches and the subsequent reference screening process resulted in 45 original studies of bDMARD dose reduction in RA patients after attainment of low disease activity or remission (Table 1). Fifteen of these studies were randomized controlled trials (RCTs) that were specifically designed to compare dose reduction with continuation of bDMARDs. The other 30 articles addressed research in which dose reduction was investigated in a nonrandomized manner (observational), or in which one arm of a randomized study fulfilled the inclusion criteria but a nontapering control group was not included. The first study of this subject was published in 2002, and there was an evident increase in the number of studies published on this topic in the years that followed. Most of the studies focused on TNFi reduction (especially etanercept and adalimumab). None of the studies investigated anakinra or golimumab reduction, and very few focused on certolizumab pegol reduction.
There is marked methodological heterogeneity among these studies (as has already been noted by Yoshida et al. and Fautrel et al. [6, 10]) in terms of, for example, the design itself (RCTs, extensions of RCTs, observational studies, and superiority versus non-inferiority designs), inclusion criteria for dose reduction (remission or LDA with variety in duration, with or without concomitant DMARD, tapering soon after the start of treatment or in a later phase), and the definition of flare. However, for the latter, criteria based on the Disease Activity Score in 28 joints (DAS28) were mostly used.
We found several reviews on the topic of bDMARD dose reduction. A Cochrane review was published in 2014 by van Herwaarden et al. that focused on down-titration and discontinuation of TNFi therapy [7]. However, its results were based on searches performed in September 2013. Because many new studies and full texts have been published since then, an update is needed. Some reviews have chosen to focus on dose reduction of both biological and synthetic DMARDs; examples include the recent reviews of Kuijper et al. and Schett et al. and a narrative review by Fautrel et al. [6, 11, 12]. Other reviews, such as those by Navarro-Millan et al., Yoshida et al., and Galvao et al. [10, 13, 14], only focus on bDMARD discontinuation.
The terminology used in the studies varies considerably. Therefore, in Table 2 we propose definitions of several terms that we will use in this review to describe concepts of interest.
1. What Are the Mechanisms Behind the Possibility of bDMARD Dose Reduction in RA Patients?
Most bDMARDs are believed to work though the achievement of a certain drug level in the blood that remains above the minimal effective drug concentration during the whole interval between two administrations [61]. The dose needed to obtain such a trough drug level differs between patients due to variations in the volume of distribution and the half-life of the drug. Furthermore, the minimal effective drug concentration varies significantly between patients. Therefore, each patient has their own dose–response curve [6].
Several dose–response patterns might be possible (Fig. 1). While some patients have an “average” dose–response curve, other patients will have a curve that is shifted to the left (good clinical response on a lower dose) or shifted to the right (good response only on a higher dose). Also, it is conceivable that some patients have a partial response to the drug or do not respond to the medication at all. The latter patients are doing well irrespective of the drug, possibly due to the placebo effect (in RCTs), regression to the mean, or concomitant medication.

Possible dose–response patterns for bDMARD treatment in RA patients (figure adapted from Fautrel et al. [6])
Conceptually, based on the possible response patterns, patients with a flat dose–response curve can discontinue the bDMARD, as the clinical effect is unrelated to treatment. For patients with an S-shaped dose–response curve, tapering is possible until the minimal effective concentration (the concentration below which disease activity increases) is reached. Patients with a partial response should be switched to another drug and patients with a dose–response curve shifted to the right would need a higher than standard dose. However, administering a higher dose is not a realistic option for bDMARDs, as the authorized dose of these drugs is based on maximal effect at the group level. So, the chance of response is low, and is in fact much lower than the chance of response after switching to another bDMARD. Also, this higher dosing will result in lower cost-effectiveness and increased risk of side effects [5, 6].
2. In Which Patients and When Should We Consider Dose Reduction?
For clinical practice, it is important to know which patients are eligible for dose reduction. Logically, dose reduction is only applicable in patients in whom the treatment goal is reached and treatment would normally remain unchanged. These are RA patients who have LDA or remission on treatment with a bDMARD.
Most of the studies included patients who showed sustained LDA or remission for ≥6 months. This period of 6 months seems reasonable, but this is based on expert opinion rather than evidence [6, 9]. It could be argued that dose reduction should only be performed in patients in clinical remission and not in patients with a low disease activity state. However, in a recent systematic review (mentioned in the section addressing question 4), neither DAS28-ESR nor DAS28-CRP at baseline demonstrated high predictive value for successful dose reduction or discontinuation of a bDMARD. Although deep remission is very nice to achieve, a less stringent goal of remission or low disease activity is a reasonable choice for many patients because (1) the patient-acceptable symptom state of RA disease activity is around a DAS28 of 3.2, (2) a subset of patients have a favorable prognosis with regard to joint damage, and thus do not need more intensive treatment, and (3) remission is not achievable in a subset of patients.
So, when the optimal effect of a bDMARD has been attained, it is possible to investigate whether this effect can be maintained with a lower dose of the drug. However, it is important to check that the bDMARD is not needed for any other condition such as Crohn’s disease or psoriasis. Also, it is also important to address the order in which the tapering of medications should occur. Many patients use not only a bDMARD but also oral glucocorticoids and one or more sDMARDs. According to the EULAR recommendations, oral glucocorticoids should be tapered first, bDMARDs next, and sDMARDs last [9]. This recommendation is based on the safety and cost-effectiveness of each drug.
In conclusion, all RA patients with sustained (e.g., ≥6 months) LDA or remission, who do not need the bDMARD for any other condition, and who do not use high doses of steroids can be considered for bDMARD dose reduction.
3. What is the Best Dose Reduction Strategy?
There are several possible strategies for dose reduction of bDMARDs in RA patients. Many studies have investigated the possibility of direct discontinuation of the drug when a patient is in a low disease activity state. This is also called withdrawal, a “treatment holiday,” or, when remission is maintained without any medication, drug-free remission (DFR); see also Table 2. Another option is a fixed dose reduction, for example halving the dose. The last and perhaps most sophisticated strategy is to taper the dose of the bDMARD step by step until disease flare or discontinuation of the medication. These last two strategies (fixed dose reduction or disease-activity-guided dose optimization) may be realized by either reducing the dose or increasing the interval between doses (spacing). Increasing the interval is the most practical approach for drugs administered through prefilled syringes, whereas dose reduction might be preferable for intravenous medication, as this is pharmacologically more efficient when a minimal effective trough concentration must be obtained for a drug with first-order pharmacokinetics [6]. It should be noted, however, that in RA treatment the overarching strategy is characterized by tight control, so this should be incorporated into any dose-reduction strategy [62].
Based on most of the studies and reviews, it is evident that direct discontinuation of a bDMARD ultimately leads to a disease flare in many or even most patients [13, 17, 26, 28, 29]. At the group level, this strategy is therefore probably inferior to continuation of the bDMARD with respect to disease control, although no studies have investigated a strategy in which direct discontinuation was combined with restarting under tight control. However, direct discontinuation is feasible for at least a relevant subset of patients, which makes it interesting to identify these patients beforehand (see question 4).
Fixed dose reduction and disease-activity-guided dose optimization have often been found to be noninferior to continuation of the drug [7, 17, 22, 24,25,26,27, 63]. These strategies should therefore be considered in daily practice, as suggested by the EULAR and ACR in current guidelines [8, 9]. One strategy for disease-activity-guided dose optimization is to attempt tapering only once (as in the DRESS study [25]). Another option is to taper again after remission has been re-achieved (as in the STRASS study [22]). As it seems that patient dose–response curves are relatively stable over the short term, repeated tapering attempts are probably not favorable. This may be why the spacing arm in the STRASS study has a slightly higher mean DAS28 value than the maintenance arm. It may, however, be reasonable to expect (although this should be investigated) that another tapering attempt could be considered after a longer period, for example 1 or 2 years.
There is a discrepancy between the results of blinded fixed dose reduction of etanercept and open-label disease-activity-guided dose tapering: having the dose was shown to be just as effective as full-dose continuation (and thus feasible in nearly 100% of patients), while open-label tapering was not feasible in 30–40% of patients. An explanation for this may be that doubling the interval is not exactly the same as halving the dose. Another, more likely, explanation might be the nocebo and attribution effects that are introduced when dose reduction is not blinded. Patients might perceive dose reduction as being inferior and may feel worse as a result (nocebo), or unrelated events may be falsely attributed to the dose reduction (causal attribution) [6]. There are currently no known interventions for countering these effects of nocebo and false causal attribution, so open-label dose reduction strategies will probably underperform in clinical practice compared to what is biologically and pharmacologically possible.
To summarize the findings, open-label disease-activity-guided dose optimization seems to be the best strategy in clinical practice, although this probably underperforms compared to blinded dose halving as done in RCTs. It may be best to perform one attempt at tapering and thereafter maintain the lowest effective dose that was found, as multiple tapering attempts can result in higher disease activity. Fixed dose halving is a good alternative, but disease activity should be monitored, and of course the benefits are less compared to tapering until stop. Direct stopping can be attempted, but the relapse risk is much higher, and no studies have shown noninferiority of a stop strategy with restart in case of flaring compared to bDMARD continuation.
4. What Proportion of the Patients Can Be Stopped or Tapered, and Can We Predict Successful Dose Reduction Using Patient or Treatment Characteristics?
Although the percentage of patients who can successfully stop or taper varies considerably between studies, and depends on the flare criteria used (see question 6), many more patients can taper than can discontinue. For direct bDMARD discontinuation, the relapse risk after one year lies between 45% and 88% [6]. For fixed bDMARD dose reduction, these numbers are much lower—around 40% in the PRESERVE trial, 50% in the DOSERA trial, and 34% in the ALLOW study [17, 26, 27]. Two reviews conclude that halving the dose of etanercept and rituximab is as effective as continuing with the full dose [7, 63].
For tapering strategies, the relapse rate should be interpreted differently, since tapering is continued until a patient flares (in order to find the optimal dose). In the DRESS study, the occurrence of short-lived flares was 73% in the tapering arm versus 23% in the continuation arm. However, there was no difference in persistent flares (longer than 3 months): 12% versus 10% in the tapering and continuation arms, respectively. The STRASS trial found comparable relapse rates: 77% (tapering) and 47% (continuation), although noninferiority could not be established due to lower than projected inclusion rates [22, 25].
The flare rate is thus lower for bDMARD fixed dose reduction versus bDMARD discontinuation. Open-label disease-activity-guided dose optimization leads to a high risk of short-lived flare versus continuation but comparable long-term disease control. Finally, fixed dose reduction seems as effective for two bDMARDs. These quantitative chances of successful dose reduction or discontinuation can be communicated to patients, and following shared decision-making (SDM), dose reduction can be attempted.
The chance of a successful dose reduction may differ between patient groups, depending on the patient or treatment characteristics. Therefore, many studies have also investigated possible predictors of success. Prediction of successful dose reduction or discontinuation of a bDMARD would provide several advantages. In patients who cannot use a lower dose, flares can be prevented by not tapering at all. For patients who are able to directly stop their bDMARD, accurate prediction would save time and medication since the dose-tapering phase can be skipped.
Regarding disease duration, a review by Kavanaugh reports that withdrawal appears possible for a subset of patients, especially those with early disease [64]. However, their conclusion is not consistent with a more recent review by Kuijper et al. in which the flare rate in studies including early RA patients was not consistently lower than that in patients with established RA [11].
Regarding the disease activity state before dose reduction, almost all studies use the DAS28 definition of LDA or remission when deciding upon patient inclusion [65]. Intuitively, it might seem logical that patients in remission have a higher chance of successful dose reduction compared to patients with low disease activity. However, in the RETRO trial, satisfying the ACR/EULAR Boolean remission criteria was not associated with a lower risk of relapse [6, 19]. Also, in the DRESS study, baseline disease activity was not a predictor of successful tapering [6, 25]. Therefore, all patients with LDA or in remission can be offered dose reduction with an equal chance of success.
Several dose-reduction studies have investigated various biomarkers for predicting successful tapering of bDMARDs. Some narrative reviews have demonstrated that it remains challenging to identify those patients who can taper their bDMARD without risking a flare [12, 66, 67]. In addition, the review of Schett et al. concludes that anti-citrullinated protein antibody (ACPA) negativity and the presence of “deep” remission such as absence of ultrasound synovitis and/or normal serum markers of inflammation are associated with greater chances of achieving drug-free remission [12].
A recent systematic review on this topic included 16 studies with a predefined tapering protocol and identified 64 and 52 different biomarkers for successful discontinuation and dose reduction, respectively. Among all the biomarkers investigated in more than one study, only three biomarkers were identified as predictive in two studies: a higher adalimumab trough level to predict successful dose reduction and a lower Sharp/van der Heijde erosion score and a shorter symptom duration at the start of a bDMARD to predict successful discontinuation [68]. The strength of this evidence was limited, since the latter two biomarkers (erosion score and symptom duration) showed a statistically significant but not strong association, and the first biomarker (adalimumab trough level) is questionable considering the extensive multiple testing performed in one study [69] and the disputed results of another study [70, 71]. Also, new data from the STRASS study could not confirm any predictive value of adalimumab level [72]. In contrast to Schett et al., ACPA was not found to be a predictor in this systematic review, and ultrasound and several serum markers were only studied once. Some studies have been published recently on the Multi-biomarker Disease Activity (MBDA) score as a predictor of successful tapering, but they report conflicting results [73,74,75,76].
Thus, biomarker-based prediction is not ready for clinical practice yet. Assessment of subclinical inflammation by laboratory or imaging testing may provide a useful tool to determine a patient’s risk of flare, but these biomarkers need to be validated first in other cohorts with a predefined tapering protocol before they can be considered to be predictive.
The type of bDMARD used might also be an effect modifier for successful dose reduction. Although some bDMARDs have been more extensively investigated than others, there do not appear to be any large differences in the effects of dose reduction. This may be due to the fact that for all bDMARDs, treatment using the authorized dose leads to overtreatment for at least a proportion of patients, since this dose is almost always chosen to be the highest effective dose at the group level. Some differences do seem to exist. For example, in the DREAM study with tocilizumab, relapse occurred quite rapidly [47].
Rituximab (RTX) is a rather different type of bDMARD. It is administered at intervals of at least 6 months due to the long B-cell depletion effect. The authorized RTX dosing for RA is also clearly much higher than needed. A recent systematic review revealed that half the authorized dose (1 × 1000 mg) is as effective as the full dose (2 × 1000 mg). This low dose is now widely used in clinical practice [77]. Several case studies and one case series suggest the possibility that a much lower dose of rituximab might be effective in the treatment of RA patients [78,79,80,81]. The effectiveness of these ultralow doses should be investigated further. Note that retreatment with RTX can be given on demand, but this results in repeated flaring and suboptimal disease control compared to fixed retreatment schedules or tight control treatment [82], as this approach essentially mimics repeated dose reduction attempts. So, while lower dosing can and should be used, in our opinion, retreatment should preferably be carried out either with a fixed interval or under strict tight control.
Regarding sDMARD use, Kavanaugh et al. suggest that patients who are MTX-naïve and receive an induction regimen of MTX with a TNF inhibitor may be better suited to dose reduction than those who do not respond to MTX sufficiently, improve upon the addition of a TNF blocker, and then are withdrawn from the bDMARD [64]. This seems logical, as response in these patients probably depends on MTX rather than the bDMARD. In the review by Kuijper et al., no relationship was observed between the use of a concomitant sDMARD and time to flare [11]. However, no information was reported on the order in which bDMARD and sDMARDs treatment was given before tapering. Therefore, no clear conclusion can be drawn on the effect of a concomitant DMARD treatment based on these reviews.
5. What Are the Effects of Dose Reduction on Function, Quality Of Life, Adverse Events, and Radiographic Damage?
Since fixed dose reduction and tapering of bDMARDs seem feasible in a large proportion of RA patients, and discontinuation for a smaller group, it is important to address the effects that are found on other important clinical outcomes such as function, quality of life, adverse events, and progression of joint damage.
Function (measured with the HAQ-DI) was found to be worse after discontinuation in the PRESERVE study, but not in two other RCTs, the OPTIMA and ADMIRE [17, 18, 28]. The ENCOURAGE study showed that fewer patients had HAQ <0.5 after discontinuation [21]. In the ALLOW study, physical function was slightly worse after withdrawal of abatacept, but this improved after reinstating treatment [15]. Function was found to be comparable to continuation after fixed dose reduction and tapering [17, 22, 25]. In the STRASS study, a small difference in quality of life remained at the end of the study [22].
The reduction of (dose-dependent) adverse events is one of the reasons to consider dose reduction of bDMARDs. Although several studies have monitored adverse events, few have found significant differences between dose reduction and continuation [17, 18, 22, 25, 26, 28, 49]. This might be due to the fact that none of these studies were powered to detect differences in side effects, and clinical trials in general have a limited follow-up time. Also, tapering studies usually include patients who have been using the bDMARD for quite some time, thus selecting the patients who are less prone to adverse effects (healthy survivor bias). However, Raffeiner et al. did find fewer infections in the half-dose etanercept group compared to the full-dose group [24].
Several studies have assessed the effect of bDMARD dose reduction on radiographic structural damage progression. In the PRESERVE trial, discontinuation of etanercept led to increased joint damage. However, progression in the dose-halving group was similar to that in the continuation group [17]. These findings are in line with other studies which found that dose reduction/tapering did not lead to significant radiographic damage progression [22, 24, 34, 35, 54, 55]. In the DRESS study, a minimal increase in radiographic progression was found in the tapering group, but no patients had an outcome of relevant joint damage progression [25]. Kuijper et al. conclude in their systematic review that there are limited data on radiographic damage but that the current evidence shows that progression remains limited after treatment de-escalation [11].
In conclusion, discontinuation results in somewhat worse function and more joint damage. Fixed dose reduction and tapering does not seem to result in deterioration in these parameters. A reduction in adverse events has not been unequivocally shown, although this seems plausible, as bDMARD-induced infections have been shown to be dose-related [4].
6. Which Flare Criterion is Best to Use When Deciding Whether to Restart/Re-escalate Treatment, and How Often Should the Patient Be Monitored?
In the included studies, several different criteria for flares were used, although they were mostly based on the DAS28. The OMERACT working group performed a validation study of the DAS28-based RA flare criteria. They concluded that an increase in DAS28 >1.2, or >0.6 if DAS28 ≥3.2, appears to be the most discriminating and valid based on a set of predefined validation criteria [83]. It is therefore advisable to use this flare criterion in clinical practice. In addition, the OMERACT RA Flare group is developing a patient-reported flare questionnaire that could also be used in the future [84], especially in health care systems where travel distances are much higher than generally encountered in Western Europe. Other flare criteria could be used as well, but they may be either too sensitive or too specific, resulting in worse patient outcomes or conversely unjustified treatment re-escalation.
Since dose reduction may lead to a flare in (a proportion of) the patients, it is very important to closely monitor patients who are tapering their bDMARDs. When a flare occurs, the dose should be increased again to the lowest effective dose. Based on the methods of several trials, an interval of no more than 3 months appears necessary, with an extra consultation when patients experience a worsening of their symptoms [22, 24, 25].
7. Is It Effective and Safe To Restart Treatment?
When considering discontinuation or tapering until stop, it is essential to know whether restarting the bDMARD or intensifying treatment will be effective and safe. Regarding effectiveness, most patients are able to regain LDA or remission again after restarting the bDMARD treatment. Percentages of between 80% and 100% are described [85]. Also, most studies show that restarting a bDMARD after withdrawal is well tolerated and not associated with more adverse events or higher immunogenicity [15, 25, 35, 38, 44, 49, 55]. Data from tight control studies also support this notion, as the mean DAS28 for example in the DRESS study is similar for continuation and dose reduction after 18 months, while switching to other bDMARDs was rare [25]. Therefore, based on the current evidence, it seems that restarting bDMARDs after discontinuation is effective and safe.
It has been suggested in the literature that tapering of bDMARDs may lead to the formation of anti-drug antibodies (ADAbs), which could then result in worse outcomes after restarting treatment. However, there does not seem any evidence supporting this statement [85, 86]. It is probable that the amount of “free” antibodies that is measured depends on the dose of the antigen (the drug). When administering a high dose, most of the ADAbs will be bound to the drug. When administering a low dose, more of the ADAbs will be unbound and are thus measureable in the blood. This does not automatically imply that the formation of these antibodies is increased, or that the presence of the ADAbs leads to a lower effect or side effects.
8. What is the Cost-Effectiveness of Dose Reduction?
Next to infection risk and patient burden due to regular self-injection, costs are one of the main reasons to look into dose reduction of bDMARDs after LDA or remission is reached. Surprisingly, not many of the studies that address this topic report a cost analysis of their strategy. This may be because the majority of the studies are funded by pharmaceutical companies, so there is perhaps a limited interest in demonstrating that dose reduction is cost-effective. While it seems logical that tapering a bDMARD will result in a substantial cost saving, the question is whether these savings outweigh the costs induced by increased monitoring, patient education, an increase in flares, and a subsequent deterioration in quality of life (as reflected in QALYs).
Only three of the RCTs included in this review describe a cost-effectiveness analysis: the STRASS and DRESS studies, which both investigated disease-activity-guided tapering of bDMARDs until discontinuation, and the PRESERVE study [22, 25, 87,88,89]. The STRASS study found that spacing resulted in a smaller gain in QALYs during the study period of 18 months compared to continuation. They calculated that 53,417 euros were saved per QALY lost. The authors indicate that it depends on the willingness to accept whether this is cost-effective [22]. In the DRESS study, the mean QALY loss was −0.02 in the tapering arm compared to the continuation arm, and the dose optimization strategy resulted in savings of approximately 8000 euros per patient per year. The savings per QALY lost were 390,493 euros. When the minimal QALY loss was adjusted to account for the upper limit of what society is willing to pay or accept in the Netherlands, the net savings were still high [25]. For the PRESERVE study, a Markov model was devised that incorporated data from the trial and extrapolated to 10 years follow-up, allowing a dose increase in the case of a flare and dose reduction in the case of remission according to tight control. Overall, the fixed dose halving strategy seemed most advantageous, mainly because half-dose etanercept showed a similar effectiveness to full-dose [89].
Three of the nonrandomized studies that we found reported costs [37, 44, 52]. In an uncontrolled study of infliximab tapering by van der Maas et al., a mean reduction of 3474 euros per patient was found [37]. In a strategy study by Inui et al., patients discontinued etanercept when disease activity was low and restarted when a flare occurred. In the 5 patients who maintained low disease activity without restarting etanercept, the savings were found to be approximately 35% [44]. Murphy et al. reported a cost saving of 600,000 euros after 2 years in their cohort of 79 patients (45 RA, 10 psoriatic arthritis, and 24 ankylosing spondylitis) that reduced the dose of etanercept or adalimumab [52]. That meant a saving of 3800 euros per patient per year—comparable to the savings found by van der Maas et al.
Overall, disease-activity-guided dose optimization results in large cost savings per patient per year and no or a small loss in QALYs. Cost-effectiveness estimates are, however, very sensitive to either no or very small changes in quality of life, so the precise cost-effectivenesses of different strategies remain to be established, although results seem very encouraging.
9. How Can Dose Optimization Best Be Implemented in Clinical Practice?
An often forgotten aspect of new treatment strategies is their implementation in clinical practice. Although several studies have shown the additional value of bDMARD dose reduction, and it has been incorporated into international recommendations [8, 9], this does not automatically mean that clinicians will act on it [90, 91].
Several studies have investigated the current use of a lower-than-standard dose of bDMARDs in routine clinical practice. A systematic review into dose escalation and dose reduction of bDMARDs in clinical practice found that, for etanercept, 13.2% of patients used a lower-than-registered dose. For adalimumab and infliximab, this was 8.9% and 25%, respectively [92]. In a retrospective cohort of RA patients using Medicare claims (n = 26,510), approximately 10–20% of patients who initiated and adhered to etanercept and adalimumab for ≥12 months subsequently received reduced-dose therapy for an 12 additional months and beyond [93]. In the Ninja cohort (n = 1037), 7.4% of patients stopped bDMARD treatment due to remission [94] and 40% of patients in a tertiary hospital in Spain (n = 96) used a lower-than-registered dose while remaining at a low disease activity or in remission [95]. These data show that in routine clinical practice, outside of trials, bDMARD dose reduction is still relatively rare, and it is often implemented for reasons other than dose optimization (e.g., side effects), and the mean percentage of patients on a lower-than-registered dose probably lies somewhere between 10% and 25%.
Many factors can impede the use of new insights in clinical practice, such as barriers related to the innovation itself (e.g., complexity, relative advantage), the individual health care provider or patient (e.g., knowledge, attitude, skills, self-efficacy), incentives and resources (time, funding), or the organizational context (work climate, structures) [90, 96]. For dose reduction, it is conceivable that rheumatologists are not aware of the possibility of dose reduction (knowledge), do not agree with the evidence (attitude), or simply do not have the time or tools/protocols to adhere to the guidelines (practical barriers). The same holds true for patients. Since it is still difficult to predict successful dose reduction, tapering comes with a risk of (short-term) disease flare which makes the decision to taper very dependent on patient preference. Gaining insight into barriers and facilitators for patients and physicians could facilitate implementation.
Recently, a pilot study aiming at the implementation of tight control and bDMARD dose optimization was published [97]. A multicomponent strategy consisting of education, protocol development, and treatment advice was employed to improve the use of these principles in a tertiary hospital with two rheumatologists. The results showed an increase in DAS measurements and a large decrease in bDMARD use, while mean disease activity levels remained unchanged. Larger, preferably controlled, studies are necessary to assess the effectivenesses of implementation strategies.
10. What is the Patient Perspective on bDMARD Dose Reduction?
Since dose reduction of a bDMARD comes with an increased risk of short-lived disease flare, the decision to start tapering is also dependent on the preference of each individual patient. The physician can inform, educate, and motivate the patient based on the current evidence on dose reduction, but the final decision should be SDM-based. It is therefore important to investigate what patients’ cognitions and emotions are regarding bDMARD dose reduction.
Three qualitative studies into the patient perspective on bDMARD dose reduction were identified [98,99,100]. These studies all found that dose reduction is associated with both positive and negative perceived aspects for patients. Positive aspects include the reduced risk of adverse events, reduced frequency of injections, and contributing to savings in the healthcare budget. Examples of negative aspects are the risk of a flare, a delay in access to previous doses, and fear of a loss of efficacy after restarting treatment.
While these qualitative studies all explore factors that are important to patients when considering dose reduction of a bDMARD, the preferences of individual patients will differ largely. However, the current evidence on dose reduction and the need to reduce medication costs urge that tapering in RA patients who reach a stable LDA or remission on bDMARD treatment should be discussed in shared decision-making. In clinical practice, a balance must be found between patient concerns and the responsibility of hospitals and rheumatologists to contribute to savings in the healthcare budget.
Communication methods could help physicians in their daily work regarding bDMARD dose reduction. Patient expectations could be modified by informing them as early as possible about the option of dose reduction, for example at the start of their bDMARD treatment. Also, motivational interviewing or positive framing can be used in conversations about dose reduction with individual patients.
Discussion
Based on the current evidence for this subject, we conclude that bDMARD dose reduction can be considered in all RA patients who have stably reached their treatment goals (e.g., ≥6 months LDA or remission) on treatment with a bDMARD. The best strategy seems to be disease-activity-guided dose tapering with fixed dose reduction as an alternative, since the risk of relapse was found to be highest for direct bDMARD discontinuation, and discontinuation results in worse physical functioning and more joint damage. Although bDMARD tapering seems to be (very) cost-effective, a reduction in adverse events after dose reduction is yet to be clearly demonstrated.
When tapering the bDMARD treatment of a patient, disease activity should be monitored closely, for example with a consultation every 3 months and extra consultations when necessary. The validated flare criterion (∆DAS28 >1.2 or >0.6 if DAS28 ≥3.2) can be used to identify patients who have lost response due to the tapering. When a patient flares, the dose should be increased to the lowest effective dose. Current evidence shows that restarting bDMARD treatment is effective and safe. Unfortunately, no clear predictors of successful tapering have been identified so far. The evidence for bDMARD dose reduction and rising healthcare costs urge that dose reduction should be considered and attempted for eligible patients. However, patient values and preferences should be respected and a balance may be found using SDM.
This study has some limitations, as our searches for relevant articles were systematic but the data extraction and writing were performed in a narrative manner. Also, we did not perform a quality assessment of the included articles, and no formal meta-analyses were done. However, this review does provide a complete overview of the most important studies that have been performed on bDMARD dose reduction, and the questions that we address here could be of interest to a large group of clinicians involved in the treatment of RA patients.
Several new trends are visible regarding bDMARD dose reduction, such as the introduction of biosimilars, which will change the cost-effectiveness ratio for tapering [101]. Also, evidence on bDMARD dose reduction for other diagnoses in rheumatology is emerging, for example in relation to psoriatic arthritis and ankylosing spondylitis [102]. Furthermore, new methods of research are gaining interest, such as noninferiority trials (investigating whether a new strategy or treatment is no worse than the old one) and modeling studies (using existing data to answer new research questions, thus saving costs and limiting the burden on patients) [103, 104]. Lastly, it is clear that most of the research done on the topic of dose reduction is “hard science,” and studies of the “soft science” associated with dose reduction (e.g., investigations of SDM and implementation) are lagging behind. Future research should focus not only on achieving a better understanding of the effects of dose reduction on important clinical outcomes but also on the perspectives of the patients and physicians as well as the implementation of this new treatment principle.
Conclusions
In conclusion, a lot of research has been done on the topic of bDMARD dose reduction in RA. The best dose-reduction strategies seem to be disease-activity-guided dose optimization and fixed dose reduction. The evidence for bDMARD dose reduction and rising healthcare costs urge that dose reduction should be considered for and attempted in RA patients who have reached a stable state of LDA or remission. However, patient values and preferences should be respected, and a balance may be found using SDM.
References
Nam JL, Ramiro S, Gaujoux-Viala C, et al. Efficacy of biological disease-modifying antirheumatic drugs: a systematic literature review informing the 2013 update of the EULAR recommendations for the management of rheumatoid arthritis. Ann Rheum Dis. 2014;73(3):516–28.
Zorginstituut Nederland. Medicijnkosten.nl website. http://www.medicijnkosten.nl.
Singh JA, Wells GA, Christensen R, et al. Adverse effects of biologics: a network meta-analysis and cochrane overview. Cochrane Database Syst Rev. 2011;(2):CD008794.
Singh JA, Cameron C, Noorbaloochi S, et al. Risk of serious infection in biological treatment of patients with rheumatoid arthritis: a systematic review and meta-analysis. Lancet. 2015;386(9990):258–65.
Bongartz T, Sutton AJ, Sweeting MJ, Buchan I, Matteson EL, Montori V. Anti-TNF antibody therapy in rheumatoid arthritis and the risk of serious infections and malignancies: systematic review and meta-analysis of rare harmful effects in randomized controlled trials. JAMA. 2006;295(19):2275–85.
Fautrel B, den Broeder AA. De-intensifying treatment in established rheumatoid arthritis (RA): why, how, when and in whom can DMARDs be tapered? Best Pract Res Clin Rheumatol. 2015;29(4–5):550–65.
van Herwaarden N, den Broeder AA, Jacobs W, et al. Down-titration and discontinuation strategies of tumor necrosis factor-blocking agents for rheumatoid arthritis in patients with low disease activity. Cochrane Database Syst Rev. 2014;9:CD010455.
Singh JA, Saag KG, Bridges SL Jr, et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Care Res (Hoboken). 2016;68(1):1–25.
Smolen JS, Landewe R, Breedveld FC, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update. Ann Rheum Dis. 2014;73(3):492–509.
Yoshida K, Sung YK, Kavanaugh A, et al. Biologic discontinuation studies: a systematic review of methods. Ann Rheum Dis. 2014;73(3):595–9.
Kuijper TM, Lamers-Karnebeek FB, Jacobs JW, Hazes JM, Luime JJ. Flare rate in patients with rheumatoid arthritis in low disease activity or remission when tapering or stopping synthetic or biologic DMARD: a systematic review. J Rheumatol. 2015;42(11):2012–22.
Schett G, Emery P, Tanaka Y, et al. Tapering biologic and conventional DMARD therapy in rheumatoid arthritis: current evidence and future directions. Ann Rheum Dis. 2016;75(8):1428–37.
Galvao TF, Zimmermann IR, da Mota LM, Silva MT, Pereira MG. Withdrawal of biologic agents in rheumatoid arthritis: a systematic review and meta-analysis. Clin Rheumatol. 2016;35(7):1659–68.
Navarro-Millán I, Sattui SE, Curtis JR. Systematic review of tumor necrosis factor inhibitor discontinuation studies in rheumatoid arthritis. Clin Ther. 2013;35(11):1850–61.
Kaine J, Gladstein G, Strusberg I, et al. Evaluation of abatacept administered subcutaneously in adults with active rheumatoid arthritis: impact of withdrawal and reintroduction on immunogenicity, efficacy and safety (phase IIIb ALLOW study). Ann Rheum Dis. 2012;71(1):38–44.
Batticciotto A, Varisco V, Antivalle M, et al. AB0297 dose reduction in patients with rheumatoid arthritis responding to the standard rituximab regimen. Ann Rheum Dis. 2013;72(Suppl 3):A877.
Smolen JS, Nash P, Durez P, et al. Maintenance, reduction, or withdrawal of etanercept after treatment with etanercept and methotrexate in patients with moderate rheumatoid arthritis (PRESERVE): a randomised controlled trial. Lancet. 2013;381(9870):918–29.
Smolen JS, Emery P, Fleischmann R, et al. Adjustment of therapy in rheumatoid arthritis on the basis of achievement of stable low disease activity with adalimumab plus methotrexate or methotrexate alone: the randomised controlled OPTIMA trial. Lancet. 2014;383(9914):321–32.
Haschka J, Englbrecht M, Hueber AJ, et al. Relapse rates in patients with rheumatoid arthritis in stable remission tapering or stopping antirheumatic therapy: interim results from the prospective randomised controlled RETRO study. Ann Rheum Dis. 2016;75(1):45–51.
Mariette X, Rouanet S, Sibilia J, et al. Evaluation of low-dose rituximab for the retreatment of patients with active rheumatoid arthritis: a non-inferiority randomised controlled trial. Ann Rheum Dis. 2014;73(8):1508–14.
Yamanaka H, Nagaoka S, Lee SK, et al. Discontinuation of etanercept after achievement of sustained remission in patients with rheumatoid arthritis who initially had moderate disease activity-results from the ENCOURAGE study, a prospective, international, multicenter randomized study. Mod Rheumatol. 2016;26(5):651–61.
Fautrel B, Pham T, Alfaiate T, et al. Step-down strategy of spacing TNF-blocker injections for established rheumatoid arthritis in remission: results of the multicentre non-inferiority randomised open-label controlled trial (STRASS: spacing of TNF-blocker injections in Rheumatoid ArthritiS Study). Ann Rheum Dis. 2016;75(1):59–67.
Galloway JB, Kingsley G, Ma M, et al. SAT0150 optimising treatment with TNF inhibitors in rheumatoid arthritis with different dose tapering strategies: the Opttira trial. Ann Rheum Dis. 2015;74(Suppl 2):706.
Raffeiner B, Botsios C, Ometto F, et al. Effects of half dose etanercept (25 mg once a week) on clinical remission and radiographic progression in patients with rheumatoid arthritis in clinical remission achieved with standard dose. Clin Exp Rheumatol. 2015;33(1):63–8.
van Herwaarden N, van der Maas A, Minten MJ, et al. Disease activity guided dose reduction and withdrawal of adalimumab or etanercept compared with usual care in rheumatoid arthritis: open label, randomised controlled, non-inferiority trial. BMJ. 2015;350:h1389.
van Vollenhoven RF, Ostergaard M, Leirisalo-Repo M, et al. Full dose, reduced dose or discontinuation of etanercept in rheumatoid arthritis. Ann Rheum Dis. 2016;75(1):52–8.
Westhovens R, Robles M, Ximenes AC, et al. Maintenance of remission following 2 years of standard treatment then dose reduction with abatacept in patients with early rheumatoid arthritis and poor prognosis. Ann Rheum Dis. 2015;74(3):564–8.
Chatzidionysiou K, Turesson C, Teleman A, et al. A multicentre, randomised, controlled, open-label pilot study on the feasibility of discontinuation of adalimumab in established patients with rheumatoid arthritis in stable clinical remission. RMD Open. 2016;2(1):e000133.
Ghiti MM, Vonkeman HE, Ten Klooster PM, et al. Stopping tumor necrosis factor inhibitor treatment in patients with established rheumatoid arthritis in remission or with stable low disease activity: a pragmatic multicenter, open-label randomized controlled trial. Arthritis Rheumatol. 2016;68(8):1810–7.
den Broeder AA, Creemers MC, van Gestel AM, van Riel PL. Dose titration using the Disease Activity Score (DAS28) in rheumatoid arthritis patients treated with anti-TNF-alpha. Rheumatology (Oxford). 2002;41(6):638–42.
Quinn MA, Conaghan PG, O’Connor PJ, et al. Very early treatment with infliximab in addition to methotrexate in early, poor-prognosis rheumatoid arthritis reduces magnetic resonance imaging evidence of synovitis and damage, with sustained benefit after infliximab withdrawal: results from a twelve-month randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2005;52(1):27–35.
Brocq O, Millasseau E, Albert C, et al. Effect of discontinuing TNFalpha antagonist therapy in patients with remission of rheumatoid arthritis. Jt Bone Spine. 2009;76(4):350–5.
Saleem B, Keen H, Goeb V, et al. Patients with RA in remission on TNF blockers: when and in whom can TNF blocker therapy be stopped? Ann Rheum Dis. 2010;69(9):1636–42.
Tanaka Y, Takeuchi T, Mimori T, et al. Discontinuation of infliximab after attaining low disease activity in patients with rheumatoid arthritis: RRR (remission induction by remicade in RA) study. Ann Rheum Dis. 2010;69(7):1286–91.
van den Broek M, Klarenbeek NB, Dirven L, et al. Discontinuation of infliximab and potential predictors of persistent low disease activity in patients with early rheumatoid arthritis and disease activity score-steered therapy: subanalysis of the BeSt study. Ann Rheum Dis. 2011;70(8):1389–94.
Harigai M, Takeuchi T, Tanaka Y, Matsubara T, Yamanaka H, Miyasaka N. Discontinuation of adalimumab treatment in rheumatoid arthritis patients after achieving low disease activity. Mod Rheumatol. 2012;22(6):814–22.
van der Maas A, Kievit W, van den Bemt BJ, van den Hoogen FH, van Riel PL, den Broeder AA. Down-titration and discontinuation of infliximab in rheumatoid arthritis patients with stable low disease activity and stable treatment: an observational cohort study. Ann Rheum Dis. 2012;71(11):1849–54.
Aguilar-Lozano L, Castillo-Ortiz JD, Vargas-Serafin C, et al. Sustained clinical remission and rate of relapse after tocilizumab withdrawal in patients with rheumatoid arthritis. J Rheumatol. 2013;40(7):1069–73.
Detert J, Bastian H, Listing J, et al. Induction therapy with adalimumab plus methotrexate for 24 weeks followed by methotrexate monotherapy up to week 48 versus methotrexate therapy alone for DMARD-naive patients with early rheumatoid arthritis: HIT HARD, an investigator-initiated study. Ann Rheum Dis. 2013;72(6):844–50.
Hørslev-Petersen K, Hetland ML, Junker P, et al. THU0212 improved remission rates acquired by adding adalimumab to methotrexate and intraarticular glucocorticoid cannot be maintained after withdrawal of adalimumab. a 2-year investigator initiated randomised, controlled study on early rheumatoid arthritis. Ann Rheum Dis. 2013;72(Suppl 3):A236.
Kurasawa T, Nagasawa H, Kishimoto M, Amano K, Takeuchi T, Kameda H. Addition of another disease-modifying anti-rheumatic drug to methotrexate reduces the flare rate within 2 years after infliximab discontinuation in patients with rheumatoid arthritis: an open, randomized, controlled trial. Mod Rheumatol. 2014;24(4):561–6.
Rakieh C, Saleem B, Takase K, et al. Long term outcomes of stopping tumour necrosis factor inhibitors (TNFI) in patients with established rheumatoid arthritis (RA) who are in sustained remission: is it worth the risk? Ann Rheum Dis. 2013;72(Suppl 3):A208–9.
Huizinga TW, Conaghan PG, Martin-Mola E, et al. Clinical and radiographic outcomes at 2 years and the effect of tocilizumab discontinuation following sustained remission in the second and third year of the ACT-RAY study. Ann Rheum Dis. 2015;74(1):35–43.
Inui K, Koike T, Tada M, et al. Restart for sustaining remission of rheumatoid arthritis in use of etanercept: Resume study. Ann Rheum Dis. 2014;73(Suppl 2):936–7.
Iwamoto T, Ikeda K, Hosokawa J, et al. Prediction of relapse after discontinuation of biologic agents by ultrasonographic assessment in patients with rheumatoid arthritis in clinical remission: high predictive values of total gray-scale and power Doppler scores that represent residual synovial inflammation before discontinuation. Arthritis Care Res (Hoboken). 2014;66(10):1576–81.
Maneiro JR, Perez-Pampin E, Salgado E, Carmona L, Gomez-Reino JJ. Observational study of optimization of biologic therapies in rheumatoid arthritis: a single-centre experience. Rheumatol Int. 2014;34(8):1059–63.
Nishimoto N, Amano K, Hirabayashi Y, et al. Drug free REmission/low disease activity after cessation of tocilizumab (Actemra) Monotherapy (DREAM) study. Mod Rheumatol. 2014;24(1):17–25.
van Herwaarden N, Herfkens-Hol S, van der Maas A, et al. Dose reduction of tocilizumab in rheumatoid arthritis patients with low disease activity. Clin Exp Rheumatol. 2014;32(3):390–4.
Atsumi T, Yamamoto K, Tekeuchi T, et al. Clinical benefit of 1-year certolizumab pegol treatment in MTX-naïve, early rheumatoid arthritis patients is maintained after discontinuation up to 1 year (abstract). Arthritis Rheumatol. 2015;67(Suppl 10).
Emery P, Burmester GR, Bykerk VP, et al. Evaluating drug-free remission with abatacept in early rheumatoid arthritis: results from the phase 3b, multicentre, randomised, active-controlled AVERT study of 24 months, with a 12-month, double-blind treatment period. Ann Rheum Dis. 2015;74(1):19–26.
Marks JL, Holroyd CR, Dimitrov BD, et al. Does combined clinical and ultrasound assessment allow selection of individuals with rheumatoid arthritis for sustained reduction of anti-tumor necrosis factor therapy? Arthritis Care Res (Hoboken). 2015;67(6):746–53.
Murphy CL, Awan S, Sullivan MO, et al. Major cost savings associated with biologic dose reduction in patients with inflammatory arthritis. Ir Med J. 2015;108(1):19–21.
Naredo E, Valor L, De la Torre I, et al. Predictive value of Doppler ultrasound-detected synovitis in relation to failed tapering of biologic therapy in patients with rheumatoid arthritis. Rheumatology (Oxford). 2015;54(8):1408–14.
Takeuchi T, Matsubara T, Ohta S, et al. Biologic-free remission of established rheumatoid arthritis after discontinuation of abatacept: a prospective, multicentre, observational study in Japan. Rheumatology (Oxford). 2015;54(4):683–91.
Tanaka Y, Hirata S, Kubo S, et al. Discontinuation of adalimumab after achieving remission in patients with established rheumatoid arthritis: 1-year outcome of the HONOR study. Ann Rheum Dis. 2015;74(2):389–95.
Alivernini S, Peluso G, Fedele AL, Tolusso B, Gremese E, Ferraccioli G. Tapering and discontinuation of TNF-alpha blockers without disease relapse using ultrasonography as a tool to identify patients with rheumatoid arthritis in clinical and histological remission. Arthritis Res Ther. 2016;3(18):39.
Bouman C, Tweehuysen L, Haverkort D, et al. [AB0342] Study on abatacept and tocilizumab attenuation (SONATA) in rheumatoid arthritis patients: a retrospective, explorative cohort study. Ann Rheum Dis. 2016;75(Suppl 2):1019.
Heimans L, Akdemir G, Boer KV, et al. Two-year results of disease activity score (DAS)-remission-steered treatment strategies aiming at drug-free remission in early arthritis patients (the IMPROVED study). Arthritis Res Ther. 2016;21(18):23.
Wiland P, Dudler J, Veale D, et al. The effect of reduced or withdrawn etanercept-methotrexate therapy on patient-reported outcomes in patients with early rheumatoid arthritis. J Rheumatol. 2016;43(7):1268–77.
Bingham CO III, Pohl C, Woodworth TG, et al. Developing a standardized definition for disease “flare” in rheumatoid arthritis (OMERACT 9 Special Interest Group). J Rheumatol. 2009;36(10):2335–41.
Nestorov I. Clinical pharmacokinetics of TNF antagonists: how do they differ? Semin Arthritis Rheum. 2005;34(5 Suppl 1):12–8.
Schipper LG, van Hulst LT, Grol R, van Riel PL, Hulscher ME, Fransen J. Meta-analysis of tight control strategies in rheumatoid arthritis: protocolized treatment has additional value with respect to the clinical outcome. Rheumatology (Oxford). 2010;49(11):2154–64.
Bredemeier M, de Oliveira FK, Rocha CM. Low- versus high-dose rituximab for rheumatoid arthritis: a systematic review and meta-analysis. Arthritis Care Res (Hoboken). 2014;66(2):228–35.
Kavanaugh A, Smolen JS. The when and how of biologic agent withdrawal in rheumatoid arthritis: learning from large randomised controlled trials. Clin Exp Rheumatol. 2013;31(4 Suppl 78):S19–21.
Prevoo ML, van’t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995;38(1):44–8.
Nagy G, van Vollenhoven RF. Sustained biologic-free and drug-free remission in rheumatoid arthritis, where are we now? Arthritis Res Ther. 2015;3(17):181.
van den Broek M, Visser K, Allaart CF, Huizinga TW. Personalized medicine: predicting responses to therapy in patients with RA. Curr Opin Pharmacol. 2013;13(3):463–9.
Tweehuysen L, van den Ende CH, Beeren FM, Been EM, van den Hoogen FH, den Broeder AA. Little evidence for usefulness of biomarkers for predicting successful dose reduction or discontinuation of a biologic agent in rheumatoid arthritis: a systematic review. Arthritis Rheumatol. 2017;69(2):301–308.
van Herwaarden N, Bouman CA, van der Maas A, et al. Adalimumab and etanercept serum (anti)drug levels are not predictive for successful dose reduction or discontinuation in rheumatoid arthritis. Ann Rheum Dis. 2015;74(12):2260–1.
Bouman C, den Broeder AA. Letter in response to the article of Chen et al: ‘Drug trough levels predict therapeutic responses to dose reduction of adalimumab for rheumatoid arthritis patients during 24 weeks follow-up’. Rheumatology (Oxford). 2016.
Chen DY, Chen YM, Hsieh TY, et al. Drug trough levels predict therapeutic responses to dose reduction of adalimumab for rheumatoid arthritis patients during 24 weeks of follow-up. Rheumatology (Oxford). 2016;55(1):143–8.
Marotte H, Rinauda M, Paul S, Fautrel B. No prediction of relapse by TNF blocker concentrations or detection of antibodies against anti-TNF: data from STRASS study. Ann Rheum Dis. 2016;75:495.
Bouman C, van der Maas A, van Herwaarden N, Sasso EH, van den Hoogen FH, den Broeder AA. The multi-biomarker disease activity score in a TNF inhibitor tapering study in rheumatoid arthritis patients: predictive value for successful tapering, flaring and radiographic progression [abstract]. Arthritis Rheumatol. 2015;67(Suppl 10).
Hirata S, Wang X, Hwang CC, et al. Predicting flare and sustained clinical remission after adalimumab withdrawal using the multi-biomarker disease activity (MBDA) score [abstract]. Arthritis Rheumatol. 2016;68(Suppl 10).
Lamers-Karnebeek FB, Ghiti Moghadam M., Vonkeman HE, et al. Multi-biomarker disease actvity score as a predictor of flare in patients with rheumatoid arthritis who stop TNF-alpha-inhibitor therapy [abstract]. Arthritis Rheumatol. 2015;67(Suppl 10).
Rech J, Hueber AJ, Englbrecht M, et al. Prediction of disease relapses by multi-biomarker disease test activity in rheumatoid arthritis patients tapering DMARD treatment [abstract]. Arthritis Rheumatol. 2015;67(Suppl 10).
Bredemeier M, Campos GG, de Oliveira FK. Updated systematic review and meta-analysis of randomized controlled trials comparing low- versus high-dose rituximab for rheumatoid arthritis. Clin Rheumatol. 2015;34(10):1801–5.
Bruzzese V, Pepe J. Unexpected and persistent depletion of B lymphocytes CD20 following a minimum dose of anti-CD20 antibody (Rituximab). Reumatismo. 2009;61(4):306–8.
Bruzzese V. Therapeutic effectiveness of minimal doses of rituximab in a patient with rheumatoid arthritis. Int J Immunopathol Pharmacol. 2011;24(1):265–7.
Bruzzese V, Marrese C, Hassan C, Andriani A, Zullo A. Prompt efficacy of very low-dose rituximab on monoclonal B lymphocytosis in a rheumatoid arthritis patient. Int J Rheum Dis. 2013;16(6):764–5.
Shenoy P, Bavaliya M. Efficacy of very low dose (100 mg) rituximab in active rheumatoid arthritis despite combination DMARD-single center, prospective, observational study (abstract). Arthritis Rheumatol. 2015;29:67.
Emery P, Mease PJ, Rubbert-Roth A, et al. Retreatment with rituximab based on a treatment-to-target approach provides better disease control than treatment as needed in patients with rheumatoid arthritis: a retrospective pooled analysis. Rheumatology (Oxford). 2011;50(12):2223–32.
van der Maas A, Lie E, Christensen R, et al. Construct and criterion validity of several proposed DAS28-based rheumatoid arthritis flare criteria: an OMERACT cohort validation study. Ann Rheum Dis. 2013;72(11):1800–5.
Bartlett SJ, Bykerk VP, Cooksey R, et al. Feasibility and domain validation of rheumatoid arthritis (RA) flare core domain set: report of the OMERACT 2014 RA Flare Group Plenary. J Rheumatol. 2015;42(11):2185–9.
Chan CK, Holroyd CR, Mason A, Zarroug J, Edwards CJ. Are there dangers in biologic dose reduction strategies? Autoimmun Rev. 2016;15(7):742–6.
Vincent FB, Morand EF, Murphy K, Mackay F, Mariette X, Marcelli C. Antidrug antibodies (ADAb) to tumour necrosis factor (TNF)-specific neutralising agents in chronic inflammatory diseases: a real issue, a clinical perspective. Ann Rheum Dis. 2013;72(2):165–78.
Kievit W, van HN, van den Hoogen FH, et al. Disease activity-guided dose optimisation of adalimumab and etanercept is a cost-effective strategy compared with non-tapering tight control rheumatoid arthritis care: analyses of the DRESS study. Ann Rheum Dis. 2016;75:1939–44.
Vanier A, Tubach F, Alfaiate T, Mariette X, Fautrel B. Step-down strategy of spacing TNF-blockers injections for established rheumatoid arthritis in remission: a cost-utility analysis based on the STRASS trial. Ann Rheum Dis. 2015;74(Suppl 2):178.
Kobelt G. Treating to target with etanercept in rheumatoid arthritis: cost-effectiveness of dose reductions when remission is achieved. Value Health. 2014;17(5):537–44.
Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999;282(15):1458–65.
Harrold LR, Harrington JT, Curtis JR, et al. Prescribing practices in a US cohort of rheumatoid arthritis patients before and after publication of the American College of Rheumatology treatment recommendations. Arthritis Rheum. 2012;64(3):630–8.
Ferriols-Lisart R, Ferriols-Lisart F. Dose modifications of anti-TNF drugs in rheumatoid arthritis patients under real-world settings: a systematic review. Rheumatol Int. 2015;35(7):1193–210.
Zhang J, Xie F, Delzell E, et al. Impact of biologic agents with and without concomitant methotrexate and at reduced doses in older rheumatoid arthritis patients. Arthritis Care Res (Hoboken). 2015;67(5):624–32.
Yoshida K, Kishimoto M, Radner H, et al. Low rates of biologic-free clinical disease activity index remission maintenance after biologic disease-modifying anti-rheumatic drug discontinuation while in remission in a Japanese multicentre rheumatoid arthritis registry. Rheumatology (Oxford). 2016;55(2):286–90.
Rosario V, Hernández MV, Inciarte-Mundo J, et al. A significant number of patients with rheumatoid arthritis receive low doses of biological agents in clinical practice. Ann Rheum Dis. 2013;71(Suppl 3):666.
Flottorp SA, Oxman AD, Krause J, et al. A checklist for identifying determinants of practice: a systematic review and synthesis of frameworks and taxonomies of factors that prevent or enable improvements in healthcare professional practice. Implement Sci. 2013;8:35.
Lesuis N, Verhoef LM, Nieboer LM, et al. Implementation of protocolized tight control and biological dose optimization in daily clinical practice: results of a pilot study. Scand J Rheumatol. 2016;27:1–4.
Markusse IM, Akdemir G, Huizinga TW, Allaart CF. Drug-free holiday in patients with rheumatoid arthritis: a qualitative study to explore patients’ opinion. Clin Rheumatol. 2014;33(8):1155–9.
Verhoef LM, Selten EM, van den Hoogen F, den Broeder AA, Hulscher ME. Perceived barriers and facilitators for bDMARD dose optimization: a qualitative study into RA patients’ perspectives. Ann Rheum Dis. 2016;75:1272.
Wallis D, Holroyd CR, Sonpal K, Zarroug J, Adams J, Edwards CJ. Dose reduction of biological therapies in rheumatoid arthritis—the patient’s perspective. Ann Rheum Dis. 2016;75:1313.
Dorner T, Kay J. Biosimilars in rheumatology: current perspectives and lessons learnt. Nat Rev Rheumatol. 2015;11(12):713–24.
Olivieri I, D’Angelo S, Padula A, Leccese P, Nigro A, Palazzi C. Can we reduce the dosage of biologics in spondyloarthritis? Autoimmun Rev. 2013;12(7):691–3.
Landewe R, Van Der Heijde D. New concepts of clinical trials in rheumatoid arthritis: a boom of noninferiority trials. Curr Opin Rheumatol. 2016;28(3):316–22.
Welsing PM, Severens JL, Hartman M, van Gestel AM, van Riel PL, Laan RF. The initial validation of a Markov model for the economic evaluation of (new) treatments for rheumatoid arthritis. Pharmacoeconomics. 2006;24(10):1011–20.
Acknowledgements
No funding or sponsorship was received for this study or the publication of this article. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published.
Disclosures
Lise Verhoef, Lieke Tweehuysen, Marlies Hulscher, Bruno Fautrel, and Alfons den Broeder have nothing to disclose.
Compliance with Ethics Guidelines
This article is based on previously conducted studies, and does not involve any new studies of human or animal subjects performed by any of the authors.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/2D87F060266F1CFA.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Verhoef, L.M., Tweehuysen, L., Hulscher, M.E. et al. bDMARD Dose Reduction in Rheumatoid Arthritis: A Narrative Review with Systematic Literature Search. Rheumatol Ther 4, 1–24 (2017). https://doi.org/10.1007/s40744-017-0055-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40744-017-0055-5