
Abstract
Background
Critically ill pediatric patients are considered at high risk for medication errors. Although much research focuses on the actual errors, equally important are medication errors that, although intercepted, carried the potential for an adverse drug event. The aim of this study was to determine the occurrence of prescribing errors and potential adverse drug events (pADEs) in a local pediatric intensive and critical care unit (PICU) in Hong Kong. Our secondary objective was to determine the type of error, nature of medication involved and the time of error occurrence.
Methods
We conducted a prospective observational chart review among patients in a pediatric intensive and high dependency unit between January 16, 2015 and April 20, 2015. Medical charts for each patient were reviewed for the occurrence of a prescribing error or pADE. Each pADE was assessed for the type of error, the classification of agent involved, clinical severity of the error, and the time the error occurred.
Results
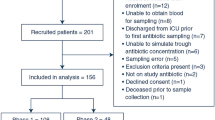
Forty-one patients with a mean age of 3.2 years were included in our study. Of these patients, 19 (46.3%) experienced at least one pADE. We identified 131 pADEs, 129 of which were prescribing errors conferring a rate of 6.8 errors per affected patient or 3.1 errors per patient admitted to the PICU. The most common error found in the study was incorrect dose calculation (48.1%), with intravenous fluids (41.7%), cardiovascular agents (15.0%), and anti-infectives (12.5%) the most common agents involved with an error. The majority of the pADEs in our study were either clinically serious (33.1%) or significant (44.9%) in nature. Nearly one in every four errors required monitoring and/or intervention to prevent harm, and almost all (96.9%) of the prescribing errors were intercepted before reaching the patient.
Conclusion
This study highlights incorrect dose calculation as the most common prescribing error in a pediatric critical care setting. Intravenous fluids, cardiovascular agents, and anti-infectives were the classes of medication most commonly involved with a pADE. Due to the high-risk nature of medications used and the critical condition of these patients, more than three-quarters of pADEs were considered to be clinically serious or significant in causing patient harm.

Similar content being viewed by others


References
National Coordinating Council for Medication Error Reporting and Prevention (NCCMERP). About Medication Errors. [Internet]. [cited July 21 2015]. Available from: http://www.nccmerp.org/aboutMedErrors.html.
Martinez-Anton A, Sanchez J, Casanueva L. Impact of an intervention to reduce prescribing errors in a pediatric intensive care unit. Intensive Care Med. 2012;38:1532–8.
Skapik J, Pronovost P, Miller M, Thompson D, Wu A. Pediatric safety incidents from an intensive care reporting system. J Patient Saf. 2009;5(2):95–101.
Institute of Medicine Committee on Quality Health Care in America. To err is human: building a safer health system. Report of the Institute of Medicine. In: Kohn L, Corrigan J, Donaldson M, editors. National Academy Press; 2000.
Bates D, Cullen D, Laird N, Petersen L, et al. Incidence of adverse drug events and potential adverse drug events. JAMA. 1995;274(1):29–34.
Bates D, Boyle D, Vander Vliet M, Schenider J, Leape L. Relationship between medication errors and adverse drug events. J Gen Intern Med. 1995;10:199–205.
Kunac D, Kennedy J, Austin N, Reith D. Incidence, preventability, and impact of adverse drug events (ADEs) and potential ADEs in hospitalized children in New Zealand. Pediatr Drugs. 2009;11(2):153–60.
Kaushal R, Bates D, Landrigan C, McKenna K, Clapp M, Federico F, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285(16):2114–20.
Burmester M, Dionne R, Thiagarajan R, Laussen P. Interventions to reduce medication errors in a paediatric cardiac intensive care unit. Intensive Care Med. 2008;34:1083–90.
Alagha H, Badary O, Ibrahim H, Sabri N. Reducing prescribing errors in the paediatric intensive care unit: an experience from Egypt. Acta Paediatr. 2011;100:e169–74.
Cimino M, Kirsjhbaum M, Brodsky L, Shaha S. Assessing medication prescribing errors in pediatric intensive care units. Pediatr Crit Care Med. 2004;5(2):124–32.
Wong I, Ghaleb M, Franklin B, Barber N. Incidence and nature of dosing errors in paediatric medications. Drug Saf. 2004;27(9):661–70.
Wong I, Wong L, Cranswick E. Minimising medication errors in children. Arch Dis Child. 2009;94:161–4.
Glanzmann C, Frey B, Meier C, Vonbach P. Analysis of medication prescribing errors in critically ill children. Eur J Pediatr. 2015;174:1347–55.
Folli H, Poole R, Benitz W, Russo J. Medication error prevention by clinical pharmacists in two children’s hospitals. Pediatrics. 1987;79:718–22.
Yang C, Veltri M, Anton B, Yaster M, Berkowitz I. Food and Drug Administration approval for medications used in the pediatric intensive care unit: a continuing conundrum. Pediatr Crit Care Med. 2011;12(5):e195–9.
ISMP List of High Alert Medications in Acute Care Settings [Internet]. http://www.ismp.org/Tools/institutionalhighAlert.asp: Institute for Safe Medication Practices [cited 2017 Jan 21].
WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC classification and DDD assignment 2013. World Health Organization; 2012.
Holdsworth M, Fichtl R, Behta M, Raisch D, Mendez-Rico E, Adams A, et al. Incidence and impact of adverse drug events in pediatric inpatients. Arch Pediatr Adolesc Med. 2003;157:60–5.
Overhage J, Lukes A. Practical, reliable, comprehensive method for characterizing pharmacists’ clinical activities. Am J Health Syst. 1999;56(23):2444–50.
Buckley M, Erstad B, Kopp B, Theodorou A, Priestley G. Direct observation approach for detecting medication errors and adverse drug events in a pediatric intensive care unit. Pediatr Crit Care Med. 2007;8(2):145–52.
Franke H, Woods D, Holl J. High-alert medications in the pediatric intensive care unit. Pediatr Crit Care Med. 2009;10(1):85–90.
Kaushal R, Bates D, Abramson E, Soukup J, Goldmann D. Unit-based clinical pharmacists’ prevention of serious medication errors in pediatric inpatients. Am J Health Syst. 2008;65:1254–60.
Committe on Drugs and Committee on Hospital Care. Prevention of medication errors in the pediatric inpatient setting. Pediatrics. 2003;112(2):431–6.
Costello J, Torowicz D, Yeh T. Effects of a pharmacist-led pediatric medication safety team on medication error-reporting. Am J Health Syst. 2007;64:1422–6.
National Patient Safety Agency. Safety in doses: medication safety incidents in the NHS. London: Patient Safety Observatory report; 2009.
Rashed A, Wilton L, Lo C, Kwong B, Leung S, Wong I. Epidemiology and potential risk factors of drug-related problems in Hong Kong paediatric wards. Br J Clin Pharmacol. 2013;77(5):873–9.
Agency for Healthcare Research and Quality [Internet].: U.S. Department of Health and Human Services [cited Feb. 7 2007]. Available from: https://healthit.ahrq.gov/health-it-tools-and-resources/workflow-assessment-health-it-toolkit/all-workflow-tools/fmea-analysis.
Spath P. Using failure mode and effects analysis to improve patient safety. AORN. 2003;78(1):16–37.
Lago P, Bizzarri G, Scalzotto F, Parpaiola A, Amigoni A, Putoto G, et al. Use of FMEA analysis to reduce risk of errors in prescribing and administering drugs in paediatric wards: a quality improvement report. BMJ Open. 2012;2(e001249):1–9.
Rinke M, Bundy D, Velasquez C, Rao S, Zerhouni Y, Lobner K, et al. Interventions to reduce pediatric medication errors: a systematic review. Pediatrics. 2014;134:338–60.
Dickinson C, Wagner D, Shaw B, Owens T, Paslp D, Niedner M. A systematic approach to improving medication safety in a pediatric intensive care unit. Crit Care Nurs Q. 2012;35(1):15–26.
Booth R, Sturgess E, Taberner-Stokes A, Peters M. Zero tolerance prescribing: a strategy to reduce prescribing errors on the paediatric intensive care unit. Intensive Care Med. 2012;38:1858–67.
Krupicka M, Bratton S, Sonnenthal K, Goldstein B. Impact of a pediatric clinical pharmacist in the pediatric intensive care unit. Crit Care Med. 2002;30(4):919–21.
Wong I, Ghaleb M, Franklin B, Barber N. Ways to reduce drug dose calculation errors in children. J Health Serv Res Policy. 2010;15(Suppl 1):68–70.
Hilmas E, Sowan A, Gaffoor M, Vaidya V. Implementation and evaluation of a comprehensive system to deliver pediatric continuous infusion medications with standardized concentrations. Am J Health Syst Pharm. 2010;67:58–69.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the research institution’s Investigational Review Board. The authors declare no financial assistance was received for conducting the study or preparation of the manuscript.
Conflict of interest
Authors C. Ewig, H.M. Cheung, K.H. Kam, H.L. Wong, and C. Knoderer declare they have no conflict of interests with the design, implementation and results of this study or with the contents of the manuscript.
Rights and permissions
About this article

Cite this article
Ewig, C.L.Y., Cheung, H.M., Kam, K.H. et al. Occurrence of Potential Adverse Drug Events from Prescribing Errors in a Pediatric Intensive and High Dependency Unit in Hong Kong: An Observational Study. Pediatr Drugs 19, 347–355 (2017). https://doi.org/10.1007/s40272-017-0222-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40272-017-0222-8