
Abstract
Introduction
Hidradenitis suppurativa (HS) is a chronic, autoinflammatory skin disease associated with many comorbidities. One biologic (adalimumab) is approved for HS. This study assessed the sociodemographic characteristics, comorbidities, treatment patterns, healthcare resource utilization (HCRU) and associated costs of patients with HS following biologic approval.
Methods
This non-interventional, retrospective cohort study involved adult (≥ 18 years) and adolescent (12–17 years) patients diagnosed with HS in the United States (US) using Optum’s de-identified Clinformatics® Data Mart Database during the period 1 January 2016 to 31 December 2018.
Results
Of 42,843 identified patients, 10,909 met the incident HS patient criteria (10,230 adults, 628 adolescents, 51 patients aged <12 years). Patients were mostly diagnosed by a general practitioner/pediatrician (adults: 41.6%; adolescents: 39.6%) or dermatologist (adults: 22.1%; adolescents: 30.6%). Commonly reported Charlson comorbidities at pre-index in adult patients were diabetes without complications (20.4%), chronic pulmonary disease (16.4%) and diabetes with complications (9.0%), and the most frequent Elixhauser comorbidities were uncomplicated hypertension (38.3%), obesity (22.5%), uncomplicated diabetes (19.0%) and depression (17.4%). The burden of comorbidities generally increased over time after diagnosis in both adults and adolescents. HS-related surgical procedures were uncommon in the 2-years post-index period: an incision and drainage procedure was reported in 7.6% of adults and 6.4% of adolescents. Patients were predominantly treated with both topical and systemic antibiotic treatments (adults: 25.0% and 65.1%, respectively; adolescents: 41.7% and 74.5%, respectively). Biologic prescription was higher in adults than adolescents (3.5% vs. 1.8%). Total healthcare costs for adult and adolescent patients in the 2-years post-index period were US$42,143 and US$16,057, respectively, with outpatient costs accounting for the majority of these costs (US$20,980 and US$8408, respectively).
Conclusion
In adult and adolescent patients with HS, comorbidity burden continues to increase after diagnosis. All-cause and HS-specific HCRU and costs are high in adults and adolescents with HS. These findings support the need for a multidisciplinary comprehensive care strategy for patients with HS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In adult and adolescent patients with hidradenitis suppurativa (HS), the comorbidity burden continues to increase over time. |
Healthcare resource use and costs are high in adults and adolescents with HS. |
Patients with HS may require comprehensive care strategies involving a multidisciplinary team of physicians to improve health while reducing health care expenditures. |
1 Introduction
Hidradenitis suppurativa (HS) is a chronic, autoinflammatory, recurrent, debilitating skin disease characterized by painful, deep lesions predominantly located in the axillary, inguinal and anogenital regions [1,2,3]. The prevalence of HS is generally in the range of 0.1–1%, however estimates vary based on geographical location and data methodology [4,5,6,7,8]. Furthermore, current registry data have suggested an increasing incidence in the United States (US) [6, 9, 10].
A multidisciplinary approach is often used in the management of HS and can comprise surgical intervention, topical and systemic agents, and lifestyle modification. The most commonly used pharmacological agents for HS include topical or systemic antibiotics, intralesional or systemic corticosteroids, and procedural interventions such as deroofing and excision. Biologics began to emerge several years ago as important treatment options for moderate to severe HS [11] and have likely changed treatment patterns. However, to date, adalimumab, a tumor necrosis factor-α blocker, is the only biologic therapy approved for HS, but phase II and III trials are currently underway to assess the efficacy and safety of other biologics in patients with moderate to severe HS [12].
Unsurprisingly, HS is associated with a significant burden of disease, and patients with HS also report various comorbid conditions, including metabolic, inflammatory/autoimmune, and psychiatric disorders [3, 13,14,15,16]. Furthermore, HS has a substantial impact on patients' quality of life and can result in stigmatization and a significant negative impact on work life [17,18,19,20]. HS has also been reported to be detrimental to the mental well-being of patients: anxiety, depression, and suicidality are more common in patients with HS than in most other dermatological conditions [21, 22].
Treatment patterns of HS in the period since biologic therapy was approved (i.e., 2015) may have changed. The costs associated with HS management prior to biologic treatment were reported as significant [15, 23]. Marvel et al. reported that the average total cost of care among patients with HS in the US ranged between US$2662 (Medicaid) and US$4428 (Commercial/Medicare) per patient per year prior to the approval of adalimumab [23]. To address this knowledge gap, this study assessed the sociodemographic characteristics, treatment patterns, healthcare resource utilization (HCRU) and associated costs of patients with HS, in the time following the approval of a biologic for the management of HS by using a large dataset from a US administrative claims database.
2 Methods
2.1 Objectives of the Analysis
The primary objective of this study was to evaluate the demographic, clinical and socioeconomic characteristics of patients with HS over a 3-year period in the time period following approval of biologic treatment in the US. Secondary objectives were to (1) analyze the medical treatment patterns of patients with HS; (2) analyze the HS-specific interventional procedure patterns of patients with HS; and (3) characterize HS-specific and all-cause HCRU and associated costs of patients with HS.
2.2 Study Design and Patients
This was a descriptive, non-interventional, retrospective cohort study involving adult (aged ≥ 18 years) and adolescent (aged 12–17 years) patients diagnosed with HS in the US using Optum’s de-identified Clinformatics® Data Mart Database (CDM), which is a commercial and Medicare Advantage health claims dataset. Optum’s CDM database includes claims for both medical and prescription coverage of patients to enable users to evaluate the complete healthcare experience. The population is weighted to include a commercial health plan population and Medicare Advantage population that is geographically diverse, spanning 50 states in the US.
Patients with at least one HS diagnosis (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code 705.83 and Tenth Revision [ICD-10-CM] code L73.2) during the identification period from 1 January 2016 to 31 December 2018 were included. The index date for this analysis was the date of the first claim of a HS diagnosis within this identification period. The population was further refined by including only patients with ≥ 1 year of continuous enrollment (CE) before the index date (referred to as the pre-index period) and ≥ 2 years of CE after the index date (referred to as the post-index period).
Analysis was conducted only on patients with HS who were considered incident, defined as patients without a confirmed HS diagnosis in the 1-year (and up to 5 years) pre-index period. This was done to ensure that patients included were relatively newly diagnosed.
2.3 Data Reporting and Statistical Analysis
In all analyses, missing data were treated as a separate category and were described using frequency counts and percentages.
Data are reported for incident HS patients only and are presented for the three following time periods: 1-year pre-index period, 1-year post-index period, and 2-years post-index period (which is cumulative and includes both the first- and second-year post-index date). Data are presented separately for adult (≥ 18 years) and adolescent (≥ 12–17 years) patients. Additional exploratory analyses are presented for subgroups of patients prescribed biologics and patients not prescribed biologics.
HS-specific treatment, procedure and HCRU outcomes in the 1-year pre-index period were not captured, as accurately attributing these outcomes to HS disease was reliant on linking the event of interest to a HS diagnosis, which was not present in the pre-index period.
2.4 Ethical Considerations
Optum is a de-identified database, and no patient-level data were collected or stored.
2.5 Study Variables
Sociodemographic characteristics (see the Appendix in the electronic supplementary material [ESM]) were obtained on the index date or in the 1-year pre-index period.
Comorbidities, treatment, and procedure patterns, as well as HCRUs and associated costs, were measured during the 1-year pre-index period (excluding the index date), and 1- and 2-years post-index period (including the index date). Comorbidities were based on the presence of an associated ICD-9 or ICD-10 code within the assessed time frame, and included Charlson comorbidities [24, 25], Charlson Comorbidities Index (CCI), Elixhauser comorbidities [26], and Elixhauser Cormorbidities Index (ECI) [26]. Both the Charlson and Elixhauser indices do not adjust for age, therefore CCI and ECI are presented only for adult patients with HS. Other comorbidities were selected based on their previously reported association with HS [27,28,29] (see the Methods section of the ESM).
Medical treatment and procedures were captured over the same time periods as comorbidities, while HS-specific procedures were captured 1 and 2 years post-index and were indicated by a claim associated with a diagnosis of HS. HS-specific medications were identified as requiring a diagnosis of HS within 7 days before a drug claim. The time to the first HS-specific procedure or prescription following the index diagnosis (days) was determined. The HS-related medications and procedures are listed in the Methods section of the ESM.
HCRU and associated costs were estimated during the 1-year pre-index period (excluding the index date) and the 1- or 2-years post-index period (including the index date). All-cause and HS-specific HCRUs were assessed for all analyses: all-cause and HS-specific HCRUs including office visits (dermatologist visits and surgeon visits), other outpatient visits, emergency room (ER), and hospitalizations; healthcare costs comprising all-cause and HS-specific ER costs; all-cause and HS-specific inpatient costs; all-cause and HS-specific outpatient costs; all-cause and HS-specific medical costs (inpatient, outpatient and ER); all-cause and HS prescription drug costs; all-cause and HS-related total healthcare costs (medical cost and prescription drug cost). Physician specialty involved during a patient’s HS journey was reported for patients diagnosed by dermatologists, surgeons, ER, obstetricians and gynecologists (OBGYN), general practitioners (GPs), other specialists, and other healthcare providers (HCPs; i.e., dentist, physical therapist).
2.6 Data Analysis
The physician on the index HS claim for a patient in the study period was assigned as the index physician. In case of multiple physicians on the index date, the index physician was assigned based on a descending order of priority using the following criteria: (1) claim locations, which were identified as facility or non-facility claims with non-facility claims prioritized; (2) the location was further broken down and priority was in the following order: profession, outpatient facility and then ancillary services; and (3) if more than one physician specialty was selected based on the above criteria, the HCP specialty priority was as per the following hierarchy: dermatologist, surgeon, ER/hospital, GP/pediatrician, OBGYN, other specialists, and other HCPs.
3 Results
3.1 Patient Flow and Demographics
A total of 42,843 patients with at least one HS diagnosis during the identification period were identified from the Optum database (Fig. 1). Of these patients, 24,200 had 1-year of CE during the pre-index period and 13,269 had ≥ 2 years of CE post-index. Within this population, 10,909 patients met the criteria to be considered as being an incident HS patient, including 10,230 incident HS adults (≥ 18 years), 628 incident HS adolescents (≥ 12–17 years) and 51 patients < 12 years.

Patient flow. aA diagnosis of HS was captured using ICD-9-CM code 705.83 and ICD-10-CM code L73.2. bThe identification period was between 1 January 2016 and 31 December 2018. cA gap of ≤45 days was allowed. dThe index date for this analysis was considered as the date of the first claim of a diagnosis of HS within this identification period. HS hidradenitis suppurativa, ICD-9-CM International Classification of Diseases, Ninth Revision, Clinical Modification, ICD-10-CM International Classification of Diseases, Tenth Revision, Clinical Modification, N number of patients in each group
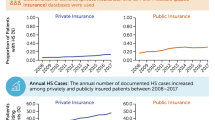
The mean age (standard deviation [SD]) of adult and adolescent patients was 47.1 (17.3) and 15.3 (1.5) years, respectively. The majority (70.7%) of patients included were female, irrespective of age. All adolescent patients and 68.7% of adult patients had commercial insurance, with 31.3% of adults being covered by Medicare (Table 1). Patients mostly received their diagnosis by a GP/pediatrician (adults, 41.6%; adolescents, 39.6%) or a dermatologist (adults, 22.1%; adolescents, 30.6%), and confirmed diagnoses were similar for 2016, 2017 and 2018 for adolescents but increased each year for adults (Table 1).
3.2 Comorbidities among Incident Hidradenitis Suppurativa (HS) Patients
The most commonly reported (defined as those occurring in ≥ 3% of the population within either the 1-year pre-index, 1-year post-index or 2-years post-index periods) Charlson comorbidities in adult patients were diabetes without complications, followed by chronic pulmonary disease and diabetes with complications (Table 2). These comorbidities, together with peripheral vascular disease and renal disease, increased over the 3 years. As expected, the frequencies of Charlson comorbidities were low in adolescents, except for chronic pulmonary disease (likely asthma rather than chronic obstructive pulmonary disease), being present in 8.3%, 8.9% and 10.7% of adolescents in the 1-year pre-index, 1-year post-index and 2-years post-index periods, respectively (Table 2).
In adult patients, the most commonly reported Elixhauser comorbidities were uncomplicated hypertension, obesity, uncomplicated diabetes, depression and chronic pulmonary disease, all of which increased over time (Table 3). In adolescent patients, the frequency of depression, obesity and chronic pulmonary disease was high in all time periods, with depression and obesity increasing over time (Table 3).
Of the selected comorbidities that were assessed based on their previously reported association with HS in the literature [27,28,29], anxiety disorder was common in both adult (Fig. 2a) and adolescent (Fig. 2b) patients in the 1-year pre-index, 1-year post-index and 2-years post-index periods. Acne vulgaris and acne (other) were prevalent in adolescent but not adult patients (Fig. 2). Within the adult population, obstructive sleep apnea, hyperglycemia, anemia, and substance abuse were all frequently reported (Fig. 2a). Overall, the burden of comorbidities increased substantially over time after diagnosis in both adults and adolescents, except for hyperglycemia in adolescents (Fig. 2).

Selected comorbidities of interest in incident adult and adolescent HS patients. aObstructive sleep apnea. Bar graphs demonstrating the most frequent (> 3% in any group) selected comorbidities of interest in incident adult (N = 10,230) (a) and adolescent (N = 628) (b) HS patients. HS hidradenitis suppurativa, N number of patients in each group, NAFLD nonalcoholic fatty liver disease, SpA spondyloarthropathies
3.3 Procedures and Treatments among Incident Adult and Adolescent HS Patients
Procedures and treatments among incident adult and adolescent HS patients in the 1-year post-index and 2-years post-index periods are presented in Table 4.
HS-related surgical procedures were relatively uncommon in the post-index periods; incision and drainage was the most frequently reported procedure, with similar levels observed between adult and adolescent patients (Table 4). Patients with HS were predominantly treated with both topical and systemic antibiotic treatments in the post-index periods; of interest, adolescents received topical and systemic antibiotics more than the adult population in both post-index periods (Table 4). The use of analgesics (including opioids) to treat HS-related pain was common in the post-index periods, and higher in adult than adolescent patients (Table 4).
Biologic treatment was uncommon in both adult and adolescent patients in the post-index periods. Biologic prescription was higher in adults and increased slightly between the 1- and 2-years post-index periods in both adults (2.6% vs. 3.5%) and adolescents (0.6% vs. 1.8%). Most biologic prescriptions were for adalimumab (91.0% [322/354] and 90.9% [10/11] for adult and adolescent patients in the 2-years post-index period, respectively), with the remainder of biologic prescriptions used being off-label for this indication.
3.4 HS-Related Healthcare Resource Utilization and Associated Costs among Incident Adult and Adolescent HS Patients
Both adults and adolescent patients with HS reported a high HCRU. The mean number of HCRU office and outpatient visits per patient were high for both adult and adolescent patients in all time periods, with a higher number of visits reported for adult patients (Table 5). For both adult and adolescent patients, most medical visits (both office and outpatient) occurred outside of dermatology and surgery specialties. HS-specific visits accounted for over 10% of all-cause office visits.
The total healthcare cost (total medical plus total prescription cost) for adult and adolescent patients in the 2-years post-index period was US$42,143 and US$16,057, respectively (Table 6). Outpatient costs accounted for most total medical costs for both adults and adolescent patients. HS-specific total healthcare costs accounted for 4–15% of overall total healthcare costs in adult and adolescent patients in the 1- and 2-years post-index periods (Table 6).
Of interest, all-cause dermatology office visits and HS-specific overall visits were higher for adolescents compared with adults (Table 5), and, in line with this, HS-specific total healthcare costs were slightly higher in adolescent patients (Table 6).
3.5 Biologics Versus Non-Biologics Subgroups
Differences in comorbidities, procedures, and treatments and HCRU was also investigated in patients with and without previous biologic exposure and are detailed in ESM Tables S1–S4 and ESM Figs. S1 and S2.
4 Discussion
This study provides real-world information on sociodemographic characteristics, treatment patterns, HCRU and associated costs of HS patients in a large dataset collected after the approval of biologic therapy for the treatment of HS during 2016–2018. The majority (69.2%) of incident patients with HS were of working age (between 18 and 59 years), which is relevant as HS impacts work participation and can lead to absenteeism, low work productivity, lower annual income and income growth, and a higher risk of leaving the workforce [19, 20, 30].
This study confirmed the high comorbidity burden in patients with HS, as reported elsewhere in the medical literature [23, 31, 32]. Psychosocial comorbidities, including depression, anxiety, loneliness, and low self-esteem, were commonly reported comorbidities in both adult and adolescent patients, in line with the well-established burden of HS on patients’ QoL [18, 33,34,35]. Adolescents also reported acne vulgaris as a common comorbidity [36]. As supported by the literature, adult patients in this study commonly reported several additional comorbidities including anemia [37], obstructive sleep apnea [38], substance abuse [39], hyperglycemia [40] and spondyloarthritis [41]. Increases in diagnosed associated comorbidities were seen for diabetes (with and without complications), chronic pulmonary disease, hypertension, renal disease, depression, and obesity. Whether early treatment or early identification of these patients at risk can improve their overall health outcomes is an important question that remains to be studied. Whether a HS diagnosis contributes to accelerated accumulation of comorbidities or helps to uncover existing ones, these patients would likely benefit from improved early care.
Even though this study was performed after biologic therapy was approved for HS in the US (2016–2018), this analysis showed that most patients are managed on topical therapies and systemic antibiotics. Indeed, the level of antibiotic use (systemic and topical) was higher in adolescents than adults, which might be because physicians are more reluctant to escalate treatment in the adolescent population. Few studies have been performed in real-world settings to assess the prescription of biologic therapies in patients with HS. One study conducted following the approval of biologics in Hungary observed that 15.5% of patients were treated with biologics (adalimumab: 15%; infliximab [off-label]: 0.5%); however, this study was conducted in a small population of patients (n = 200) [42]. A recent cross-sectional analysis of > 25,000 patients with HS in the US reported that 1.8% of these patients had been prescribed a biologic [43], which is in line with the findings of the current study where < 4% of patients had received a biologic.
Overall, patients made the most visits to other offices rather than to a dermatology office; this observation is supported by the baseline demographics data where patients mostly visited GPs/pediatricians rather than a dermatologist, and with a high number of HS-specific visits to physicians other than a dermatologist. This suggests a possible under-management of the disease, with patients being treated by non-specialist HCPs. Given the complexity of HS as a disease, treatment of HS by a non-dermatologist may result in a lack of effective medical treatment, misdiagnosis, or a delay in diagnosis. On the other hand, these patients had high comorbidity levels and were rapidly being diagnosed with further comorbidities, therefore good primary and secondary care are important for their care and management. However, the implementation of an evidence-based diagnosis and treatment management checklist for patients with HS in the primary care setting that is easy to use with clear criteria may reduce the delay in diagnosis and optimize treatment outcomes for these patients [44]. Furthermore, detailed treatment algorithms and consensus guidelines exist for HS to support HCPs in treating HS and to optimize HS treatment outcomes [45].
Focusing on HCRU, all-cause visits and healthcare costs were higher for adults, which aligns with the higher and accumulating comorbidity burden in adults, whereas adolescent patients recorded more HS-specific office visits and higher HS-specific healthcare costs. This finding may be because children have fewer concomitant medical problems and require other kinds of care less frequently. Outpatient medical costs represented a higher proportion of the economic burden in both adult and adolescent patients. This finding contrasts with previous reports published before the approval of biologics where the total cost of treating patients with HS was attributable to inpatient costs [15, 23], indicating a previous reliance on surgical procedures, which decreased considerably after the introduction of biologics as an alternative treatment option. However, further analyses with larger proportions of patients prescribed biologics than used in this study would be required to confirm such conclusions. Furthermore, differences in study design and patient populations should also be considered. A retrospective study determining the HCRU and costs for patients with atopic dermatitis in US adults using the Truven Health Marketscan Commercial Claims and Encounters database during 2013 found the adjusted total incremental annual costs were US$3302, with resource utilization and costs being higher in patients with more severe atopic dermatitis (US$4463) [46]. While not a direct comparison, the high costs and high frequencies of comorbidities with HS reported here would suggest that earlier diagnosis and treatment is likely to have a positive impact on the overall cost burden.
There are several limitations to this study. The study relies on data in administrative claims, which may be inaccurate or subject to human error, technical error, or missing data. Incident patients included in this population had to have ≥ 1 HS diagnosis, rather than ≥ 2 diagnoses, which would have increased reliability of the diagnosis [47]. It should also be noted that the data were based on the insured US population and did not include the entire US population (Medicaid population not included). Therefore, the study findings are not generalizable to the entire US population. In addition, the data included only fully adjudicated and paid claims and diagnosed conditions. The study did not consider the severity of HS as this was not recorded using claims data, and this could influence HCRU. There could also be ascertainment bias, as patients with HS now being cared for would be more likely to have other diagnoses uncovered. Lastly, this study does not include a control population of patients without HS, which would provide important insights on the incidence of comorbidities in the HS population.
5 Conclusions
This study provides real-world information and demonstrates that in adult and adolescent patients with HS, the overall comorbidity burden was high and continued to accumulate over the study period after the approval of biologic therapy for the treatment of HS. Furthermore, all-cause and HS-specific resource utilization and costs are high in both adults and adolescents with HS. Patients with HS may require comprehensive care strategies involving a multidisciplinary team of physicians to improve health while reducing health care expenditures.
References
Gonzaga TA, Endorf FW, Mohr WJ, Ahrenholz DH. Novel surgical approach for axillary hidradenitis suppurativa using a bilayer dermal regeneration template: a retrospective case study. J Burn Care Res. 2013;34(1):51–7.
Jemec GB. Clinical practice. Hidradenitis suppurativa. N Engl J Med. 2012;366(2):158–64.
Sabat R, Jemec GBE, Matusiak L, Kimball AB, Prens E, Wolk K. Hidradenitis suppurativa. Nat Rev Dis Primers. 2020;6(1):18.
Calao M, Wilson JL, Spelman L, Billot L, Rubel D, Watts AD, et al. Hidradenitis suppurativa (HS) prevalence, demographics and management pathways in Australia: a population-based cross-sectional study. PLoS ONE. 2018;13(7): e0200683.
Delany E, Gormley G, Hughes R, McCarthy S, Kirthi S, Markham T, et al. A cross-sectional epidemiological study of hidradenitis suppurativa in an Irish population (SHIP). J Eur Acad Dermatol Venereol. 2018;32(3):467–73.
Garg A, Lavian J, Lin G, Strunk A, Alloo A. Incidence of hidradenitis suppurativa in the United States: a sex- and age-adjusted population analysis. J Am Acad Dermatol. 2017;77(1):118–22.
Ingram JR, Jenkins-Jones S, Knipe DW, Morgan CLI, Cannings-John R, Piguet V. Population-based Clinical Practice Research Datalink study using algorithm modelling to identify the true burden of hidradenitis suppurativa. Br J Dermatol. 2018;178(4):917–24.
Phan K, Charlton O, Smith SD. Global prevalence of hidradenitis suppurativa and geographical variation—systematic review and meta-analysis. Biomed Dermatol. 2020;4:2. https://doi.org/10.1186/s41702-019-0052-0.
Sung S, Kimball AB. Counterpoint: analysis of patient claims data to determine the prevalence of hidradenitis suppurativa in the United States. J Am Acad Dermatol. 2013;69(5):818–9.
Vazquez BG, Alikhan A, Weaver AL, Wetter DA, Davis MD. Incidence of hidradenitis suppurativa and associated factors: a population-based study of Olmsted County, Minnesota. J Invest Dermatol. 2013;133(1):97–103.
Kimball AB, Okun MM, Williams DA, Gottlieb AB, Papp KA, Zouboulis CC, et al. Two phase 3 trials of adalimumab for hidradenitis suppurativa. N Engl J Med. 2016;375(5):422–34.
Aarts P, Dudink K, Vossen A, van Straalen KR, Ardon CB, Prens EP, et al. Clinical implementation of biologics and small molecules in the treatment of hidradenitis suppurativa. Drugs. 2021;81(12):1397–410.
Garg A, Malviya N, Strunk A, Wright S, Alavi A, Alhusayen R, et al. Comorbidity screening in hidradenitis suppurativa: evidence-based recommendations from the US and Canadian Hidradenitis Suppurativa Foundations. J Am Acad Dermatol. 2022;86(5):1092–101.
Hendricks AJ, Hsiao JL, Lowes MA, Shi VY. A comparison of international management guidelines for hidradenitis suppurativa. Dermatology. 2021;237(1):81–96.
Kirby JS, Miller JJ, Adams DR, Leslie D. Health care utilization patterns and costs for patients with hidradenitis suppurativa. JAMA Dermatol. 2014;150(9):937–44.
Jemec GB, Kimball AB. Hidradenitis suppurativa: epidemiology and scope of the problem. J Am Acad Dermatol. 2015;73(5 Suppl 1):S4-7.
Bouazzi D, McPhie ML, Kjærsgaard Andersen R, Alavi A, Jemec GBE. Hidradenitis suppurativa and perceived stigmatization in a diverse Canadian clinic population: a pilot study. Br J Dermatol. 2021;184(3):570–1.
Kouris A, Platsidaki E, Christodoulou C, Efstathiou V, Dessinioti C, Tzanetakou V, et al. Quality of life and psychosocial implications in patients with hidradenitis suppurativa. Dermatology. 2016;232(6):687–91.
Tzellos T, Yang H, Mu F, Calimlim B, Signorovitch J. Impact of hidradenitis suppurativa on work loss, indirect costs and income. Br J Dermatol. 2019;181(1):147–54.
van Straalen KR, Prens LM, Hylkema TH, Janse IC, Dickinson J, Houwing R, et al. Impact of hidradenitis suppurativa on work productivity and associated risk factors. J Am Acad Dermatol. 2021;84(5):1401–5.
Patel KR, Lee HH, Rastogi S, Vakharia PP, Hua T, Chhiba K, et al. Association between hidradenitis suppurativa, depression, anxiety, and suicidality: a systematic review and meta-analysis. J Am Acad Dermatol. 2020;83(3):737–44.
Garg A, Neuren E, Cha D, Kirby JS, Ingram JR, Jemec GBE, et al. Evaluating patients’ unmet needs in hidradenitis suppurativa: results from the Global Survey Of Impact and Healthcare Needs (VOICE) Project. J Am Acad Dermatol. 2020;82(2):366–76.
Marvel J, Vlahiotis A, Sainski-Nguyen A, Willson T, Kimball A. Disease burden and cost of hidradenitis suppurativa: a retrospective examination of US administrative claims data. BMJ Open. 2019;9(9): e030579.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83.
Quan H, Li B, Couris CM, Fushimi K, Graham P, Hider P, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–82.
van Walraven C, Austin PC, Jennings A, Quan H, Forster AJ. A modification of the Elixhauser comorbidity measures into a point system for hospital death using administrative data. Med Care. 2009;47(6):626–33.
Cartron A, Driscoll MS. Comorbidities of hidradenitis suppurativa: a review of the literature. Int J Womens Dermatol. 2019;5(5):330–4.
Dufour DN, Emtestam L, Jemec GB. Hidradenitis suppurativa: a common and burdensome, yet under-recognised, inflammatory skin disease. Postgrad Med J. 2014;90(1062):216–21 (quiz 20).
Tzellos T, Zouboulis CC. Review of comorbidities of hidradenitis suppurativa: implications for daily clinical practice. Dermatol Ther (Heidelb). 2020;10(1):63–71.
Desai N, Shah P. High burden of hospital resource utilization in patients with hidradenitis suppurativa in England: a retrospective cohort study using hospital episode statistics. Br J Dermatol. 2017;176(4):1048–55.
Kimball AB, Sundaram M, Gauthier G, Guérin A, Pivneva I, Singh R, et al. The comorbidity burden of hidradenitis suppurativa in the United States: a claims data analysis. Dermatol Ther (Heidelb). 2018;8(4):557–69.
Reddy S, Strunk A, Garg A. Comparative overall comorbidity burden among patients with hidradenitis suppurativa. JAMA Dermatol. 2019;155(7):797–802.
Matusiak Ł. Profound consequences of hidradenitis suppurativa: a review. Br J Dermatol. 2020;183(6):e171–7.
Patel ZS, Hoffman LK, Buse DC, Grinberg AS, Afifi L, Cohen SR, et al. Pain, psychological comorbidities, disability, and impaired quality of life in hidradenitis suppurativa [corrected]. Curr Pain Headache Rep. 2017;21(12):49.
Pavon Blanco A, Turner MA, Petrof G, Weinman J. To what extent do disease severity and illness perceptions explain depression, anxiety and quality of life in hidradenitis suppurativa? Br J Dermatol. 2019;180(2):338–45.
Liy-Wong C, Kim M, Kirkorian AY, Eichenfield LF, Diaz LZ, Horev A, et al. Hidradenitis suppurativa in the pediatric population: an international, multicenter, retrospective, cross-sectional study of 481 pediatric patients. JAMA Dermatol. 2021;157(4):385–91.
Resnik SR, Geisler EL, Reyes N, Lozano J, Ramirez-Caussade RA, Resnik B. Prevalence and risk factors for anemia in a population with hidradenitis suppurativa. Cureus. 2020;12(12): e12015.
Wertenteil S, Strunk A, Garg A. Incidence of obstructive sleep apnoea in patients with hidradenitis suppurativa: a retrospective population-based cohort analysis. Br J Dermatol. 2018;179(6):1398–9.
Garg A, Papagermanos V, Midura M, Strunk A, Merson J. Opioid, alcohol, and cannabis misuse among patients with hidradenitis suppurativa: a population-based analysis in the United States. J Am Acad Dermatol. 2018;79(3):495-500.e1.
Sabat R, Chanwangpong A, Schneider-Burrus S, Metternich D, Kokolakis G, Kurek A, et al. Increased prevalence of metabolic syndrome in patients with acne inversa. PLoS ONE. 2012;7(2): e31810.
Rondags A, van Straalen KR, Arends S, van der Zee HH, Prens EP, Spoorenberg A, et al. High prevalence of clinical spondyloarthritis features in patients with hidradenitis suppurativa. J Am Acad Dermatol. 2019;80(2):551-4.e1.
Gáspár K, Hunor Gergely L, Jenei B, Wikonkál N, Kinyó Á, Szegedi A, et al. Resource utilization, work productivity and costs in patients with hidradenitis suppurativa: a cost-of-illness study. Expert Rev Pharmacoecon Outcomes Res. 2022;22(3):399–408.
Orenstein LAV, Wright S, Strunk A, Garg A. Low prescription of tumor necrosis alpha inhibitors in hidradenitis suppurativa: a cross-sectional analysis. J Am Acad Dermatol. 2021;84(5):1399–401.
Zouboulis CC, del Marmol V, Mrowietz U, Prens EP, Tzellos T, Jemec GBE. Hidradenitis suppurativa/acne inversa: criteria for diagnosis, severity assessment, classification and disease evaluation. Dermatology. 2015;231(2):184–90.
Zouboulis CC, Bechara FG, Dickinson-Blok JL, Gulliver W, Horváth B, Hughes R, et al. Hidradenitis suppurativa/acne inversa: a practical framework for treatment optimization—systematic review and recommendations from the HS ALLIANCE working group. J Eur Acad Dermatol Venereol. 2019;33(1):19–31.
Drucker AM, Qureshi AA, Amand C, Villeneuve S, Gadkari A, Chao J, et al. Health care resource utilization and costs among adults with atopic dermatitis in the United States: a claims-based analysis. J Allergy Clin Immunol Pract. 2018;6(4):1342–8.
Kim GE, Shlyankevich J, Kimball AB (2014) The validity of the diagnostic code for hidradenitis suppurativa in an electronic database. Br J Dermatol 171(2):338–42. https://doi.org/10.1111/bjd.13041
Acknowledgements
The authors thank Shilpa Kakkar, PhD (Novartis Healthcare, Hyderabad, India), Ian Wright, PhD, and Trudy McGarry, PhD (Novartis, Dublin, Ireland) for providing medical writing support that was funded by Novartis Pharma AG in accordance with Good Publication Practice (GPP 2022) guidelines (https://www.ismpp.org/gpp-2022). The authors would also like to thank Juanzhi Fang (Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA) for her contribution to the development and conduct of this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was sponsored by Novartis Pharma AG, Basel, Switzerland.
Conflict of interest
Amit Garg is an advisor for AbbVie, Aclaris Therapeutics, Anaptys Bio, Aristea Therapeutics, Boehringer Ingelheim, Bristol Myers Squibb, Incyte, InflaRx, Insmed, Janssen, Novartis, Pfizer, Sonoma Biotherapeutics, UCB, Union Therapeutics, and Viela Biosciences, and receives honoraria. He also receives research grants from AbbVie, UCB and the National Psoriasis Foundation, and is co-copyright holder of the HS-IGA and HiSQOL instruments. Yvonne Geissbühler and Craig Richardson are full-time employees of Novartis Pharma AG, Basel, Switzerland, and Emma Houchen is a full-time employee of Novartis Pharmaceuticals, Dublin, Ireland. Nilesh Choudhary, Disha Arora, Varun Vellanki, Abhishek Srivastava, and Priyanka are full-time employees of Novartis Pharmaceuticals Corporation, Hyderabad, India. John Darcy II is a full-time employee of Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA. Alexa B. Kimball’s institution received grants from Abbvie, Anapyts Bio, Aristea, Bristol Myers Squibb, Eli Lilly, Incyte, Janssen, Moonlake, Novartis, Pfizer, UCB, and Sonoma Bio, and fellowship funding from Abbvie and Janssen. Alexa B. Kimball received consulting fees from Abbvie, Alumis, Bayer, Bristol Myers Squibb, Boehringer Ingelheim, Eli Lilly, FIDE, Novartis, Moonlake, Janssen, Pfizer, Priovant, Sonoma Bio, Sanofi UCB, and Ventyx; serves on advisory boards for Target RWE; serves as an advisory council member to the NIH Director; and serves on the board of directors of Almirall.
Availability of data and material
Data collected for this study will be made available to others upon request. Proposals for data requests will be reviewed and considered on an individual basis.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Code availability
Not applicable.
Author contributions
All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: All authors. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: All authors. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: EH. All authors read and approved the final version.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Garg, A., Geissbühler, Y., Houchen, E. et al. Disease Burden and Treatment Patterns Among US Patients with Hidradenitis Suppurativa: A Retrospective Cohort Study. Am J Clin Dermatol 24, 977–990 (2023). https://doi.org/10.1007/s40257-023-00796-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40257-023-00796-2