
Abstract
Introduction
Sofosbuvir/Velpatasvir/Voxilaprevir (SOF/VEL/VOX) is the first direct-acting antiviral (DAA) therapy approved for patients who have previously failed a DAA-containing regimen including NS5A inhibitors. In clinical trials, SOF/VEL/VOX was associated with high rates of sustained virologic response at post-treatment week 12 (SVR12) and was well tolerated. However, the effectiveness and safety of SOF/VEL/VOX in the real world remained uncertain. We aimed to perform a systematic review and meta-analysis to assess the real world effectiveness and safety of SOF/VEL/VOX.
Methods
We systematically searched the PubMed, Embase, Cochrane Library, Web of Science, and ClinicalTrials.gov databases for relevant real world studies published before January 28, 2022. Patients with previous treatment failure who received SOF/VEL/VOX were included. The primary outcome was the percentage of patients achieving SVR12. Secondary outcome included adverse events (AEs) during treatment.
Results
Fifteen studies with a total of 1796 HCV-infected patients with previous treatment failure were included. SVR12 rates were 93% (95% CI 91–95) in the ITT populations (n = 1517, 11 cohorts) and 96% (95% CI 95–97) in the PP populations (n = 1187, 10 cohorts). SVR12 rates were significantly higher in non-GT3-infected patients (OR = 2.29, 95% CI 1.23–4.27, P = 0.009) and non-cirrhotic patients (OR = 2.22, 95% CI 1.07–4.60, P = 0.03) than in GT3-infected patients and cirrhotic patients. Furthermore, the SVR12 rates of previous treatment of SOF/VEL were significantly lower than those of other regimens in both ITT and PP populations (P ≤ 0.001). Adverse events (AEs) were reported in 30% (228/760) of patients. Serious AEs (SAEs) were reported in 3.82% (29/760) of patients. The most frequently reported AEs were headache, asthenia, nausea, fatigue, and diarrhea, which were mostly mild in severity. AE-related treatment discontinuations were reported in 0.66% (5/760) of patients.
Conclusions
Consistent with clinical trials, the real world evidence indicates that SOF/VEL/VOX is a well-tolerated and highly effective salvage therapy for HCV-infected patients with previous treatment failure. However, there may still be a risk of treatment failure for patients with GT3 infection, cirrhosis, or SOF/VEL treatment failure. The protocol of this study was registered at PROSPERO, registration no. CRD 42022306828.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Patient populations in the real world tend to be more diverse and potentially less adherent to treatment compared to those in clinical trials. The effectiveness and safety of sofosbuvir/velpatasvir/voxilaprevir in the real world remained uncertain. |
Sofosbuvir/velpatasvir/voxilaprevir achieved 93% virologic cure overall as a salvage therapy in the real world. |
Effectiveness and safety results were consistent with those from clinical trials. |
There may be still a risk of treatment failure for patients with GT3 infection, cirrhosis, or Sofosbuvir/Velpatasvir treatment failure. |
Introduction
Hepatitis C virus (HCV) infection has a great impact on the morbidity and mortality of liver cirrhosis and hepatocellular carcinoma (HCC) patients, and it is a major public health problem in the world [1, 2]. Since the introduction of highly effective direct-acting antiviral drugs (DAAS) in 2011, significant changes have revolutionized the field of treatment [3]. In 2016, the World Health Organization (WHO) put forward a new global goal to eliminate viral hepatitis by 2030 [4]. Although the overall success of DAA treatment is high, there is still a small number of patients who have not eradicated the virus, and relapse or virus breakthroughs are reduced during DAA treatment [5]. The retreatment of patients with DAA failure may be challenging. Currently, a strategy for these patients with sofosbuvir/velpatasvir/voxilaprevir (SOF/VEL/VOX) was recommended by the European Association for the Study of the Liver (EASL) guidelines [6] and the American Association for the Study of Liver Diseases (AASLD) guidelines [7, 8].
SOF/VEL/VOX (Vosevi®) is a composite preparation containing a fixed dose of sofosbuvir (400 mg), velpatasvir (100 mg), and voxilaprevir (100 mg) in a single tablet [9]. SOF/VEL/VOX is a pan-genotypic DAA; it is recommended to be taken as one tablet orally with food every day. It was approved for use in adult patients with genotype (GT) 1–6 chronic HCV infection previously treated with a regimen containing NS5A inhibitors or with a regimen containing sofosbuvir without NS5A inhibitors on July 18, 2017, by the USA [10], on July 28, 2017, by the European Commission [11], and on December 20, 2019, by the China National Medical Products Administration [12].
Two phase III clinical trials (POLARIS-1 and POLARIS-4) [13] demonstrated the efficacy and safety of SOF/VEL/VOX for 12 weeks in patients who failed to achieve a sustained virologic response (SVR) based on various DAA regimens. SVR was defined as a serum HCV RNA level > 15 IU/ml 12 weeks after the treatment [13]. POLARIS-1 included patients of all genotypes who failed a treatment containing NS5A inhibitor, of which 46% had cirrhosis. Of the subjects treated with SOF/VEL/VOX, 96% (253/263) achieved SVR12. POLARIS-4 included patients with GT 1–4 infection who failed the previous DAA treatment regimen, which did not include NS5A inhibitors [13]. Of the subjects treated with SOF/VEL/VOX, 98% (178/182) achieved SVR12. SVR12 rate in patients without cirrhosis was higher than that in patients with cirrhosis in both POLARIS-1 and POLARIS-4 (99% vs. 93% and 94% vs. 86%, respectively) [13].
In the real world, the effectiveness of DAAs may be lower than that observed in clinical trials because the patient population is diverse and the compliance with treatment may be poor [14, 15]. The effectiveness of some DAA regimens in the real world has been proved to be similar to that in clinical trials [16, 17]. However, since SOF/VEL/VOX was just approved for the treatment of HCV-infected patients in 2017, the published data are limited, with only a small number of real world studies and clinical trials. Our objective is to evaluate the efficacy and safety of SOF/VEL/VOX as a HCV infection salvage therapy for patients with previous treatment failures in the real world through a systematic review and meta-analysis.
Methods
Literature Search
This study was reported in accordance with the recent updated Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 2020 guidelines [18]. The protocol of this study was registered at the International Prospective Register of Systematic Reviews (PROSPERO), with registration no. CRD 42022306828.
The literature search was conducted through PubMed, Embase, Cochrane Library, Web of Science, and ClinicalTrials.gov database for relevant studies published before January 28, 2022. Detailed literature search strategies of the databases are presented in Table 1. This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Inclusion and Exclusion Criteria
Studies were included if they met all of the inclusion criteria as follows: (1) Study design: prospective or retrospective observational cohorts, or any other real world study. (2) Population of study: adults regardless of genotype with chronic hepatitis C who had previously failed combined therapy with DAAs and interferon or interferon-free. Patients with HCC, with or without cirrhosis, coinfected with human immunodeficiency virus (HIV) infection or with hepatitis B virus (HBV) infection were also enrolled. (3) Intervention: patients received SOF/VEL/VOX 400/100/100 mg/day for 12 weeks; ribavirin (RBV) was added at the investigator’s discretion according to relevant guidelines. (4) Outcomes of study: the primary outcome was the percentage of patients achieving SVR12. The secondary outcome included any adverse events (AEs) during treatment.
Studies were excluded according to the exclusion criteria as follows: (1) studies with irrelevant outcomes; (2) studies were published as review, systematic review, meta-analysis, case report, editorial, letter, news, or clinical trial; (3) the number of patients included in the study was < 10; (4) publications that were not in English.
Data Extraction
Two reviewers (JX and BX) independently screened the retrieved studies according to the selection criteria. The full text of an article was reviewed if one or both reviewers considered a study potentially eligible. Two reviewers (JX and BX) manually screened the reference lists of retrieved articles to identify additional relevant studies. We resolved discrepancies by consultation with a third party (WL). For each included study, the following data were extracted independently by two reviewers (JX and BX): first author, publication year, country, population demographics (mean age and sex percentage), the sample size of the total cohort, genotype, and the rate of RAS testing at baseline.
Efficacy outcome contained the overall SVR12 rate of the intention-to-treat (ITT) population and the per-protocol (PP) population [19]. ITT population was defined as all patients who received at least one dose of SOF/VEL/VOX; these patients had SVR12 data, stopped treatment early, died during treatment, had poor compliance, or were lost to follow-up. The PP population was defined as the ITT population excluding patients with incomplete data, patients lost to follow-up during the study, or patients with poor compliance. If the SVR12 rate in ITT population was 100%, then the number of patients used to estimate SVR12 in the ITT population was used in the PP population [19]. SVR12 rates of different subgroups in both ITT and PP populations were evaluated as follows: HCV GT (GT1, 2, 3, 4, 5, or 6) and cirrhosis status, gender, and HCV treatment experience (prior HCV treatment).
Safety outcomes were estimated based on the incidence of any adverse events (AEs; any level), any common AEs, any serious AEs (SAEs), or withdrawal due to AEs. The cohort patients who reported these data were included in the safety population. The analysis of safety included only the studies that reported these data [19].
Risk of Bias Assessment
Two researchers (JX, BX) assessed bias in non-randomized studies using the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tool [20]. The risk of bias was assessed by considering the seven bias domains of the ROBINS-I tool, as shown below: (1) bias due to confounding; (2) bias in selection of participants into the study; (3) bias in classification of interventions; (4) bias due to deviations from intended interventions; (5) bias due to missing data; (6) bias in measurement of outcomes; (7) bias in selection of the reported result.
If the study had a low risk of bias in all areas, the overall risk of bias was determined to be low. If the study had some problems in at least one area, it was considered to have a moderate risk of bias. If the study was judged to have a serious risk of bias in at least one area, or the study was judged to have some problems in multiple areas, which greatly reduced confidence in the results, the risk of bias was considered to be serious [20]. When consensus could not be reached, disagreements were solved by consensus or through consultation with the third senior examiner (WL).
Data Analysis
Descriptive tables that included data on population characteristics, interventions, and outcomes were created. The meta-analysis was performed using Stata software (version 15.0) and Revman Software (version 5.4). Excel 2016 was used for statistical analysis and data arrangement. For the dichotomous results we extracted, the results were expressed as the odds ratio (OR) with a 95% confidence interval (95% CI). The heterogeneity of the results across studies was assessed with the I2 statistic. If P < 0.05 or I2 > 50%, the random-effects model was used; otherwise, the fixed effects model was selected. The overall SVR12 rate was calculated in a way that resembles a meta-analysis: each study has conferred a weight, and the rate of SVR12 in each study is adjusted according to the weight that the study contributes to the overall SVR12 rate. The weighted value of each study is assigned by the software based on the sample size of each study. The SVR12 values from the different studies were pooled using the metaprop command in Stata software. All tests were two-sided, and P < 0.05 was regarded as statistically significant. Additionally, Egger’s and Begg’s tests [21, 22] were used to evaluate publication bias together with a funnel plot. To further confirm the overall results, a sensitivity analysis was conducted by omitting one study at a time to test the robustness of the study data.
Results
Main Characteristics of the Studies and Populations
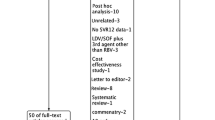
Figure 1 shows the results of the systematic publication review and screening process. A total of 1796 HCV-infected patients were examined in 15 studies [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37], which were selected among 466 screened articles. We excluded 204 duplicate records by checking the author name, publication date, and journal title. Following the inclusion and exclusion criteria previously described, 15 studies were eligible, including 4 conference abstracts [23,24,25,26] and 11 full articles [27,28,29,30,31,32,33,34,35,36,37]. The studies were mainly conducted in eight countries: US (n = 4), Canada (n = 3), Italy (n = 2), Australian (n = 1), England (n = 1), France (n = 1), Germany (n = 1), and Spain (n = 1), and there was 1 multi-country study included Germany, Italy, and Spain. There were seven single-center studies [23, 25,26,27, 32, 34, 37] and eight multicenter studies [24, 28,29,30,31, 33, 35, 36]. A summary of the demographic and clinical characteristics of the patients is presented in Table 2. The results of the risk of bias are presented in Table 3.

PRISMA process flow of study selection
Efficacy Analyses: The Overall SVR12 Rate and by Subgroups
Of the 1796 patients included in the 15 studies, SVR12 data from the ITT population (reported in 11 studies, n = 1517) and the PP population (reported in 10 studies, n = 1187) were both included in the meta-analysis. Six studies (n = 908) [27, 29, 32,33,34, 36] reported SVR12 rate in both ITT and PP populations, and four studies (n = 279) [24, 25, 28, 32] reported SVR12 rate only in PP populations. SVR12 rates in the individual cohorts ranged from 85 to 100% of the ITT population (Fig. 2) and ranged from 90 to 100% of the PP population (Fig. 3). The funnel plot of the meta-analysis in the ITT population is available in Fig. 4. Egger’s (P = 0.902) and Begg’s tests (P = 0.755) both confirmed that there was no statistically significant publication bias.

The overall SVR12 rate in the ITT population

The overall SVR12 rate in the PP population

The funnel plot of the meta-analysis in the ITT population
The results from the meta-analysis showed that the overall SVR12 rates with SOF/VEL/VOX were 93% (95% CI 91–95, I2 = 55.08%) in the ITT population (n = 1517) with heterogeneity and 96% (95% CI 95–97, I2 = 0%) in the PP population (n = 1187) with no heterogeneity. To the same extent, the heterogeneity may come from the study of Papaluca et al. [36], because when excluding this study, the value of I2 decreased. The results of sensitivity analysis in ITT population are listed in Table 4. The results of sensitivity analysis showed that excluding any study had little effect on the overall results, suggesting that the results were stable.
SVR12 rate in the PP population was similar to that in the ITT population for all GT subgroups (Fig. 5). The overall SVR12 rates of GT1 (n = 879; 7 cohorts), GT2 (n = 62; 5 cohorts), GT3 (n = 339; 7 cohorts), GT4 (n = 47; 4 cohorts), and GT6 (n = 7; 3 cohorts) were 92% (95% CI 86–97), 97% (95% CI 89–100), 87% (95% CI 83–92), 97% (95% CI 88–100), and 100% (95% CI 73–100), respectively (Fig. 5). There were insufficient published cohort data to evaluate SVR12 rate for patients infected with HCV GT5, and the data of GT6 populations were also very few in these study.

The overall SVR12 rate of different genotypes in ITT and PP population
In phase III trials, lower SVR12 rates were observed in GT3-infected patients and cirrhotic patients [13]. We performed a subgroup analysis to compare the SVR12 rates of non-GT3-infected patients with GT3-infected patients and that of non-cirrhotic patients with cirrhotic patients. It showed that the SVR12 rates were significantly higher in non-GT3-infected patients and non-cirrhotic patients than in GT3-infected patients (OR = 2.29, 95% CI 1.23–4.27, P = 0.009) and cirrhotic patients (OR = 2.22, 95% CI 1.07–4.60, P = 0.03) (Figs. 6, 7). We also found that the SVR12 rate of patients who had been treated with SOF/VEL previously was significantly lower than for those treated with other regimens in both ITT and PP populations (P ≤ 0.001) (Fig. 8). Furthermore, there was no significant difference in the SVR12 rate between males and females in both ITT and PP populations (P > 0.5) (Fig. 9).

The overall SVR12 rate of non-GT3-infection versus GT3-infection in ITT population

The overall SVR12 rate of non-cirrhosis versus cirrhosis in ITT population

The overall SVR12 rate of patients who had been treated with SOF/VEL previously versus those treated with other regimens

The overall SVR12 rate of male versus female patients
Safety Analysis
Safety data were summarized from 760 patients with safety reports (9 cohorts) [23, 25, 28,29,30, 33,34,35,36], and any AEs were reported in 228 patients (30%, Table 5). No single AE was reported with a frequency > 10%. The most frequently reported AEs were headache (8.29%, 5 cohorts), asthenia (5.53%, 1 cohort), nausea (4.61%, 5 cohorts), fatigue (4.47%, 4 cohorts), and diarrhea (3.95%, 4 cohorts). Twenty-nine (3.82%, 6 cohorts) SAEs were reported including acute kidney injury, liver decompensation, HCC, urothelial carcinoma, abdominal hernia, cholecystectomy, acute-on-chronic liver failure, variceal bleeding, and hepatorenal syndrome, but not all these SAEs were drug-related. In total, five patients (0.66%, 3 cohorts) discontinued treatment because of an AE [29, 33, 36]: one patient underwent liver transplantation at week 10 [29]; one patient died of liver failure 2 months after treatment discontinuation [33]; two patients had abdominal pain and one deteriorating renal function [36].
Discussion
Real world studies provide valuable information for the treatment efficacy and safety in general clinical practice; however, compared with patients participating in clinical trials, these patients are more heterogeneous and more inclusive of marginalized populations [38]. They provide valuable information for patients, doctors, decision-makers, and payers and are an important supplement to the results of clinical trials [19]. The results of this meta-analysis show that SOF/VEL/VOX is an effective and well-tolerated salvage therapy for patients with HCV infection who had previous treatment failures in the real world.
Of the 1796 patients in our study, 1517 were included in the ITT population, and 1187 were included in the PP population. This change in the number of patients was because four studies [24, 25, 28, 32] did not report on the ITT populations at all, and six studies [23, 27, 29, 33, 34, 36] reported on both ITT and PP populations. According to ROBINS-I criteria [20], most studies were deemed to have an overall risk of bias rating of moderate risk. Sensitivity analysis showed that these risks had little influence on our results, indicating that our results were relatively stable.
Although the pooled rate of SVR12 in the ITT population was 93%, there was heterogeneity (I2 = 55.08%), which may have come from the study of Papaluca et al. [36], since, when excluding this study, the heterogeneity decreased to a low level (I2 = 44.32%). This may be because the study included patients who were notable for “difficult-to-cure” characteristics [36]. The cohort included a high prevalence rate of cirrhosis (78%) and HCV GT3-infected patients (72%), the majority with portal hypertension (PHT) (61%) [36], which was significantly higher than in phase III clinical trials and most other real world studies of SOF/VEL/VOX we included.
In the era of DAAs, the treatment of patients with GT3 infection remains a clinical challenge [39]. In some studies, GT3-infected patients and patients with cirrhosis remain difficult to treat [40, 41]. Due to the small sample size of GT3 and cirrhotic patients in the PP population, we only conducted subgroup analysis of GT3 and cirrhosis in the ITT population; however, the SVR12 rate may be higher when the PP population is added. In our research, the SVR12 rate of patients with HCV GT3 infection was lower than with other genotypes, suggesting that patients with GT3 infection have a higher risk of virologic relapse than those with other genotypes. The SVR12 rate was found to be lower in patients with cirrhosis than without in two phase III clinical trials [13]. Many real world studies find high SVR12 rates following DAA therapy in patients with cirrhosis, but some of them also suggested differences from those without cirrhosis [42,43,44]. In the course of our research, we also found that the SVR12 rate was lower in cirrhotic patients than in those without. Adding weight-based ribavirin to SOF/VEL/VOX in GT3 patients with cirrhosis who had failed with an NS5A inhibitor-based regimen to minimize the risk of recurrence was recommended in current AASLD guidelines [8]; however, the level of evidence and strength of the recommendation were just IIa and C, respectively. In this meta-analysis, RBV was added in 9 studies [24,25,26, 29, 31, 33,34,35,36] of 157 (8.74%) patients because of treatment needs. Limited by small populations, we did not perform a subgroup analysis of RBV. The necessity of using RBV can be further discussed in future studies.
The study of Pabjan et al. [45] also demonstrated that in addition to GT3-infected and cirrhotic patients, male sex and treatment experience significantly reduced the chances of virologic response. However, in our study, there was no significant difference in the SVR12 rate between males and females in both the ITT and PP populations. This may be due to the higher proportion of male sex (79.68%) in these real world studies. Also, it was found that patients with prior SOF/VEL treatment experience had a lower incidence of SVR12 rate in some studies [27, 28, 35, 37]. Due to the diversification of previous treatment and limited data, we just selected the subgroup of patients with SOF/VEL treatment experience for further analysis. Our research also found that the SVR12 rates of patients who had SOF/VEL treatment failure were significantly lower than in patients with other regimens in both ITT and PP populations (P ≤ 0.001). However, it is not clear why the SVR12 rate of patients receiving SOF/VEL/VOX retreatment who had failed the treatment with SOF/VEL was worse than for those who failed a different regimen. Since SOF/VEL includes two of the three components in SOF/VEL/VOX, any factors related to the failure of SOF/VEL treatment may also affect the effect of at least two of the three components in SOF/VEL/VOX [27]. We think this is precisely the reason so may wish to clarify this hypothesis or expand upon it.
In our study, resistance testing was not available in all studies; some studies also showed that there was no significant difference in the incidence of SVR12 between patients with and without RASs records [28]. According to the analysis of patients included in the phase III clinical trials, baseline RASs did not affect the SVR of patients with DAA experienced after 12 weeks of treatment with SOF/VEL/VOX [46]. Although pretreatment RAS testing was recommended in some situations in AASLD guidelines, since whether RASs had been done or not had no effect on the overall SVR12 rate of patients, baseline RAS testing was not recommended before using SOF/VEL/VOX according to AASLD guidelines [8]. The rates of RAS testing at baseline were recorded in ten studies [24, 28,29,30,31,32, 34,35,36,37]. Only two studies [31, 32] had a 100% baseline RAS testing rate. Since most studies did not have data on the correlation between RAS testing and SVR12 rate, we did not perform a subgroup analysis of RASs.
Because VEL and VOX are substrates of the CYP450 system, SOF, VEL, and VOX are all substrates of the P-glycoprotein drug transporter [9]. Drugs such as P-glycoprotein inducers and/or CYP2B6, CYP2C8, or CYP3A4 inducers may significantly reduce the plasma concentrations of any of the three drugs in SOF/VEL/VOX, thus reducing the therapeutic effect of SOF/VEL/VOX [47]. The combination of these drugs with SOF/VEL/VOX is not recommended [9, 47]. Only two studies [33, 36] included mentioned drug interactions about SOF/VEL/VOX, in which only three patients received drugs not recommended for use with SOF/VEL/VOX. One patient received an OATP1B1 inhibitor eltrombopag, which may increase the risk of elevated ALT due to increased VOX plasma concentration [33]. The second patient received simvastatin, which may increase the concentration of simvastatin due to the inhibition of BCRP by VEL [33]. The third participant [36] was prescribed a proton-pump inhibitor used with SOF/VEL/VOX, but no detailed drug name was recorded. None of them showed safety signals potentially related to drug-drug interactions (DDIs) [33, 36].
In this meta-analysis, the tolerance of SOF/VEL/VOX was similar to that reported in the POLARIS trials [13]. Headache, asthenia, diarrhea, fatigue, and nausea were the most commonly reported AEs [9, 13, 48, 49]. However, in our study asthenia was only reported in one study [28] with an incidence of 5.53%, which in the POLARIS-1 trials was 8% [50]. In our study, only 0.66% of patients terminated treatment because of AEs, which was 1% or less in clinical trials. The safety results were consistent with those in clinical trials.
To the best of our knowledge, this is the first meta-analysis reporting the effectiveness and safety of SOF/VEL/VOX as a hepatitis C virus infection salvage therapy for patients with previous treatment failures in the real world. Although our study was strictly conducted based on the PRISMA guidelines, this meta-analysis has several limitations to be noted. First, the major limitation of this study is the small number of included studies. Even though comprehensive search strategies were performed, only 15 studies met our inclusion criteria. However, we still believe this to be a comparatively large sample size as HCV treatment failures were an uncommon event since the average failure rate with DAA treatment is < 5% [51, 52]. Second, we included papers published as both conference abstracts and full papers, which may have led to a lack of consistency. Only the overall SVR12 results were reported in the conference abstracts, and most lacked SVR12 data for each subgroup. Third, the level of detail reported across the individual studies and the characteristics of the patients were inconsistent. Since the approval of SOF/VEL/VOX for the treatment of HCV-infected patients who have previously had treatment failure was < 5 years at the beginning of our study, the real world studies were relatively limited. Insufficient data were available to analyze the SVR12 rate in GT5-infected populations; although there were GT6-infected population data, the number of patients was only seven, which was relatively too small to analyze. In a phase III clinical trial, patients coinfected with HBV or HIV and those with decompensated cirrhosis were excluded; however, patients in the real world often have multiple complications. Most patients in the studies we included were coinfected with HIV and cirrhosis, or even decompensated cirrhosis; some even had HCC before the treatment began, and only two studies excluded the patients with decompensated cirrhosis (Child-Pugh score B or C) [34, 36]. This may lead to different results from clinical trials. Furthermore, most of the studies included in our research were from western countries, and the data on populations in Asia and other countries were lacking, which may be related to the limited marketing region of this drug. More national and ethnic research is needed for further study.
Conclusion
In conclusion, the results of this meta-analysis demonstrate that the real world effectiveness and safety of SOF/VEL/VOX in 1796 patients were consistent with those observed in clinical trials. Furthermore, real world evidence indicates that SOF/VEL/VOX is a highly effective and well-tolerated salvage therapy option for previous treatment failure in HCV-infected patients. However, there is still a risk of treatment failure for patients with GT3 infection, cirrhosis, or those with SOF/VEL treatment failure. More national and ethnic research is needed for further study.
References
Jing W, Liu J, Liu M. Global trends and regional differences in hepatitis C virus infection prevalence and implications for prevention—worldwide, 1990–2017. China CDC Wkly. 2020;2(30):564–9.
Di Marco L, La Mantia C, Di Marco V. Hepatitis C: standard of treatment and what to do for global elimination. Viruses. 2022;14(3):505.
Kohli A, Shaffer A, Sherman A, et al. Treatment of hepatitis C: a systematic review. JAMA. 2014;312(6):631–40.
Klein MB. Simplifying HCV treatment: a pathway to elimination and model for delivering health care to vulnerable populations. Lancet Gastroenterol Hepatol. 2022;7:277–9.
Benítez-Gutiérrez L, Barreiro P, Labarga P, et al. Prevention and management of treatment failure to new oral hepatitis C drugs. Expert Opin Pharmacother. 2016;17(9):1215–23.
Pawlotsky JM, Negro F, Aghemo A, et al. EASL recommendations on treatment of hepatitis C 2018. J Hepatol. 2018;69(2):461–511.
Panel A. Hepatitis C guidance: AASLD-IDSA recommendations for testing, managing, and treating adults infected with hepatitis C virus. Hepatology. 2015;62(3):932–54.
Chung RT, Ghany MG, Kim AY, et al. Hepatitis C guidance 2018 update: AASLD-IDSA recommendations for testing, managing, and treating hepatitis C virus infection. Clin Infect Dis. 2018;67(10):1477–92.
Vosevi, prescribing information. Gilead Sciences, Inc., CA, USA (2017). Available from: https://www.gilead.com/-/media/files/pdfs/medicines/liver-disease/vosevi/vosevi_pi.pdf. Accessed Nov 2019.
Press Release 2017. Available from: https://www.gilead.com/news-and-press/press-room/press-releases/2017/7/us-food-and-drug-administration-approves-gileads-vosevi-sofosbuvirvelpatasvirvoxilaprevir-for-retreatment-of-adults-with-chronic-hepatitis-c. Accessed Jul 2017.
Press Release 2017. Available from: https://www.gilead.com/news-and-press/press-room/press-releases/2017/7/european-commission-grants-marketing-authorization-for-gileads-vosevi-sofosbuvirvelpatasvirvoxilaprevir-for-the-treatment-of-all-genotypes-of-ch. Accessed Jul 2017.
Press Release 2019. Available from: https://www.gilead.com/news-and-press/press-room/press-releases/2019/12/china-national-medical-products-administration-approves-vosevi-sofosbuvir-velpatasvir-and-voxilaprevir-for-people-with-chronic-hepatitis-c-infecti. Accessed Dec 2019.
Bourlière M, Gordon SC, Flamm SL, et al. Sofosbuvir, velpatasvir, and voxilaprevir for previously treated HCV infection. N Engl J Med. 2017;376(22):2134–46.
Tacke F, Gunther R, Buggisch P, et al. Treatment of HCV genotype 2 with sofosbuvir and ribavirin results in lower sustained virological response rates in real life than expected from clinical trials. Liver Int. 2017;37:205–11.
Backus LI, Belperio PS, Shahoumian TA, et al. Effectiveness of sofosbuvir-based regimens in genotype 1 and 2 hepatitis C virus infection in 4026 US Veterans. Aliment Pharmacol Ther. 2015;42:559–73.
Chiu WN, Hung CH, Lu SN, et al. Real-world effectiveness of glecaprevir/pibrentasvir and ledipasvir/sofosbuvir for mixed genotype hepatitis C infection: a multicenter pooled analysis in Taiwan. J Viral Hepat. 2020;27(9):866–72.
Nozaki A, Atsukawa M, Kondo C, et al. The effectiveness and safety of glecaprevir/pibrentasvir in chronic hepatitis C patients with refractory factors in the real world: a comprehensive analysis of a prospective multicenter study. Hepatol Int. 2020;14(2):225–38.
Page MJ, Mckenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Online). 2021;372: n71.
Lampertico P, Carrión JA, Curry M, et al. Real-world effectiveness and safety of glecaprevir/pibrentasvir for the treatment of patients with chronic HCV infection: a meta-analysis. J Hepatol. 2020;72(6):1112–21.
Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–101.
Egger M, Davey-Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Brown P, Demertzis Z, Jafri SM. Single center experience with sofosbuvir/velpatasvir/voxilaprevir (Vosevi) based therapy for chronic hepatitis C infection. Gastroenterology. 2019;156(6):S1344.
De Quadros Onofrio F, Cooper C, Borgia SM, et al. Prior therapy with sofosbuvir/velpatasvir associated with reduced response to sofosbuvir/velpatasvir/voxilaprevir: results from a canadian prospective registry. Hepatology. 2019;70:981A (v70 suppl.1 2019).
Hezode C, Guyader D, Nguyen-Khac E, et al. Sofosbuvir + velpatasvir + voxilaprevir in DAA failure patients with cirrhosis: final results of the French compassionate use program. J Hepatol. 2019;70(1): e224.
Janjua N, Wilton J, Cook D, et al. Real-world effectiveness of sofosbuvir/velpatasvir/voxilaprevir as a hepatitis C virus infection salvage treatment. J Hepatol. 2020;73:S356–7.
Belperio PS, Shahoumian TA, Loomis TP, et al. Real-world effectiveness of sofosbuvir/velpatasvir/voxilaprevir in 573 direct-acting antiviral experienced hepatitis C patients. J Viral Hepat. 2019;26(8):980–90.
Llaneras J, Riveiro-Barciela M, Lens S, et al. Effectiveness and safety of sofosbuvir/velpatasvir/voxilaprevir in patients with chronic hepatitis C previously treated with DAAs. J Hepatol. 2019;71(4):666–72.
Degasperi E, Spinetti A, Lombardi A, et al. Real-life effectiveness and safety of sofosbuvir/velpatasvir/voxilaprevir in hepatitis C patients with previous DAA failure. J Hepatol. 2019;71(6):1106–15.
Pearlman B, Perrys M, Hinds A. Sofosbuvir/velpatasvir/voxilaprevir for previous treatment failures with glecaprevir/pibrentasvir in chronic hepatitis C infection. Am J Gastroenterol. 2019;114(9):1550–2.
Salazar AD, Dietz J, Maio V, et al. Prevalence of resistance-associated substitutions and retreatment of patients failing a glecaprevir/pibrentasvir regimen. J Antimicrob Chemother. 2020;75(11):3349–58.
Pisaturo M, Starace M, Minichini C, et al. Virological patterns of hepatitis C virus patients with failure to the current-generation direct-acting antivirals. Int J Antimicrob Agents. 2020;56(3): 106067.
Vermehren J, Serfert Y, Cornberg M, et al. Sofosbuvir, velpatasvir, and voxilaprevir for patients with failure of previous direct-acting antiviral therapy for chronic hepatitis C: results from the German Hepatitis C-Registry (DHC-R). Gastroenterology. 2020;58(9):841–6.
Da BL, Lourdusamy V, Kushner T, et al. Efficacy of sofosbuvir/velpatasvir/voxilaprevir in direct-acting antiviral experienced patients with hepatitis C virus. Eur J Gastroenterol Hepatol. 2021;33(6):859–61.
Onofrio FQ, Curtis C, Borgia SM, et al. Salvage therapy with sofosbuvir/velpatasvir/voxilaprevir in DAA-experienced Patients: results from a prospective Canadian Registry. Clin Infect Dis. 2021;72(11):e799–805.
Papaluca T, Roberts SK, Strasser SI, et al. Efficacy and safety of sofosbuvir/velpatasvir/voxilaprevir for hepatitis C virus (HCV) NS5A-inhibitor experienced patients with difficult to cure characteristics. Clin Infect Dis. 2021;73(9):e3288–95.
Smith DA, Bradshaw D, Mbisa J, et al. Real world SOF/VEL/VOX retreatment outcomes and viral resistance analysis for HCV patients with prior failure to DAA therapy. J Viral Hepat. 2021;28(9):1256–64.
Aghemo A, Horsmans Y, Bourgeois S, et al. Real-world outcomes in historically underserved patients with chronic hepatitis C infection treated with glecaprevir/pibrentasvir. Infect Dis Ther. 2021;10:2203–22.
Foster GR, Afdhal N, Roberts SK, et al. Sofosbuvir and velpatasvir for HCV genotype 2 and 3 infection. N Engl J Med. 2015;373:2608–17.
Meszaros M, Truchi R, Ouzan D, et al. Sofosbuvir, glecaprevir, pibrentasvir, and ribavirin as a rescue therapy in difficult-to-treat HCV patients. Hepatology. 2021;74:2304–6.
Zarębska-Michaluk D, Jaroszewicz J, Parfieniuk-Kowerda A, et al. Effectiveness and safety of pangenotypic regimens in the most difficult to treat population of genotype 3 HCV infected cirrhotics. J Clin Med. 2021;10(15):3280.
Flisiak R, Janczewska E, Wawrzynowicz-Syczewska M, et al. Real-world effectiveness and safety of ombitasvir/paritaprevir/ritonavir ± dasabuvir ± ribavirin in hepatitis C: AMBER study. Aliment Pharmacol Ther. 2016;44(9):946–56.
Xia Huan Lu, Chengzhen WY, et al. Efficacy and safety of direct-acting antiviral therapy in patients with chronic hepatitis C virus infection: a real-world single-center experience in Tianjin China. Front Pharmacol. 2020;11:710.
Naguib GG, Farid A, Hassan M, et al. Direct-acting antiviral regimens in egyptian patients with chronic hepatitis C virus infection: a real-world single-center experience. Arab J Gastroenterol. 2021;22:285–91.
Pabjan P, Brzdęk M, Chrapek M, et al. Are there still difficult-to-treat patients with chronic hepatitis C in the era of direct-acting antivirals? Viruses. 2022;14(1):96.
Sarrazin C, Cooper CL, Manns MP, et al. No impact of resistance-associated substitutions on the efficacy of sofosbuvir, velpatasvir, and voxilaprevir for 12 weeks in HCV DAA experienced patients. J Hepatol. 2018;69:1221–30.
Mathur P, Kottilil S, Wilson E. Sofosbuvir/velpatasvir/voxilaprevir: a highly effective option for retreatment of hepatitis C in difficult-to-treat patients. Antivir Ther. 2019;24:1–10.
Jacobson IM, Lawitz E, Gane EJ, et al. Efficacy of 8 weeks of sofosbuvir, velpatasvir, and voxilaprevir in patients with chronic HCV infection: 2 phase 3 randomized trials. Gastroenterology. 2017;153(1):113–22.
Bourliere M, Gordon SC, Schiff ER, et al. Deferred treatment of sofosbuvir-velpatasvir-voxilaprevir for patients with chronic hepatitis C virus who were previously treated with an NS5A inhibitor: an open-label substudy of POLARIS-1. Lancet Gastroenterol Hepatol. 2018;3:559–65.
Bourlière M, Gordon SC, Schiff ER, et al. Deferred treatment with sofosbuvir-velpatasvir-voxilaprevir for patients with chronic hepatitis C virus who were previously treated with an NS5A inhibitor: an open-label substudy of POLARIS-1. Lancet Gastroenterol Hepatol. 2018;3:559–65.
Higley C, Hsu CC, Smith C, et al. Safety and efficacy of sofosbuvir/velpatasvir/voxilaprevir in post-liver transplant patients with previous direct-acting antiviral failure: Six case reports. World J Hepatol. 2020;12:1341–8.
Patel S, Martin MT, Flamm SL. Sofosbuvir/velpatasvir/voxilaprevir for hepatitis C virus retreatment in decompensated cirrhosis. Liver Int. 2021;41:3024–7.
Acknowledgements
I am very grateful to my husband for his help and support. We also appreciate the valuable comments from other members of our group.
Funding
No funding or sponsorship was received for this study or publication of this article. The Rapid Service Fee was funded by Beijing Youan Hospital, Capital Medical University, Beijing, China.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work, and have given their approval for this version to be published.
Author Contributions
Jing Xie and Bin Xu searched the literature and collected the data; Jing Xie wrote the manuscript; Wei Liu designed the project and revised the manuscript; Linlin Wei and Chunyang Huang helped polish the language of the manuscript. All authors have read and approved the manuscript.
Disclosures
Jing Xie, Bin Xu, Linlin Wei, Chunyang Huang, and Wei Liu all have nothing to disclose.
Compliance with Ethics Guidelines
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Registration and Protocol
The protocol for this study was registered at the International Prospective Register of Systematic Reviews (PROSPERO), with registration no. CRD 42022306828. The address is: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=306828.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Xie, J., Xu, B., Wei, L. et al. Effectiveness and Safety of Sofosbuvir/Velpatasvir/Voxilaprevir as a Hepatitis C Virus Infection Salvage Therapy in the Real World: A Systematic Review and Meta-analysis. Infect Dis Ther 11, 1661–1682 (2022). https://doi.org/10.1007/s40121-022-00666-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-022-00666-0