
Abstract
Introduction
Myasthenia gravis (MG) is a rare, debilitating, chronic disorder caused by the production of pathogenic immunoglobulin G autoantibodies against the neuromuscular junction. A lack of real-world studies in rare diseases reflects a relatively limited understanding of the significant unmet needs and burden of disease for patients. We aimed to provide comprehensive real-world insights into the management and burden of MG from treating physicians in the United States (US).
Methods
Data were collected using the Adelphi Real World MG Disease Specific Programme™, a point-in-time survey of physicians and their patients with MG, in the US between March and July 2020. Physician-reported clinical data, including demographics, comorbidities, symptoms, disease history, treatments, and healthcare resource utilization, were collected.
Results
In total, 456 patient record forms were completed by 78 physicians based in the US. At time of survey completion, patient mean age was 54.5 years. Mean time from symptom onset to diagnosis was 9.0 months (n = 357). Ocular symptoms were reported in 71.7% of patients. General fatigue affected 47.1% of patients and over half of those reported the severity as moderate or severe (59.5%, n = 128). Acetylcholinesterase inhibitors and/or steroids were the most frequently prescribed first-line treatment type among patients receiving treatment at time of survey completion and with moderate-to-severe symptoms (77.9%, n = 159/204). High-dose steroids (n = 14) and intravenous immunoglobulin (n = 13) were the most prescribed acute treatments among those receiving an acute treatment at time of survey completion (n = 36), with symptom exacerbations or myasthenic crises being the most common reasons for acute treatment. On average, 2.5 healthcare professionals were involved in patient management and 5.0 consultations were made per patient over the last 12 months.
Conclusions
Our findings indicated that, despite treatment, there is a proportion of patients with MG in the US who had a significant need for improved disease management.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Why carry out this study? |
There is a lack of real-world evidence in myasthenia gravis (MG), reflecting a limited understanding of patients’ unmet needs and burden of disease. |
What did the study ask? |
Using data collected from physician-completed patient record forms as part of the Adelphi Real World MG Disease Specific Programme™ in MG, this study aimed to provide comprehensive real-world insights into the clinical presentation and management of MG from treating physicians in the United States. |
What was learned from the study? |
The mean number of symptoms per patient was the same (five) after treatment as it was at diagnosis, suggesting that many patients were still impacted by disease, despite treatment. |
Over one-third of the patients in this cohort required acute treatment at some point, predominantly for the treatment of exacerbations or myasthenic crisis. |
On average, 2.5 healthcare professionals were involved in patient management and 5.0 consultations were made per patient over the last 12 months. |
Our findings showed that current maintenance treatment does not fully control the disease, as patients continued to experience a high burden of disease and healthcare resource utilization despite treatment, highlighting the need for improved treatment options in MG. |
Introduction
Myasthenia gravis (MG) is a debilitating, chronic, autoimmune, neuromuscular disease with most patients experiencing fluctuating muscle weakness and fatigue [1, 2]. MG is caused by pathogenic immunoglobulin G autoantibodies, which can inhibit signal transmission at the neuromuscular junction (NMJ) by binding to various proteins including receptors [3,4,5]. Approximately 74–88% of patients have acetylcholine receptor (AChR) autoantibody-positive MG. Synaptic transmission to muscle fibers is impacted by these pathogenic autoantibodies that, by binding to receptors, block acetylcholine and increase receptor degradation. Additionally, AChR autoantibodies trigger the classical complement cascade, which converges at complement C5, leading to damage of the NMJ, and ultimately impairment to muscle contraction [6].
MG is a rare disease, with an estimated 60,000 cases of MG in the United States (US) [7, 8]. As with many rare diseases, because of the relatively low prevalence compared with more common diseases, there is a lack of real-world studies in MG to understand and address patients’ unmet needs and the burden of disease [9]. While randomized clinical trials are necessary to obtain robust efficacy and safety data on a treatment, observational real-world studies are also important as they can provide information on larger, more representative populations compared with clinical trials, and an understanding of the true progression and management of the disease [9]. An analysis of insurance claims between 2010 and 2019 from the IBM® MarketScan® database showed that 91% of patients living with MG in the US received drug therapy, and 40% of those received non-steroidal immunosuppressive treatment (IST) or biologics [10]. However, some survey research has suggested that as many as 50% of patients with MG fail to reach minimal symptom expression (Myasthenia Gravis Activities of Daily Living score 0 or 1) [11], while more stringent criteria for refractory disease has been estimated at 10–20% of the MG population [12, 13]. Inadequately controlled disease is more likely to have significant impact on prognosis, health-related quality of life, and use of healthcare resources compared with the nonrefractory MG population [3, 13,14,15]. Hospitalizations, myasthenic crises, and use of acute treatments for MG worsening such as IVIg and PLEX are key drivers of increased MG-related healthcare costs [16]. Despite these insights, comprehensive data are still lacking on real-world clinical experiences and perspectives from a large sample.
Adelphi Real World Disease Specific Programmes™ (DSPs) are an established methodology for investigating treatment practices across a large range of diseases using point-in-time surveys [17]. They collect real-world data from clinical practice, including patient demographics, treatment practices and physician-reported healthcare resource utilization (HCRU) [9].
Here, using data from the MG DSP, we aimed to provide comprehensive real-world insights and evidence into the HCRU, management and disease burden of MG in the US.
Methods
Study Design and Data Source
Data were obtained via the Adelphi Real World MG DSP, a point-in-time survey of MG-treating physicians in the US and their patients between March and July 2020. A complete description of the methods of the survey has been previously published and validated [17,18,19], and further information on the phases of a DSP can be found in Supplementary Material (Fig. 1). This survey obtained ethics approval from the Western Institutional Review Board, sponsor protocol number: AG8768. The DSP is Health Insurance Portability and Accountability Act compliant, and all data was aggregated and de-identified. Patients and physicians provided informed consent to take part in the Adelphi Myasthenia Gravis Disease Specific Programme™ market research survey, on which this secondary data analysis is based. Data were collected in such a way that patients and physicians could not be identified directly.
Study Population
Physicians were recruited to participate in the DSP by local fieldwork agents and were eligible to participate in the survey following a short screening questionnaire. Physicians and healthcare professionals (HCPs) were eligible for inclusion if their primary specialty was identified as neurology, geriatrics, or primary care medicine. All those included were required to be treating at least one patient with a confirmed diagnosis of MG, based on the judgement and diagnostic skills of the respondent physician. Physician participation was financially incentivized, with reimbursement upon survey completion according to fair market research rates. No formal patient selection procedures were in place. However, physicians and HCPs were asked to provide data for a consecutive series of patients to avoid selection bias and to generate a patient sample reflective of real-world practice, with data collected at the time of each patient’s appointment to reduce the likelihood of recall bias. Furthermore, by not only collecting data from specialist centers, it was more likely that data would be collected for a more general MG population than severe patients only. Due to the consecutive nature of patient recruitment to mitigate against selection bias, and the diversity within the physician cohort, it is extremely unlikely that a patient would be counted twice in this analysis.
Study Outcomes
Physician-completed patient record forms (PRFs) were completed online after a consultation. Data collected from the PRFs included patient demographics, comorbid conditions and medications. Clinical profiles, including Myasthenia Gravis Foundation of America (MGFA) classification, and symptom type and severity, were reported at diagnosis and at time of survey completion. Symptoms were checked from a pre-selected list. “Ocular myasthenia”, “ptosis” and “diplopia” were all separate options during data collection. Ocular myasthenia was defined as “general weakness of the eye muscles”, ptosis was defined as “drooping of one or both eyelids” and diplopia was defined as “blurred or double vision”. Treatment, defined as “ever treated” or “current treatment” at time of survey completion, included both acute and chronic treatments. Acute treatment was described in the PRF as “rescue or acute treatments”, and options were intravenous immunoglobulin (IVIg), subcutaneous immunoglobulin (SCIg), high-dose steroids, plasmapheresis, and a free text option for “other”. The PRF also collected data on duration of treatment, reasons for treatment choice, physician management and involvement, and hospitalizations. “Don’t know” was a valid response to questions on symptom onset, diagnosis, and number and type of consultations.
Statistical Analysis
Data were analyzed using UNICOM® Intelligence Reporter version 7.5 (UNICOM Systems, Inc., Mission Hills, CA, USA). Categorical values are reported as frequencies and percentages. Continuous values are reported as mean and standard deviation (SD).
Results
Patient Demographics and Comorbidities
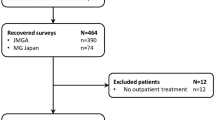
Between March and July 2020, 456 PRFs were completed by 78 physicians based in the US. Most of these physicians were neurologists (63%, n = 49) and the remainder were general physicians (37%, n = 29), with a mean (SD) proportion of 13.8% (18.11) of their professional time spent managing patients with MG.
Not all questions were completed in all PRFs due to logic routing, and as a result there was variation in the total number of patients per variable. Physician-reported patient demographics are shown in Table 1. The overall mean age at the time of survey completion was 54.5 years and 53.1% (n = 242) of patients were male. Nearly three-quarters of patients had one or more comorbidities (73.2%, n = 334) and, of these, over one-third (34.4%, n = 157) listed hypertension as a comorbidity, followed by dyslipidemia (21.7%, n = 99) and anxiety (18.6%, n = 85). Among patients who had one or more comorbidities (n = 334), 88.3% (n = 295) took medication for their concomitant condition(s). Additionally, 9.4% (n = 43) of patients also took over-the-counter medications or herbal supplements alongside their MG or concomitant treatment. There was a mean total of 2.9 prescribed and non-prescribed medications taken per person for all conditions. Statins (38.3%, n = 128) were the most commonly prescribed medications for comorbidities, followed by antidepressants (31.1%, n = 104) and angiotensin II receptor blockers (24.3%, n = 81).
Clinical Profile
The mean age at MG symptom onset was 50.1 years (n = 362), with a mean time from symptom onset to diagnosis of 9.0 months (274.0 days, n = 357) and a mean time since MG diagnosis of 42.8 months (1297.6 days, n = 419). Mean time from symptom onset to first consultation was 4.8 months (146.5 days, n = 341) and mean time from symptom-related consultation to diagnosis was 3.9 months (118.7 days, n = 361; Table 2). Diagnosing physicians were predominantly neurologists (76.1%, n = 347), after initial consultation by a primary care physician (53.9%, n = 246). Almost one-fifth of patients (19.3%, n = 88) were initially misdiagnosed with another condition, most commonly chronic fatigue syndrome, which accounted for over one-third (37.5%, n = 33) of misdiagnoses (Table 3).
At time of survey completion, the mean number of symptoms experienced by each patient was five, with the top five current symptoms reported as ocular myasthenia (53.3%, n = 243), ptosis (49.3%, n = 225), general fatigue (47.1%, n = 215), weakness in the arms (36.6%, n = 167) and diplopia (31.1%, n = 142; Table 2). Nearly half of patients (49.7%, n = 222) were experiencing weakness in their arms, legs, hands or fingers and, of these 222 patients, just over half (52.3%, n = 116) had moderate-to-severe symptoms. General fatigue was also experienced by around half of patients (47.1%, n = 215), of whom 59.5% (n = 128) were moderately or severely affected.
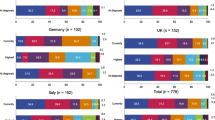
At diagnosis, 66.7% (n = 304) of patients had more than just ocular symptoms (MGFA Class II–V) indicating generalized MG, and at time of survey completion this proportion was 80.8% (n = 367) of patients. At any point from a confirmed MG diagnosis until time of survey completion, 41.0% (n = 187) of patients were classified with MGFA Class III or above, meaning that they had experienced moderate-to-severe weakness of limb, axial, oropharyngeal and/or respiratory muscles (Fig. 1).

MGFA classifications at diagnosis, currentlya, and the highest. aAt time of survey completion. MGFA Myasthenia Gravis Foundation of America
Treatment
Most patients had been prescribed treatment over the course of their disease; 4.8% (n = 22) of patients had never received any prescribed treatment for their MG. Of patients who had one or more moderate-to-severe symptom at time of survey completion (n = 233), 51.5% (n = 120) had received chronic (maintenance) therapy only, 2.6% (n = 6) had received acute treatment only, 42.1% (n = 98) had received both chronic and acute therapy, whilst 3.8% (n = 9) had received neither. Of the nine patients untreated and experiencing a moderate-to-severe symptom, eight patients were classified as MGFA Class IIa or higher. At time of survey completion, 92.5% of patients were receiving treatment.
Of the 233 patients who were still experiencing moderate-to-severe symptoms, 87.6% (n = 204) were receiving chronic treatment, 12.4% (n = 29) were receiving acute treatment (alongside chronic or alone) and 10.3% (n = 24) were not receiving any treatment (Table 4).
Chronic Treatment
The acetylcholinesterase inhibitor (AChEI) pyridostigmine was the most prescribed current chronic treatment (67.6%, n = 254; Fig. 2a), mostly chosen for the known symptomatic improvements in mobility (51.3%, n = 182). AChEIs and/or steroids were the most frequently prescribed first-line treatment type among patients with moderate-to-severe symptoms at time of survey completion (77.9%, n = 159), followed by second-line non-steroidal IST alone (47.1%, n = 96). In general, patients with higher MGFA classifications were receiving later-line treatments: Patients with moderate-to-severe symptoms and MGFA Class I–IIb (n = 129) were mostly prescribed AChEIs and/or steroids (47.3%), while for MGFA Class IIIa and above (n = 75), the most prescribed treatment was non-steroidal IST (62.7%; Fig. 2b). Patients with a higher MGFA class had a greater number of maintenance treatments prescribed at time of survey completion, although patient numbers were much lower in the higher MGFA classes (Supplementary Material [Fig. 2]).

Most prescribed chronic treatments (currenta). a Top 10 most prescribed chronic treatments (n = 376). b Most prescribed chronic treatments by MGFA class among patients with ≥ 1 moderate-to-severe symptom (n = 223). aAt time of survey completion. AChEI acetylcholinesterase inhibitor, Ig immunoglobulin, IST immunosuppressive treatment, IVIg intravenous immunoglobulin, MGFA Myasthenia Gravis Foundation of America, PLEX plasma exchange
On average, patients received their previous treatment for 25.6 months (775.7 days) before switching or stopping (n = 46). The most common reason for switching or stopping therapy was diminished effect over time (45.1%, n = 55); other reasons included risk factors and side effects (Fig. 3a). Physicians reported diminishing efficacy as the biggest driver of patient dissatisfaction with treatment overall (42.0%, n = 66; Fig. 3b). Physicians reported that 72.1% (n = 285) of patients were fully adherent to their medication; however, of the 26.6% (n = 105) who were not entirely adherent, some patients had issues remembering (29.5%, n = 31) or believed that they only needed to take medication when their symptoms worsened (27.6%, n = 29). Considering this, physicians perceived 89.8% (n = 335) of patients to be at least somewhat satisfied with their current maintenance treatment, which corroborated with 80.2% of patients self-reporting to be at least somewhat satisfied with their current treatment (n = 243 of 303 patients on current treatment with a confirmed patient self-completion form).

Treatment perceptions in MG patients. a Top five reasons for switching from previous chronic treatment (n = 122). b Top five factors driving lack of satisfaction (n = 157). MG myasthenia gravis
Acute Treatment
In total, 7.9% (n = 36) of patients were receiving acute treatment at time of survey completion, while 36.0% (n = 164) of patients had previously received acute treatment (Table 5). On average, among patients who received IVIg and SCIg courses as acute treatment, the average number of courses in the last 12 months from time of survey completion were 1.9 (n = 68) and 1.5 (n = 13), respectively. High-dose steroids (38.9%, n = 14) and IVIg (36.1%, n = 13) were the most prescribed acute treatments. The most common reasons for prescribing acute treatment were exacerbations or myasthenic crises, but some patients received acute treatment as bridging therapy while waiting for slow-onset maintenance or chronic therapy to work, or because they did not respond to maintenance or chronic therapy. At time of survey completion, only one patient was using IVIg or SCIg as bridging therapy. In total, 62.5% (n = 285) of patients had never received an acute treatment.
HCRU
On average, 2.5 HCPs were involved in patient management and 5.0 consultations were made per patient, across all HCPs, over the previous 12 months (Table 6, n = 456). Patients in higher MGFA classes consulted more frequently with HCPs of different specialties in the last 12 months.
In the 12 months prior to survey, 15.1% (n = 69) of all patients were hospitalized at least once. Of those patients, 60.9% (n = 42) were admitted, at least once, through the emergency room and 23.2% (n = 16) spent time in an intensive care unit. Across these patients’ admissions, the most common reason was to treat a complication (undefined; 37.7%, n = 26), followed by receiving IVIg (21.7%, n = 15). Among the 69 patients admitted to hospital, 59.4% (n = 41) required at least one stay overnight, with a mean hospital length of stay of 6.8 nights (Table 7). Patients with a current MGFA classification of Class IVb had the longest average stay in hospital in the previous 12 months with a mean of 19 nights (n = 3, Table 7).
Discussion
Drawing on a real-world sample of consulting physicians and presenting patient populations, these data obtained from the Adelphi Real World MG DSP provided valuable insights into the management of MG in the US.
Our data show that, on average, patients waited approximately 9 months for a diagnosis from their onset of symptoms, which could have left them untreated and thus at risk of acute deterioration of symptoms and development of myasthenic crisis [20, 21]. Delays in diagnosis can be due to the fluctuating nature of MG symptoms, making MG difficult to diagnose on clinical examination. Diagnoses may also be missed in primary and non-neurology specialist care as patients can have normal serology and electrophysiology results, particularly in ocular MG, suggesting there is a need for education in primary care and of non-neurology specialists, and more reliable methods of detection [20, 21]. Some patients also experienced unnecessary, non-specific investigations, leading to a mean delay of approximately 5 months from first symptom to consultation with a specialist consultant. MG is also under-recognized in elderly patients due to symptoms such as fatigue and slurred speech falling under broader illness symptoms and thus patients only being referred to non-specialist clinicians [21]. Our study found that approximately 1 in 5 patients were initially misdiagnosed, which may have increased the burden of disease for patients [20].
The number of symptoms reported at diagnosis and after treatment was used as a measure of impact of treatment on disease burden, and as the mean number of symptoms per patient was the same after treatment as it was at diagnosis, many patients may still have been impacted by various aspects of the disease, despite treatment. This suggests that treatment does not necessarily reduce patient burden, even though some of these symptoms will be different than at diagnosis. This is supported by several studies highlighting the fact that many people with generalized MG still report a negative impact of disease or treatment and report fatigue [22, 23], muscle weakness, anxiety and depression, despite receiving treatment [24,25,26,27,28,29,30]. However, whilst many of the symptoms were MG-specific, some such as general fatigue could also be attributed to other comorbidities. Ocular myasthenia was found to be the most frequently reported symptom and general fatigue was the most “troublesome” symptom, with 60% of symptoms at time of survey completion reported as moderate or severe. The burdensome nature of general fatigue may be common, as observational studies report a similar correlation between the increase in disease severity and an increase in fatigue score [31, 32]. The proportion of patients with more than just ocular symptoms (MGFA Class II–V) increased following diagnosis and throughout the course of disease, demonstrating progression from ocular MG to generalized MG, which is likely to negatively impact patients’ quality of life [2].
Among patients with moderate-to-severe MG (MGFA Class III and above) nonsteroidal ISTs were the most prescribed treatment class, while one-third of patients in these classes required chronic steroids. In addition, over one-third of the patients in our survey required acute treatment at some point, predominantly for the treatment of exacerbations or myasthenic crisis, highlighting the lack of disease control with current maintenance treatments or regimens. About 10% of patients have also used acute treatment as bridging therapy due to slow onset of action of some available maintenance or chronic therapies. This finding supports data from the US medical claims database (IBM® MarketScan® Commercial Claims and Encounters) showing that, while receiving AChEI and/or steroids, 27% of patients experienced exacerbations and, of these, 38% of patients required IVIg rescue therapy [10]. Patients with more severe disease require more consultations and have more hospital admissions, placing additional burden on patients and healthcare resources, while disease burden is further exacerbated by limitations of current treatment, such as toxicity and delayed onset of action [32].
The development of new agents with selective immunological targets and rapid onset of action, such as complement inhibitors (eculizumab, ravulizumab, zilucoplan) and neonatal Fc receptor blockers (efgartigimod, rozanolixizumab, nipocalimab) that, while real-world clinical experience is needed to understand whether these drugs will fulfil their potential, may help to resolve these limitations of current treatments and, ultimately, have a positive impact on the burden of disease in patients with MG [32]. In addition, increased use of SCIg in place of IVIg may be beneficial to reducing hospital admissions for IVIg. In our survey, the second most common reason (21.7%) for hospital admissions was for receiving IVIg, thus self-administered treatment at home may help to reduce this burden for both patients and the healthcare system. Continued disease burden and high healthcare cost is, unfortunately, a familiar issue in the US. Real world data on treatment patterns and HCRU show high burden and high cost for a wide range of diseases [33,34,35], and while the development of new MG treatment options is therefore of benefit, they are unlikely to fully resolve the issues identified in our study.
Inherent limitations to data collection via questionnaires apply to this study, including missing fields and answers dependent on either physicians’ perception or patients’ memory. As a result, there was some variation in the total number of patients per variable. Data capture was dependent on patients presenting within the fieldwork time frame, in which, while generating data for a range of patients across treatment types and disease stage, some patients may have consulted or presented more frequently than others. In addition, not all physicians in this survey were neurologists, and, therefore, the practices of primary care physicians or geriatricians may have not been fully representative of how MG is treated by specialists, especially in more complex cases. However, minimal inclusion criteria and the inclusion of non-neurologists aim to ensure that a broad population of physicians, other HCPs and patients, and therefore perspectives, is captured. Physician and patient participation is influenced by willingness to participate in the research and practical considerations of geographic location. In addition, our aim was to give a broad picture of MG patients in general, not only those treated at specialized centers. Follow-up studies of this nature that dive deeper into specialist providers and patient subpopulations will be even more beneficial. Patient-reported outcomes are a useful measure to assess the impact of treatment, however, due to the nature of this point-in-time study, patient-reported outcomes were only collected at the time of the survey and were not captured at diagnosis for a comparison to before MG treatment initiation. The majority of the patients included in our survey were reported to have at least one comorbidity, a small proportion of whom were using over-the-counter medication or supplements in addition to their MG treatment. Some of these over-the-counter medications, such as quinine and magnesium, have been shown in some instances to exacerbate MG [36]. In addition, the mean age at diagnosis was relatively high compared with the expected age of MG onset, [37, 38]. Thus, it is possible that a subgroup analysis of a younger population with fewer comorbidities may have yielded different results. Furthermore, with the data collection occurring during the 2020 coronavirus pandemic, face-to-face consultations may have been restricted and healthcare resources reduced. Finally, as MGFA classification is used predominantly in clinical trials and not routinely in clinical practice, the applicability of the disease severity data may be limited.
Despite these limitations, real-world studies in MG are vital for the understanding of the impact of disease burden on patients living with MG.
Conclusions
Overall, these real-world data suggest that a proportion of patients with MG in the US had a significant need for improved disease management. This is consistent with additional real-world evidence from US claims databases that has identified an unmet need for improved treatment options in MG to reduce the disease burden placed upon patients and healthcare resources.
References
Bacci ED, Coyne KS, Poon JL, Harris L, Boscoe AN. Understanding side effects of therapy for myasthenia gravis and their impact on daily life. BMC Neurol. 2019;19(1):335.
Szczudlik P, Sobieszczuk E, Szyluk B, Lipowska M, Kubiszewska J, Kostera-Pruszczyk A. Determinants of quality of life in myasthenia gravis patients. Front Neurol. 2020;11: 553626.
Gilhus NE, Tzartos S, Evoli A, Palace J, Burns TM, Verschuuren J. Myasthenia gravis. Nat Rev Dis Primers. 2019;5(1):30.
Juel VC, Massey JM. Myasthenia gravis. Orphanet J Rare Dis. 2007;2(1):44.
Melzer N, Ruck T, Fuhr P, Gold R, Hohlfeld R, Marx A, et al. Clinical features, pathogenesis, and treatment of myasthenia gravis: a supplement to the Guidelines of the German Neurological Society. J Neurol. 2016;263(8):1473–94.
Howard JF Jr. Myasthenia gravis: the role of complement at the neuromuscular junction. Ann N Y Acad Sci. 2018;1412(1):113–28.
Bubuioc AM, Kudebayeva A, Turuspekova S, Lisnic V, Leone MA. The epidemiology of myasthenia gravis. J Med Life. 2021;14(1):7–16.
Gilhus NE, Verschuuren JJ. Myasthenia gravis: subgroup classification and therapeutic strategies. Lancet Neurol. 2015;14(10):1023–36.
Berrih-Aknin S, Claeys KG, Law N, Mantegazza R, Murai H, Saccà F, et al. Patient-reported impact of myasthenia gravis in the real world: protocol for a digital observational study (MyRealWorld MG). BMJ Open. 2021;11(7): e048198.
Mahic M, Zaremba P, Rudnik J, Bozorg A, Dolin P. Currently used therapies for myasthenia gravis do not provide adequate disease control for all patients: a retrospective analysis of United States claims data. Am Assoc Neuromusc Electrodiagn Med. 2021;2021:5.
Cutter G, Xin H, Aban I, Burns TM, Allman PH, Farzaneh-Far R, et al. Cross-sectional analysis of the Myasthenia Gravis Patient Registry: disability and treatment. Muscle Nerve. 2019;60(6):707–15.
Mantegazza R, Antozzi C. When myasthenia gravis is deemed refractory: clinical signposts and treatment strategies. Ther Adv Neurol Disord. 2018;11:1756285617749134.
Schneider-Gold C, Hagenacker T, Melzer N, Ruck T. Understanding the burden of refractory myasthenia gravis. Ther Adv Neurol Disord. 2019;12:1756286419832242.
Guptill JT, Sharma BK, Marano A, Soucy A, Krueger A, Sanders DB. Estimated cost of treating myasthenia gravis in an insured US population. Muscle Nerve. 2012;45(3):363–6.
Xin H, Harris LA, Aban IB, Cutter G. Examining the impact of refractory myasthenia gravis on healthcare resource utilization in the United States: analysis of a myasthenia gravis foundation of America Patient Registry sample. J Clin Neurol. 2019;15(3):376–85.
Landfeldt E, Pogoryelova O, Sejersen T, Zethraeus N, Breiner A, Lochmuller H. Economic costs of myasthenia gravis: a systematic review. Pharmacoeconomics. 2020;38(7):715–28.
Anderson P, Benford M, Harris N, Karavali M, Piercy J. Real-world physician and patient behaviour across countries: Disease-Specific Programmes—a means to understand. Curr Med Res Opin. 2008;24(11):3063–72.
Babineaux SM, Curtis B, Holbrook T, Milligan G, Piercy J. Evidence for validity of a national physician and patient-reported, cross-sectional survey in China and UK: the Disease Specific Programme. BMJ Open. 2016;6(8): e010352.
Higgins V, Piercy J, Roughley A, Milligan G, Leith A, Siddall J, et al. Trends in medication use in patients with type 2 diabetes mellitus: a long-term view of real-world treatment between 2000 and 2015. Diabetes Metab Syndr Obes. 2016;9:371–80.
National Institute of Health. Myasthenia gravis fact sheet. 2020. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Myasthenia-Gravis-Fact-Sheet.
Spillane J, Higham E, Kullmann DM. Myasthenia gravis. BMJ Br Med J. 2012;345: e8497.
Elsais A, Wyller VB, Loge JH, Kerty E. Fatigue in myasthenia gravis: is it more than muscular weakness? BMC Neurol. 2013;13:132.
Hoffmann S, Ramm J, Grittner U, Kohler S, Siedler J, Meisel A. Fatigue in myasthenia gravis: risk factors and impact on quality of life. Brain Behav. 2016;6(10): e00538.
Andersen JB, Gilhus NE, Sanders DB. Factors affecting outcome in myasthenia gravis. Muscle Nerve. 2016;54(6):1041–9.
Basta IZ, Pekmezović TD, Perić SZ, Kisić-Tepavčević DB, Rakočević-Stojanović VM, Stević ZD, et al. Assessment of health-related quality of life in patients with myasthenia gravis in Belgrade (Serbia). Neurol Sci. 2012;33(6):1375–81.
Boldingh MI, Dekker L, Maniaol AH, Brunborg C, Lipka AF, Niks EH, et al. An up-date on health-related quality of life in myasthenia gravis—results from population-based cohorts. Health Qual Life Outcomes. 2015;13:115.
Jeong A, Min J-H, Kang YK, Kim J, Choi M, Seok JM, et al. Factors associated with quality of life of people with Myasthenia Gravis. PLoS ONE. 2018;13(11): e0206754.
Masuda M, Utsugisawa K, Suzuki S, Nagane Y, Kabasawa C, Suzuki Y, et al. The MG-QOL15 Japanese version: validation and associations with clinical factors. Muscle Nerve. 2012;46(2):166–73.
The CIE. Final report: The cost to patients and the community of myasthenia gravis. 2013. https://www.mgaq.org.au/sites/default/files/2020-02/CIE_Final_Report.pdf?.
Twork S, Wiesmeth S, Klewer J, Pöhlau D, Kugler J. Quality of life and life circumstances in German myasthenia gravis patients. Health Qual Life Outcomes. 2010;8:129.
Ruiter AM, Verschuuren JJGM, Tannemaat MR. Prevalence and associated factors of fatigue in autoimmune myasthenia gravis. Neuromuscul Disord. 2021;31(7):612–21.
Menon D, Barnett C, Bril V. Novel treatments in myasthenia gravis. Front Neurol. 2020;11:538.
Copher R, Kee A, Gerds A. Treatment patterns, health care resource utilization, and cost in patients with myelofibrosis in the United States. Oncologist. 2022;27(3):228–35.
Fowler NH, Chen G, Lim S, Manson S, Ma Q, Li FY. Treatment patterns and health care costs in commercially insured patients with follicular lymphoma. J Health Econ Outcomes Res. 2020;7(2):148–57.
Lu M, Goodwin B, Vera-Llonch M, Williams J. Disease burden and treatment patterns associated with eosinophilic esophagitis in the United States: a retrospective claims study. J Clin Gastroenterol. 2022;56(2):133–40.
Sheikh S, Alvi U, Soliven B, Rezania K. Drugs that induce or cause deterioration of myasthenia gravis: an update. J Clin Med. 2021;10(7):1537.
Cortes-Vicente E, Alvarez-Velasco R, Segovia S, Paradas C, Casasnovas C, Guerrero-Sola A, et al. Clinical and therapeutic features of myasthenia gravis in adults based on age at onset. Neurology. 2020;94(11):e1171–80.
Guastafierro E, Tramacere I, Toppo C, Leonardi M, Mantegazza R, Bonanno S, et al. Employment in myasthenia gravis: a systematic literature review and meta-analysis. Neuroepidemiology. 2020;54(4):304–12.
Acknowledgements
The authors would like to thank the patients, healthcare professionals, and caregivers who contributed to this study.
Funding
Data collection was undertaken by Adelphi Real World as part of an independent survey, entitled the Adelphi Real World Myasthenia Gravis Disease Specific Programme™ (DSP). UCB Pharma did not influence the original survey through either contribution to the design of questionnaires or data collection. The analysis described here used data from the Adelphi Real World Myasthenia Gravis DSP. The DSP is a wholly owned Adelphi product. UCB Pharma is one of multiple subscribers to the DSP. UCB Pharma funded this study and the journal’s Rapid Service Fee.
Medical Writing and Editorial Assistance
Medical writing support was funded by UCB Pharma, provided by Rachel Price PhD, of Ogilvy Health UK, on behalf of Adelphi Real World and UCB Pharma, in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). The authors thank Veronica Porkess PhD, of UCB Pharma, for publication and editorial support.
Authorship
All named authors meet the International Committee of Medical Journal Editors criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Milada Mahic contributed to the study concept, design and interpretation of the data. Anna Scowcroft, Tyler Story and Angela Ting contributed to the interpretation of the data. Ali Bozorg contributed to the study design and interpretation of the data. Keisha Golden, Gregor Gibson, Jonathan DeCourcy and Christian Taylor contributed to the data collection and interpretation of the data. All authors critically reviewed each draft of the manuscript and approved the submitted version.
Disclosures
Milada Mahic is a former employee of UCB Pharma and is now employed by Vertex Pharmaceuticals. Ali M. Bozorg is a former employee of UCB Pharma and is now employed by Otsuka Pharmaceutical Development and Commercialization, Inc. Anna Scowcroft, Angela Ting and Tyler J. Story are employees and stockholders of UCB Pharma. Keisha J. Golden, Gregor A. Gibson, Jonathan J. DeCourcy are employees of Adelphi Real World. Christian F. Taylor is a former employee of Adelphi Real World and does not currently have an affiliation to any organization.
Compliance with Ethics Guidelines
This survey obtained ethics approval from the Western Institutional Review Board, sponsor protocol number: AG8768. The Disease Specific Programme™ is Health Insurance Portability and Accountability Act compliant, and all data was aggregated and de-identified. Patients and physicians provided informed consent to take part in the Adelphi Myasthenia Gravis Disease Specific Programme™ market research survey, on which this secondary data analysis is based. Data were collected in such a way that patients and physicians could not be identified directly.
Data Availability
All data, including methodology, materials, data, and data analysis, that support the findings of this survey are the intellectual property of Adelphi Real World. All requests for access should be addressed directly to Jonathan DeCourcy (jonathan.decourcy@adelphigroup.com).
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Mahic, M., Bozorg, A.M., DeCourcy, J.J. et al. Physician-Reported Perspectives on Myasthenia Gravis in the United States: A Real-World Survey. Neurol Ther 11, 1535–1551 (2022). https://doi.org/10.1007/s40120-022-00383-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40120-022-00383-3