
Abstract
Introduction
Persistence and adherence to psoriasis treatments reflect overall drug effectiveness, tolerability, and convenience. Limited data are available on the treatment patterns of ixekizumab, an interleukin (IL)-17A antagonist, vs. guselkumab, an IL-23 inhibitor. Our objective was to evaluate real-life psoriasis drug treatment patterns with ixekizumab vs. guselkumab.
Methods
This retrospective observational study used United States insurance claims data from IBM Watson MarketScan Databases to analyze treatment patterns (including adherence, persistence, time on monotherapy, switching, and use of concomitant medications) for patients with 1 year, ≥ 6 months, and up to 30 months of follow-up. Outcomes were compared between ixekizumab and guselkumab on the balanced sample after applying inverse probability of treatment weighting (IPTW).
Results
Data for 1414 eligible patients (ixekizumab, N = 674 and guselkumab, N = 740) were assessed. Over the 1-year follow-up, adherence was greater for ixekizumab vs. guselkumab when evaluated by proportion of days covered ≥ 80% [odds ratio (OR) 1.77 (95% confidence interval, 1.41, 2.21), p < 0.001] and by medication possession ratio ≥ 80% [OR = 1.92 (1.54, 2.38), p < 0.001]. Persistence was longer for ixekizumab vs. guselkumab with a 60-day allowable gap [non-persistence hazard ratio (HR) (95% confidence interval): 0.80 (0.69, 0.93), p = 0.005], but there were no differences with a 90-day allowable gap [HR = 0.98 (0.83, 1.17), p = 0.850]. Results assessed in patients with ≥ 6 months follow-up confirmed these findings. This retrospective analysis of a United States claims database used prescription refill data to estimate persistence/adherence.
Conclusions
Based on real-world evidence using claims data, patients with psoriasis treated with ixekizumab had a greater adherence to and an equal or greater persistence with therapy vs. patients treated with guselkumab.
Plain Language Summary
In real-world settings, how consistently patients take a drug (adherence) and how long they continue taking it (persistence) are thought to reflect patients’ satisfaction with the combination of efficacy and tolerability of the treatment. In this study of patients with psoriasis, we compared these measures—regularity of prescription refills and continued time on drug—between patients receiving ixekizumab or guselkumab for their psoriasis. This information was taken from a large insurance claims database, and so reflects results among commercially insured patients in the United States. We found that patients taking ixekizumab more consistently obtained prescription refills during the study period. Patients taking ixekizumab or guselkumab continued treatment for similar lengths of time when we allowed a longer gap of 90 days between prescription refills, but when a shorter gap of 60 days was allowed, those on ixekizumab spent a longer time on treatment. The findings were consistent regardless of prior treatment with other similar drugs (biologics). Overall, these findings indicate that for ixekizumab, which is dosed once every 4 weeks, and guselkumab, which is dosed once every 8 weeks, patients took ixekizumab more regularly and continued on the drug for about the same or a longer amount of time compared to patients taking guselkumab. These results may help dermatology practitioners in selecting biologic drugs for their patients with psoriasis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
To gather information on real-world persistence with and adherence to psoriasis therapies, which reflect overall drug effectiveness, tolerability, and convenience in clinical practice. |
More specifically, limited data are available on persistence with and adherence to ixekizumab vs. guselkumab. |
What did the study ask? |
What are the treatment patterns observed in a large insurance claims database in patients with psoriasis treated with ixekizumab (dosed every 4 weeks) vs. guselkumab (dosed every 8 weeks) over 1 year? |
What was learned from the study? |
In this retrospective observational study, psoriasis patients (N = 1414) with at least 1 year of follow-up who were treated with ixekizumab had greater adherence to and equal or greater persistence with therapy (depending on the allowable treatment gap) compared to patients who were treated with guselkumab. |
This study offers insight into real-world treatment patterns of ixekizumab vs. guselkumab in a more diverse patient population than randomized, controlled clinical trials. |
Introduction
Moderate-to-severe psoriasis generally requires lifelong treatment, and continuous therapy is needed to maintain disease control. Lack of adherence, resulting in decreased frequency of administration or interruption of therapy, is associated with the recurrence of symptoms, commonly within 2–5 months [1,2,3,4]. In addition, up to 50% of patients starting tumor necrosis factor inhibitors may discontinue within 12 months [5,6,7,8]. Notably, the rate of treatment discontinuation and switching for all biologics is substantially higher in patients previously treated with biologics vs. biologic-naïve subjects [5, 7, 8], and treatment persistence appears to decline with additional prior biologic therapies [9]. Finally, treatment failure and switching are reported to be associated with increased use of health care services [10,11,12,13].
Ixekizumab, an interleukin (IL)-17A inhibitor approved for use in adult patients with moderate-to-severe psoriasis, has demonstrated long-term efficacy and safety up to 5 years [14, 15], and has generally shown drug persistence equal to or greater than that of other biologics for psoriasis [7, 9, 16,17,18]. Guselkumab, an IL-23p19 inhibitor also approved for psoriasis, has demonstrated efficacy and safety through 4 years [19]. Of note, the efficacy and safety of ixekizumab and guselkumab were compared in a head-to-head trial that demonstrated a faster initial response to ixekizumab through 12–16 weeks but generally comparable levels of response at 24 weeks [20, 21]. However, to date, long-term adherence to and persistence with ixekizumab have not been compared in clinical practice settings to any of the 3 currently approved IL-23 inhibitors, including guselkumab. Here, using real-world administrative claims data, we compared ixekizumab and guselkumab in terms of adherence to and persistence with therapy, days on monotherapy, days on concomitant therapy, and rates of discontinuation and switching.
Methods
Data Source
This analysis assessed data from the IBM Watson Health MarketScan® Commercial Encounters, Medicare Supplemental, and Monthly Early View Databases. The Commercial Encounters database contained records for inpatient, outpatient, and outpatient prescription drug claims for employees and their dependents covered under fee-for-service and managed care health plans; the Medicare Supplemental database contained similar data for retirees with employer-paid Medicare supplemental insurance. Early View included similar data to both databases for the period from May 1, 2019 to July 31, 2020. Data were identified using enrollment records, service dates, International Classification of Diseases, 9th and 10th Revision, Clinical Modification (ICD-9-CM and ICD-10-CM) diagnosis codes, Current Procedural Technology 4th edition (CPT-4®) codes, Healthcare Common Procedure Coding System (HCPCS) codes, and National Drug Codes (NDCs), as needed. As all data were anonymized, no ethics committee approval was needed for these analyses.
Patients
Eligible patients had at least 1 inpatient or 2 outpatient claims (at least 30 days apart) with a diagnosis of psoriasis (ICD-9-CM diagnosis code 696.1x or ICD-10-CM diagnosis codes L40.0–L40.4 or L40.8) between July 1, 2017 and December 31, 2018 (the indexing period). The study sample includes patients with ≥ 1 claim for ixekizumab or for guselkumab after the first psoriasis diagnosis.
The date of the first prescription for ixekizumab or guselkumab during the indexing period was the index date. Patients were required to have medical and benefit enrollment data for a minimum of 6 months pre-index and, for the primary analysis, a minimum 1-year follow-up (≥ 6-months follow-up for the secondary analysis). Patients could have no diagnosis for other conditions indicated for ixekizumab (psoriatic arthritis, ankylosing spondylitis) or guselkumab (psoriatic arthritis) or a prescription for the index drug during the pre-index period. Study follow-up was censored at the first among study end, health insurance plan enrollment end, and death. Patients were classified as receiving prior biologics if they received biologics with an indication for psoriasis in the 6-month pre-index period. For patients who received both drugs during the study period, the first drug was considered to be the only index drug, and they were then considered to have either discontinued or switched, depending upon the gap between receiving the drugs.
Treatment Patterns
Treatment pattern outcomes, including treatment persistence, discontinuation, switching, reinitiation, and adherence, were assessed during the follow-up period based on filled prescriptions. Treatment adherence based on actual use of the index medication without counting treatment gaps and treatment persistence based on a < 60-day or < 90-day allowable gap through the 1-year follow-up were analyzed. Treatment adherence was measured by proportion of days covered (PDC) and medication possession ratio (MPR) during follow-up. PDC and MPR were each defined as the number of days’ supply divided by the total number of days during the follow-up period; when the periods covered by consecutive fills overlapped, PDC counted the actual or concurrently covered days while MPR counted all days supplied. High adherence was defined as MPR or PDC ≥ 80%.
Treatment persistence was defined as a prescription refill within < 60 or < 90 days of the last day of supply [22]. For example, for a 60-day gap (assuming no overlap with the last prescription), counting for the treatment gap for ixekizumab would start the first day after the 4-week dosing period (day 29) that started with the prescription fill. The patient would be considered nonpersistent if no refill was recorded between day 29 and day 89 (29 plus 60 days). For guselkumab, counting for the gap would start at the first day after the 8-week dosing period (day 57), and the patient would be considered nonpersistent with no refill by day 117. For a 90-day gap, these would correspond to no prescription fills between day 29 and day 119 for ixekizumab and day 57 and day 147 for guselkumab. The end date of persistence was defined as the last day’s supply of the prescription before the permissible gap. A gap of 45 days has also been considered in previous assessments of treatment persistence [23, 24], and was assessed in this study as a sensitivity analysis.
Drug discontinuation was defined as a treatment gap of ≥ 90 days based on prior claims-based studies of biologic discontinuation [24,25,26]. Reinitiation was defined as a new claim for the index drug after meeting the criteria for discontinuation and not switching to other therapies. Switching from the index therapy was defined as when a new medication was prescribed, and the days’ supply of the new therapy (other biologics, systemic therapy, phototherapy) extended beyond the last day supplied by the index medication. The percentages of patients who discontinued, reinitiated, or switched from the index drug were reported.
Statistical Analysis
Patient demographics included age, sex, geographic location, and primary payer and health plan type, and were assessed at the index date. The Deyo–Charlson Comorbidity Index, comorbid conditions (anxiety, cerebrovascular disease, coronary heart disease, depression, diabetes, hyperlipidemia, hypersensitivity, hypertension, lymphoma, multiple sclerosis, obesity, osteoarthritis, other autoimmune disorders, peripheral vascular disease, reactive arthritis, skin cancer, and sleep apnea), and all-cause health care costs were assessed for the 6-month pre-index period. Psoriasis-related medication and treatment usage was also reported for the pre-index period. This included the use of biologic(s) (adalimumab, brodalumab, certolizumab, etanercept, guselkumab, infliximab, ixekizumab, secukinumab, or ustekinumab) and the number of unique biologics, nonbiologic systemic (apremilast, acitretin, systemic steroids, cyclosporine, methotrexate, azathioprine, hydroxyurea, isotretinoin, leflunomide, methoxsalen, mycophenolate mofetil, sulfasalazine, or thioguanine) or topical therapy, and phototherapy. All of these factors were included as covariates in weighting/models as described below.
In order to minimize bias in the comparison between ixekizumab and guselkumab, inverse probability of treatment weighting (IPTW) was employed for the adjustment of baseline heterogeneity between treatment groups. The number of unique biologics during the pre-index period and the covariates (listed above) were included in the IPTW. The balance of cohorts was evaluated using the standardized difference, with a standardized difference of < 0.1 indicating good balance. Unless otherwise specified, weighted data were reported for outcomes.
High adherence (PDC or MPR ≥ 80%) was assessed using logistic regression to calculate odds ratios with confidence intervals and p-values. Persistence was assessed using Kaplan–Meier curves for time to nonpersistence and by Cox proportional hazards regression analysis, reported as the hazard ratio with the 95% confidence interval and the p-value. All variables included in the IPTW model were also included in the models for treatment comparisons. R 3.5.1 software (R Foundation for Statistical Computing, Vienna, Austria) and SAS EG 7.15 software (SAS Institute Inc, Cary, NC) were used for the data analysis in this study.
Results
Patient Selection and Weighting
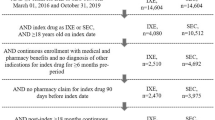
Among the 68,047 patients identified with claims from July 1, 2017 to December 31, 2018, 674 patients receiving ixekizumab and 740 receiving guselkumab satisfied all criteria for inclusion in the primary dataset (Supplementary Fig. 1). Prior to weighting, the ixekizumab and guselkumab groups generally had similar clinical characteristics: mean age was 48.9 and 48.4 years, respectively; the percentage of male patients was 51.8% and 54.3%, respectively; the most common type of health plan was preferred provider organization at 57.4% and 58.5%, respectively; and the Charlson Comorbidity Index was 0.61 vs. 0.51, respectively (Table 1). Ixekizumab patients were, however, more likely to have received previous biologics vs. guselkumab patients (60.4% vs. 49.5%, p < 0.001). Following IPTW, the samples were well matched (Table 1; see Supplementary Table 1 for results based on ≥ 6 months of follow-up).
Medication Adherence
Overall, for the 1-year follow-up population, mean ± standard deviation and median for PDC were 0.65 ± 0.28 and 0.75 for ixekizumab vs. 0.60 ± 0.25 and 0.60 for guselkumab (p < 0.001) (Table 2), which reflected a mean of 236 ± 102 days covered for ixekizumab and 219 ± 92 days covered for guselkumab. The odds ratio (OR) for high adherence of patients receiving ixekizumab (compared to those receiving guselkumab) was 77% higher based on the PDC [OR (95% confidence interval) 1.77 (1.41, 2.21)] and 92% higher based on the MPR [1.92 (1.54, 2.38); both p < 0.001] (Fig. 1). When analyzed in patients with ≥ 6 months of follow-up (and who had a longer median follow-up of up to 30 months), those receiving ixekizumab had 45% higher odds of high adherence based on PDC [OR = 1.45 (1.16, 1.80)] and 51% higher odds based on MPR [OR = 1.51 (1.23, 1.87); both p < 0.001] (Fig. 1). High adherence (defined by either PDC or MPR) remained significantly more likely with ixekizumab vs. guselkumab when compared within the subgroups of biologic experienced and biologic nonexperienced patients (all p < 0.05) (Supplementary Fig. 2).

Drug adherence by follow-up period. Odds ratio of high adherence (defined as PDC ≥ 80% or MPR ≥ 80%) for ixekizumab vs. guselkumab. CI confidence interval, GUS guselkumab, IXE ixekizumab, OR odds ratio, PDC proportion of days covered, MPR medication possession ratio
Treatment Persistence
Persistence with index therapy based on a < 60-day and < 90-day treatment gap is illustrated in Fig. 2 by Kaplan–Meier plots for follow-up periods of 1 year (primary analysis) and a minimum of 6 months (up to a maximum of 30 months). For a 1-year follow-up based on a 60-day allowable gap, a significantly higher percentage of ixekizumab vs. guselkumab patients were persistent at 1 year (56.4% vs. 49.2%, respectively, log-rank p = 0.006). However, when assessed using a 90-day allowable gap, no significant differences were seen between persistence with ixekizumab vs. guselkumab at 1 year (64.2% and 64.3%, respectively; p = 0.845). Hazard ratios (HRs) for nonpersistence allowing a 60-day or 90-day gap and, as a sensitivity analysis, a 45-day gap, are shown in Fig. 3. Patients receiving ixekizumab had a 20% lower hazard of nonpersistence given a 60-day allowable gap [HR = 0.80 (0.69, 0.93), p = 0.005], and a 30% lower hazard given a 45-day allowable gap [HR = 0.70 (0.61, 0.80), p < 0.001]; however, given a 90-day allowable gap, there was no significant difference between ixekizumab and guselkumab [HR = 0.98 (0.83, 1.17), p = 0.850]. When assessed within the slightly larger population with ≥ 6-month follow-up, the hazard of nonpersistence was 20% lower for ixekizumab vs. guselkumab with a 60-day gap [HR = 0.80 (0.70, 0.91), p < 0.001], but was comparable between drugs using the 90-day gap [HR = 1.02 (0.88, 1.18), p = 0.795]. Results obtained given a 45-day gap showed a significant difference between drugs [HR = 0.72 (0.64, 0.82), p < 0.001]. HRs for nonpersistence for ixekizumab vs. guselkumab were generally comparable in biologic experienced vs. nonexperienced patients (data not shown).

Kaplan–Meier analysis of treatment persistence with ixekizumab vs. guselkumab for a < 60-day allowable gap and (a) 1 year or (b) at least 6 months of follow-up, or for a < 90-day allowable gap and (c) 1 year or (d) at least 6 months of follow-up. Data are as observed. Percentages indicate the patients who were continuing the treatment with the index drug. IXE ixekizumab, GUS guselkumab, No. number

Persistence with ixekizumab and guselkumab by allowable treatment gap. Treatment persistence is shown as the hazard ratio for nonpersistence for ixekizumab vs. guselkumab based on a < 45-day (sensitivity analysis), < 60-day, or < 90-day allowable gap. CI confidence interval, HR hazard ratio, IXE ixekizumab
Monotherapy, Discontinuation, Switching, and Concomitant Medications
Through 1 year of follow-up, patients receiving ixekizumab had more mean days on monotherapy (218 vs. 203) and a higher PDC on monotherapy compared to guselkumab (0.60 vs. 0.56, p = 0.001) (Table 2); with concomitant therapies, the PDC did not differ significantly between treatments (p = 0.860). Among patients with a ≥ 6-month follow-up, there was no significant difference in PDC between patients on monotherapy (p = 0.149) and those on concomitant therapies (p = 0.699) (Supplementary Table 2).
The proportion of patients who met the criteria for discontinuation (> 90-day gap) of the study medication in the 1-year follow-up analysis was 35.2% for ixekizumab (4.7% reinitiated ixekizumab, 17.6% switched, and 13.0% discontinued without switching to another drug) vs. 36.2% for guselkumab (8.4% reinitiated guselkumab, 12.9% switched, and 14.9% discontinued without switching to another drug) (Supplementary Table 3). The proportion of patients who met the criteria for discontinuation of the study medication among patients with a ≥ 6-month follow-up was 48.8% for ixekizumab (8.2% reinitiated ixekizumab, 24.1% switched, and 16.5% discontinued without switching to another drug) vs. 48.5% for guselkumab (14.1% reinitiated guselkumab, 16.9% switched, and 17.5% discontinued without switching to another drug) (Supplementary Table 3).
Discussion
Drug adherence and persistence are considered important real-world measures of treatment effectiveness, combining efficacy, safety/tolerability, and convenience [27, 28]. Here, utilizing administrative claims databases, ixekizumab demonstrated greater adherence and similar-to-greater persistence through 1 year of follow-up when compared to guselkumab. These adherence and persistence findings were confirmed in a secondary analysis assessing patients over a variable follow-up period of ≥ 6 months and up to 30 months. Patients receiving ixekizumab had a significantly higher proportion of days covered on monotherapy, with similar rates of concomitant therapies. Switching therapies was more common among patients receiving ixekizumab vs. guselkumab, while the discontinuation rate was similar for ixekizumab and guselkumab.
Adherence to and persistence with treatment in patients with psoriasis have been suggested to correspond roughly to overall treatment success and patient satisfaction, respectively [27, 28]. Adherence to medication assesses the proportion of the study period covered by the index drugs, irrespective of differences in dosing intervals or the specific lengths of gaps in treatment. The likelihood of high adherence, defined either as PDC or MPR ≥ 80%, was significantly greater for ixekizumab vs. guselkumab. This is consistent with the finding of a significantly greater proportion of days covered by the drug overall and as monotherapy for ixekizumab. The proportion of the study period during which patients used concomitant medications was similar for the index drugs.
Overall, patients with psoriasis in clinical practice settings who were treated with ixekizumab had significantly greater persistence with therapy vs. guselkumab when assessed using 45-day and 60-day allowable gaps, but no difference in persistence was observed between groups in the analysis when using a more generous 90-day allowable gap. Previous studies on persistence in psoriasis have used a range of allowable gaps from 45 to 150 days [16, 23, 24], and we have previously reported results for comparisons of ixekizumab and adalimumab or secukinumab based on a 60-day gap [17, 18]. However, a recent analysis of multiple drugs for psoriasis found that persistence estimates for ustekinumab, which has a 12-week dosing interval, varied more widely depending on the allowable treatment gap than other drugs with shorter dosing and refill intervals [16]. Our results are consistent with this finding in that the significance of differences in persistence between ixekizumab, with typical maintenance dosing every 4 weeks, and guselkumab, with typical maintenance dosing every 8 weeks, varied depending upon the length of the allowable gap.
These data add to the body of evidence showing higher treatment adherence to and similar-to-longer treatment persistence with ixekizumab vs. other biologics from previous real-world studies using administrative claims data, where ixekizumab demonstrated better adherence vs. secukinumab [17] and better persistence vs. adalimumab [18] and secukinumab [9, 17]. A longer drug survival vs. other IL-17 inhibitors and other biologics was also shown with ixekizumab using the Corrona (CorEvitas) Psoriasis Registry [8]. Earlier registry studies performed prior to the significant use of ixekizumab have shown mean 1-year persistence rates (based on a 90-day gap) for both first- and second-line biologics of 77% in a British cohort [11, 12], 62% overall in a study assessing the French National Health Insurance database [29], and from 47% (adalimumab) to 79% (ustekinumab) in a Japanese claims study (based on a 60-day gap) [30]. Results from the current study (approximately 64%) using a 90-day gap were generally comparable to or slightly lower than those in the earlier registry studies. Differences in medical coverage/usage in nationalized health systems vs. under commercial insurance in the United States (US), as well as the effect of the availability of additional biologics (which has been shown to increase rates of switching) [31] in the present, more recent study, likely contributed to this finding. In a recent assessment of US insurance claims for a period immediately prior to that assessed in the present report, the 1-year persistence based on a 90-day gap was 59.4% and 60.5% for secukinumab and ustekinumab, respectively [32], which is comparable to the ~ 64% seen for ixekizumab and guselkumab herein. A recent study based on patients in the large North American Corrona Psoriasis Registry compared persistence (based on a 60-day allowable gap) between ixekizumab, non-ixekizumab IL-17 inhibitors, and TNF inhibitors [8]. For ixekizumab, persistence at 1 year was 81% in biologic-naive patients and 65% in biologic experienced patients [8]—rates that, when combined, would be higher than that observed in the present claims-based analysis.
Strengths of the current study include the large sample size, use of multiple measures of treatment adherence, evaluation of key subgroups, and sensitivity analyses using multiple persistence windows. Common to all US claims database analyses, some key patient variables—including psoriasis severity, patient weight, and full treatment history—are not available and therefore could not be used for IPTW adjustment; however, data were adjusted by biologic experience (along with other variables) in the 6-month pre-index period. Limitations include the retrospective nature of the study and the lack of available clinical information such as reason for discontinuation, which are common to all US claims database analyses, and the 1-year follow-up period, which was due to the limited amount of longer-term data available for these 2 relatively new biologics. Adherence and persistence were based on the dispensed date of prescription; it was not known with certainty when or if the patient administered the drug. In addition, we could not address the possibility that a patient could have received a free drug sample, as our analysis was restricted to insurance claims for prescription medication. As the present analyses are based on a US claims database, these results are generalizable to a commercially insured population in the US, but not necessarily to other regions or countries. Finally, although administrative data can help assess adherence and persistence of a treatment, additional studies would be needed to help understand the factors contributing to these outcomes.
Conclusion
In clinical practice settings, ixekizumab patients had greater adherence, equal or greater persistence, and more days on monotherapy at 1-year follow-up than guselkumab. These results may assist dermatology practitioners in selecting biologics for their patients with psoriasis.
References
Brezinski EA, Armstrong AW. Off-label biologic regimens in psoriasis: a systematic review of efficacy and safety of dose escalation, reduction, and interrupted biologic therapy. PloS One. 2012;7(4):e33486.
Blauvelt A, Papp KA, Sofen H, Augustin M, Yosipovitch G, Katoh N, et al. Continuous dosing versus interrupted therapy with ixekizumab: an integrated analysis of two phase 3 trials in psoriasis. J Euro Acad Dermatol Venereol. 2017;31(6):1004–13.
Griffiths CE, Vender R, Sofen H, Kircik L, Tan H, Rottinghaus ST, et al. Effect of tofacitinib withdrawal and re-treatment on patient-reported outcomes: results from a Phase 3 study in patients with moderate to severe chronic plaque psoriasis. J Euro Acad Dermatol Venereol. 2017;31(2):323–32.
Reich K, Armstrong AW, Foley P, Song M, Wasfi Y, Randazzo B, et al. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: results from the phase III, double-blind, placebo- and active comparator-controlled VOYAGE 2 trial. J Am Acad Dermatol. 2017;76(3):418–31.
Egeberg A, Ottosen MB, Gniadecki R, Broesby-Olsen S, Dam TN, Bryld LE, et al. Safety, efficacy and drug survival of biologics and biosimilars for moderate-to-severe plaque psoriasis. Br J Dermatol. 2018;178(2):509–19.
Yiu ZZN, Mason KJ, Hampton PJ, Reynolds NJ, Smith CH, Lunt M, et al. Drug survival of adalimumab, ustekinumab and secukinumab in patients with psoriasis: a prospective cohort study from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR). Br J Dermatol. 2020;183(2):294–302.
Graier T, Salmhofer W, Jonak C, Weger W, Kolli C, Gruber B, et al. Biologic drug survival rates in the era of anti-Il-17 antibodies: a time period-adjusted registry analysis. Br J Dermatol. 2021;184(6):1094–1105.
Lockshin B, Cronin A, Harrison RW, McLean RR, Anatale-Tardiff L, Burge R, et al. Drug survival of ixekizumab, TNF inhibitors, and other IL-17 inhibitors in real-world patients with psoriasis: The Corrona Psoriasis Registry. Dermatol Ther. 2021:e14808.
Egeberg A, Bryld LE, Skov L. Drug survival of secukinumab and ixekizumab for moderate-to-severe plaque psoriasis. J Am Acad Dermatol. 2019;81(1):173–8.
Foster SA, Zhu B, Guo J, Nikai E, Ojeh C, Malatestinic W, et al. Patient characteristics, health care resource utilization, and costs associated with treatment-regimen failure with biologics in the treatment of psoriasis. J Manag Care Spec Pharm. 2016;22(4):396–405.
Iskandar IYK, Warren RB, Lunt M, Mason KJ, Evans I, McElhone K, et al. Differential drug survival of second-line biologic therapies in patients with psoriasis: observational cohort study from the British Association of Dermatologists Biologic Interventions Register (BADBIR). J Invest Dermatol. 2018;138(4):775–84.
Warren RB, Smith CH, Yiu ZZN, Ashcroft DM, Barker J, Burden AD, et al. Differential drug survival of biologic therapies for the treatment of psoriasis: a prospective observational cohort study from the British Association of Dermatologists Biologic Interventions Register (BADBIR). J Invest Dermatol. 2015;135(11):2632–40.
Murage MJ, Anderson A, Casso D, Oliveria SA, Ojeh CK, Muram TM, et al. Treatment patterns, adherence, and persistence among psoriasis patients treated with biologics in a real-world setting, overall and by disease severity. J Dermatolog Treat. 2019;30(2):141–9.
Blauvelt A, Lebwohl MG, Mabuchi T, Leung A, Garrelts A, Crane H, et al. Long-term efficacy and safety of ixekizumab: 5-year analysis of the UNCOVER-3 randomized controlled trial. J Am Acad Dermatol. 2021;85(2):360–8.
Leonardi C, Reich K, Foley P, Torii H, Gerdes S, Guenther L, et al. Efficacy and safety of ixekizumab through 5 years in moderate-to-severe psoriasis: long-term results from the UNCOVER-1 and UNCOVER-2 phase-3 randomized controlled trials. Dermatol Ther (Heidelb). 2020;10(3):431–47.
Hendrix N, Marcum ZA, Veenstra DL. Medication persistence of targeted immunomodulators for plaque psoriasis: a retrospective analysis using a U.S. claims database. Pharmacoepidemiol Drug Saf. 2020;29(6):675–83.
Blauvelt A, Shi N, Burge R, Malatestinic WN, Lin CY, Lew CR, et al. Comparison of real-world treatment patterns among patients with psoriasis prescribed ixekizumab or secukinumab. J Am Acad Dermatol. 2020;82(4):927–35.
Blauvelt A, Shi N, Burge R, Malatestinic WN, Lin CY, Lew CR, et al. Comparison of real-world treatment patterns among psoriasis patients treated with ixekizumab or adalimumab. Patient Prefer Adherence. 2020;14:517–27.
Griffiths CEM, Papp KA, Song M, Miller M, You Y, Shen YK, et al. Continuous treatment with guselkumab maintains clinical responses through 4 years in patients with moderate-to-severe psoriasis: results from VOYAGE 1. J Dermatolog Treat. 2020;1–9.
Blauvelt A, Papp K, Gottlieb A, Jarell A, Reich K, Maari C, et al. A head-to-head comparison of ixekizumab vs. guselkumab in patients with moderate-to-severe plaque psoriasis: 12-week efficacy, safety and speed of response from a randomized, double-blinded trial. Br J Dermatol. 2020;182(6):1348–58.
Blauvelt A, Leonardi C, Elewski B, Crowley JJ, Guenther LC, Gooderham M, et al. A head-to-head comparison of ixekizumab vs. guselkumab in patients with moderate-to-severe plaque psoriasis: 24-week efficacy and safety results from a randomized, double-blinded trial. Br J Dermatol. 2021:184(6):1047–58.
Harnett J, Gerber R, Gruben D, Koenig AS, Chen C. Evaluation of real-world experience with tofacitinib compared with adalimumab, etanercept, and abatacept in RA patients with 1 previous biologic DMARD: data from a U.S. administrative claims database. J Manag Care Specialty Pharmacy. 2016;22(12):1457–71.
Murage MJ, Tongbram V, Feldman SR, Malatestinic WN, Larmore CJ, Muram TM, et al. Medication adherence and persistence in patients with rheumatoid arthritis, psoriasis, and psoriatic arthritis: a systematic literature review. Patient Prefer Adherence. 2018;12:1483–503.
Doshi JA, Takeshita J, Pinto L, Li P, Yu X, Rao P, et al. Biologic therapy adherence, discontinuation, switching, and restarting among patients with psoriasis in the US Medicare population. J Am Acad Dermatol. 2016;74(6):1057–65 e4.
Li P, Blum MA, Von Feldt J, Hennessy S, Doshi JA. Adherence, discontinuation, and switching of biologic therapies in medicaid enrollees with rheumatoid arthritis. Value Health. 2010;13(6):805–12.
Johnston SS, McMorrow D, Farr AM, Juneau P, Ogale S. Comparison of biologic disease-modifying antirheumatic drug therapy persistence between biologics among rheumatoid arthritis patients switching from another biologic. Rheumatol Ther. 2015;2(1):59–71.
Belinchon I, Rivera R, Blanch C, Comellas M, Lizan L. Adherence, satisfaction and preferences for treatment in patients with psoriasis in the European Union: a systematic review of the literature. Patient Prefer Adherence. 2016;10:2357–67.
Costanzo A, Malara G, Pelucchi C, Fatiga F, Barbera G, Franchi A, et al. Effectiveness end points in real-world studies on biological therapies in psoriasis: systematic review with focus on drug survival. Dermatology. 2018;234(1–2):1–12.
Sbidian E, Mezzarobba M, Weill A, Coste J, Rudant J. Persistence of treatment with biologics for patients with psoriasis: a real-world analysis of 16 545 biologic-naive patients from the French National Health Insurance database (SNIIRAM). Br J Dermatol. 2019;180(1):86–93.
Sruamsiri R, Iwasaki K, Tang W, Mahlich J. Persistence rates and medical costs of biological therapies for psoriasis treatment in Japan: a real-world data study using a claims database. BMC Dermatol. 2018;18(1):5.
Shalom G, Cohen AD, Feldhamer I, Comaneshter D, Freud T, Pavlovsky L. Drug survival in patients with psoriasis is associated with the availability of biologic medications. J Euro Acad Dermatol Venereol. 2020;34(7):1524–8.
Wu B, Muser E, Teeple A, Pericone CD, Feldman SR. Treatment adherence and persistence of five commonly prescribed medications for moderate to severe psoriasis in a U.S. commercially insured population. J Dermatolog Treat. 2021;32(6):595–602.
Acknowledgements
Funding
This study was funded by Eli Lilly and Company, including the Rapid Service Fee for publication.
Medical Writing Assistance
Medical writing assistance was provided during the preparation of this article by Thomas Melby of Syneos Health. Support for this assistance was funded by Eli Lilly and Company.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Fangyu Wang and Baojin Zhu. The first draft of the manuscript was written by Russel Burge and Baojin Zhu and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Disclosures
Andrew Blauvelt have received honoraria as a scientific adviser/clinical study investigator from AbbVie, Aligos, Almirall, Amgen, Arcutis, Arena, Athenex, Boehringer Ingelheim, Bristol-Myers Squibb, Dermavant, EcoR1, Eli Lilly and Company, Evommune, Forte, Galderma, Incyte, Janssen, Leo, Novartis, Pfizer, Rapt, Regeneron, Sanofi Genzyme, Sun Pharma, UCB Pharma and Vibliome, but none related to this work. Russel Burge, Gaia Gallo, Bridget Charbonneau, William Malatestinic, Baojin Zhu, and Fangyu Wang were employees and held stock in Eli Lilly and Company. Benjamin Lockshin has served as a speaker and/or investigator for AbbVie, Amgen, Celgene Corporation, Eli Lilly and Company, Janssen, Galderma, Incyte, Leo, Novartis, Pfizer, Regeneron, Sanofi Genzyme, Sun Pharma, and UCB Pharma, but none related to this work.
Compliance with Ethics Guidelines
Ethics committee approval was not required for this analysis of anonymized patient claims data.
Data Availability
The datasets generated during and/or analyzed during the current study are not publicly available as they are proprietary to IBM Watson Health.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Blauvelt, A., Burge, R., Gallo, G. et al. A Retrospective Cohort Analysis of Treatment Patterns Over 1 Year in Patients with Psoriasis Treated with Ixekizumab or Guselkumab. Dermatol Ther (Heidelb) 12, 701–714 (2022). https://doi.org/10.1007/s13555-022-00686-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-022-00686-1