
Abstract
Introduction
A newly developed resistant starch (RS) rice line with double mutation of starch synthase IIIa and branching enzyme IIb (ss3a/be2b) exhibits a tenfold greater percentage RS value than the wild-type rice line. Currently, the effects of cooked rice with such high RS content on secretion and action of glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) are unclear. Therefore, we conducted a pilot study to assess postprandial responses of GLP-1 and GIP along with glucose and insulin and also gastric emptying after ingestion of the high-RS cooked rice with ss3a/be2b in healthy subjects.
Methods
In a non-randomized crossover design, five healthy men ingested two test foods, control (low-RS) and high-RS cooked rice, with at least 1-week washout period between testing days. Plasma glucose, serum insulin, plasma total GLP-1, plasma total GIP, and also gastric emptying rate were measured after ingestion of each test food, and the incremental area under the curves (iAUC) was calculated for each biochemical parameter using the values from 0 to 180 min after ingestion.
Results
The high-RS cooked rice ingestion tended to reduce iAUC-glucose (p = 0.06) and significantly reduced iAUC-insulin (p < 0.01) and iAUC-GLP-1 (p < 0.05) but not iAUC-GIP (p = 0.21) relative to control cooked rice ingestion. In addition, the high-RS cooked rice ingestion did not affect gastric emptying.
Conclusions
The present results indicate that the suppressive effects of the high-RS cooked rice ingestion on postprandial responses of glucose and insulin may be provided through attenuation in GLP-1 secretion along with its low digestibility into glucose. We suggest that the high-RS rice with ss3a/be2b may serve as a better carbohydrate source and also as a novel functional food for dietary interventions to improve postprandial hyperglycemia and hyperinsulinemia without both enhancing GLP-1 secretion and affecting gastric emptying in patients with diabetes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
The effects of ingestion of novel high resistant starch (RS) rice with double mutation of starch synthase IIIa and branching enzyme IIb (ss3a/be2b) on secretion and action of glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) are unclear. |
In a non-randomized crossover design, five healthy men ingested two test foods, control (low-RS) and high-RS cooked rice, with at least 1-week washout period between testing days, and biochemical parameters including plasma glucose, serum insulin, plasma total GLP-1, and plasma total GIP and also gastric emptying rate were measured after ingestion of each test food. |
What was learned from this study? |
High-RS cooked rice ingestion tended to attenuate postprandial plasma glucose elevation and significantly suppressed postprandial elevations of serum insulin and plasma total GLP-1 but not plasma total GIP relative to ingestion of control cooked rice, and it did not affect gastric emptying. |
High-RS rice with ss3a/be2b may serve as a novel functional food for dietary interventions to ameliorate postprandial hyperglycemia and hyperinsulinemia without both enhancing GLP-1 release and affecting gastrointestinal motility in patients with diabetes. |
Introduction
Postprandial glucose homeostasis is regulated by various factors including meal nutrient composition, gastric emptying, glucose absorption, and secretion of insulin and incretins (glucagon-like peptide-1 [GLP-1] and glucose-dependent insulinotropic polypeptide [GIP]) [1, 2]. Accordingly, pharmacological and nutritional interventions based on these factors would be useful to lower postprandial hyperglycemia in daily clinical practice. Indeed, antidiabetic drugs such as α-glucosidase inhibitor, glinide, dipeptidyl peptidase-4 inhibitor, GLP-1 receptor agonist, and fast-acting insulin are widely used as a pharmacological approach for postprandial hyperglycemia control. Regarding dietary and nutritional approaches for postprandial glucose control, several interventions have been developed so far. For example, recent clinical studies have shown that preloading of vegetables and proteins before carbohydrate intake can reduce postprandial hyperglycemia in patients with type 2 diabetes [3,4,5].
Resistant starch (RS) is defined as the part of the starch molecule that is resistant to enzymatic digestion in the small intestine and eventually reaches the colon relatively unchanged, acting as a dietary fiber [6]. Based on such characteristics, RS has been recognized as a potential functional food for the prevention of chronic human diseases including diabetes, obesity, and colon cancer [7]. Especially, the intake of high-RS foods may provide beneficial metabolic effects in management of postprandial glucose elevation and furthermore in elimination of the risk for development of type 2 diabetes, because RS is resistant to digestion into glucose molecules. Indeed, several clinical studies have indicated that high-RS food intake reduces postprandial hyperglycemia and hyperinsulinemia in healthy subjects [8, 9] and subjects with impaired glucose tolerance [10].
Despite increasing data showing improvements in postprandial hyperglycemia and hyperinsulinemia after the ingestion of high-RS foods, the impact of RS on secretion and action of primary incretin hormones, GLP-1 and GIP, remains poorly understood. GLP-1 is secreted from L-cells in the distal small intestine (ileum) and colon, while GIP is released from K-cells in the proximal small intestine (duodenum and jejunum) [11, 12]. The release of GLP-1 and GIP can be stimulated by oral ingestion of nutrients including glucose and other sugars, fatty acids, essential amino acids, and dietary fiber, and these incretin hormones enhance glucose-stimulated insulin secretion [12]. Especially, nutrient ingestion of glucose and fat is known to be the primary physiologic stimulus for the secretion of GLP-1 and GIP [12].
We newly developed a high-RS rice line with double mutation of starch synthase IIIa and branching enzyme IIb (ss3a/be2b) [13], which was obtained by non-transgenic method, crossing between ss3a mutant [14] and be2b mutant [15]. The endosperm starch in the rice line contained more than 40% amylose and more amylopectin long chains, which can cause high-RS compared to normal rice cultivars [16]. Cooked rice is a commonly consumed staple food and serves as a primary carbohydrate source in Asian countries, and hence it may be an important target for carbohydrate-based dietary interventions. In the present study, we hypothesized that ingestion of high-RS cooked rice may attenuate postprandial responses of GLP-1 and GIP in addition to glucose and insulin because of its low digestibility into glucose leading to reduction in glucose stimulus in the small intestine. To test this hypothesis, we investigated the responses of glucose, insulin, GLP-1, and GIP after ingestion of the newly developed high-RS cooked rice with ss3a/be2b [13, 16] in healthy male subjects, and further examined gastric emptying rate, which may be influenced by the alteration of plasma GLP-1 levels.
Methods
Study Participants
Five healthy male participants were recruited from the Akita University Hospital, Akita, Japan. The exclusion criteria included diabetes; hyperlipidemia; obesity; malnutrition; liver, kidney, and heart diseases. The clinical characteristics of the study participants are shown in Table 1. All the enrolled participants were eligible to participate in this study. This study was approved by the Ethics Committees of Akita University (approval number 2220), and was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Nutrient Composition of Test Foods
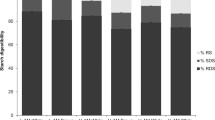
Two test foods, control and RS cooked rice, were prepared by steaming with 100 mg of 13C-acetic acid (CLM-156-0, Cambridge Isotope Laboratories, Tewksbury, MA, USA). Total cooked rice weight ingested was 150 g in both the two test foods. The nutrient composition of the two test foods is summarized in Table 2. Total RS content was measured by the method developed by McClearly et al. [17]. RS cooked rice contained 5.1 g of RS derived from rice with ss3a/be2b (3.4% of total cooked rice weight ingested), while control cooked rice contained 0.9 g of RS derived from conventional Akitakomachi rice (0.6% of total cooked rice weight ingested).
Study Protocol
The study protocol is shown in Fig. 1. In the present study, we could not enroll a large number of participants needed to employ a randomized cross-over design due to limited research budget and time. Therefore, we conducted a pilot study in a non-randomized crossover design in the small sample size. During the study period, the participants were instructed to eat a traditional Japanese-style diet. In a non-randomized crossover design, the participants ingested two test foods in the order of control and RS cooked rice with at least 1-week washout period between testing days, and biochemical parameters and gastric emptying rate were determined after ingestion of each test food. At 9:00 AM after overnight fasting, the participants ingested 150 g of control or RS cooked rice with 150 ml of water within 10 min. Blood samples were collected at fasting and additionally at 30, 60, 120, and 180 min at the completion of each test food ingestion. The levels of biochemical parameters in blood samples collected at fasting are defined as 0-min value.

Study protocol of the study
Measurements of Biochemical Parameters
The levels of plasma glucose, serum insulin, plasma total GLP-1, and plasma total GIP were determined for each time point. Besides, we calculated the incremental area under the curves of plasma glucose (iAUC-glucose), serum insulin (iAUC-insulin), plasma total GLP-1 (iAUC-GLP-1), and plasma total GIP (iAUC-GIP) using the values from 0 to 180 min based on the trapezoidal rule. Serum insulin was measured by chemiluminescent enzyme immunoassay (SRL, Tokyo, Japan). Plasma total GLP-1 and GIP were measured in duplicate using the enzyme immunoassay (EIA) kits (Phoenix Pharmaceuticals, Burlingame, CA, USA), and intra- and inter-assay coefficients of variation in the EIA were < 10 and < 15%, respectively. HbA1c, total cholesterol, and triglyceride were measured by enzymatic assay (SRL, Tokyo, Japan), and HDL cholesterol was measured directly (SRL, Tokyo, Japan).
Evaluation of Gastric Emptying Rate
A standardized 13C acetic acid breath test was performed to determine gastric emptying rate. The breath test methodology has been described previously [4, 18]. Briefly, breath samples were continuously collected from the nasal tube, and the 13CO2/12CO2 ratio was measured using BreathID system (Exalenz Bioscience, Modiin, Israel) up to 180 min after ingestion of each test food. The 13CO2/12CO2 ratio in breath samples collected at fasting is defined as 0-min value. Gastric emptying rate was determined based on the 13CO2/12CO2 ratio in the breath samples, and the time50%, which indicates the time needed for 50% of 13C acetic acid to be excreted from the stomach, was also calculated. Gastric emptying coefficient indicating the inclination of the 13CO2 excretion in the early phase was calculated as previously described [18].
Statistical Analysis
Data are presented as means ± SD. Repeated-measures data were analyzed by mixed effects models. Differences between two test foods for iAUC values, time50%, and gastric emptying coefficient were determined by paired t test or Wilcoxon signed-rank test where appropriate. p < 0.05 was considered statistically significant. Statistical analysis was performed using GraphPad Prism software (GraphPad, San Diego, CA, USA).
Results
Plasma Glucose and Serum Insulin Levels After Ingestion of Control and RS Cooked Rice
The changes in plasma glucose and serum insulin after ingestion of the two test foods are shown in Fig. 2. The p values for differences due to test food, time, and their interaction calculated using mixed effects models were 0.1701, < 0.0001, and 0.5715, respectively, for plasma glucose, and 0.0091, < 0.0001, and 0.3872, respectively, for serum insulin. iAUC-glucose values for control and RS cooked rice were 125 ± 72 and 63 ± 32 mmol/l × min, respectively (Fig. 2C). The iAUC-glucose tended to be reduced after ingestion of RS cooked rice relative to control cooked rice (p = 0.06, Fig. 2C). iAUC-insulin values for control and RS cooked rice were 19.8 ± 6.3 and 8.3 ± 3.6 nmol/l × min, respectively (Fig. 2D). The iAUC-insulin was significantly reduced after ingestion of RS cooked rice relative to control cooked rice (p < 0.01, Fig. 2D).

Changes in plasma glucose and serum insulin levels. A Plasma glucose and B serum insulin levels after ingestion of control and RS cocked rice. C iAUC-glucose and D iAUC-insulin calculated using the values from 0 to 180 min after ingestion of control and RS cocked rice
Plasma GLP-1 and GIP Levels After Ingestion of Control and RS Cooked Rice
The time course data on plasma GLP-1 and GIP after ingestion of the two test foods are shown in Fig. 3. The p values for differences due to test food, time, and their interaction calculated using mixed effects models were 0.0098, 0.6510, and 0.8499, respectively, for plasma GLP-1, and 0.0194, < 0.0001, and 0.7832, respectively, for plasma GIP. iAUC-GLP-1 values for control and RS cooked rice were 1716 ± 829 and 636 ± 695 pmol/l × min, respectively (Fig. 3C). The iAUC-GLP-1 was significantly lower after ingestion of RS cooked rice than control cooked rice (p < 0.05, Fig. 3C). iAUC-GIP values for control and RS cooked rice were 23.7 ± 3.3 and 19.0 ± 4.4 nmol/l × min, respectively (Fig. 3D). The iAUC-GIP was not significantly different between after ingestion of control and RS cooked rice (p = 0.21, Fig. 3D).

Changes in plasma total GLP-1 and GIP levels. A Plasma total GLP-1 and B plasma total GIP levels after ingestion of control and RS cocked rice. C iAUC-GLP-1 and D iAUC-GIP calculated using the values from 0 to 180 min after ingestion of control and RS cocked rice
Evaluation of Gastric Emptying After Ingestion of Control and RS Cooked Rice
Through the analyses by 13C acetic acid breath test, we observed similar time course curves of gastric emptying rate after meals between the control and RS cooked rice ingestion (Fig. 4A). Time50% values after ingestion of control and RS cooked rice were 13.7 ± 5.9 and 15.2 ± 4.9 min, respectively (Fig. 4B). Besides, gastric emptying coefficient values after ingestion of control and RS cooked rice were 3.6 ± 0.3 and 3.6 ± 0.3, respectively (Fig. 4C). Both time50% and gastric emptying coefficient were not significantly different between after ingestion of control and RS cooked rice (p = 0.16 for time50%, Fig. 4B; p = 0.44 for gastric emptying coefficient, Fig. 4C).

Changes in gastric emptying. A Gastric emptying rate, B time50%, and C gastric emptying coefficient after ingestion of control and RS cocked rice
Discussion
In the current study, we first found that plasma glucose elevation after intake of high-RS cooked rice tended to be suppressed as compared with that after the control cooked rice ingestion (Fig. 2). The suppressive effects of the current high-RS cooked rice on postprandial plasma glucose elevation would not be attributed to an enhancement of insulin secretion following their ingestion, because intake of the high-RS cooked rice significantly suppressed the elevation of postprandial serum insulin levels (Fig. 2). Consistent with our findings, a recent clinical study has reported a significant attenuation in insulin responses after high-RS food ingestion in healthy subjects [8]. Considering the digestibility properties of the high-RS cooked rice, it is likely that this food reduces breakdown and absorption of glucose in the small intestine and consequently attenuates postprandial plasma glucose elevation, accompanied with suppression of rapid glucose-stimulated insulin secretion from pancreatic β-cells after the food ingestion. Taken together, the present results suggest that the newly developed RS cooked rice used in this study would contribute to amelioration of postprandial hyperglycemia and hyperinsulinemia, which are recognized as a risk factor for cardiovascular disease [19, 20].
Grains such as rice, wheat, and maize in addition to vegetables, fruits, milk, and milk products are the major food sources of carbohydrates [21]. Rice, wheat, and maize are the most common staple foods worldwide, and these grains are rich in starch. Starch chemically consists of amylose and amylopectin, which are two polymers composed of glucose units. Amylose has a straight linear chain of glucose molecules, while amylopectin is a branched polymer of glucose molecules [22]. It is well established that starches with high-amylose and/or longer amylopectin chains exhibit higher resistance to enzymatic digestion due to their structure, and therefore work as a type of RS [16, 22, 23]. The RS rice line with ss3a/be2b has higher amylose content and longer amylopectin chains [13, 16]. As reported, the percentage RS value in ss3a/be2b double-mutant rice line is tenfold greater than the wild-type rice line [16]. The RS cooked rice ingested in this study had a high amount of RS (3.4% of total cooked rice weight ingested, Table 2). In contrast, the conventional Akitakomachi rice used as control cooked rice in this study included a low amount of RS (0.6% of total cooked rice weight ingested, Table 2). The present study indicated reduced glycemic and insulinemic responses with high-RS rice compared to lower-RS rice, in agreement with recent and previous research [8, 9].
While a large body of evidence suggests that high-RS food ingestion produces a significant attenuation in glucose and insulin responses, the findings from clinical studies investigating the effects of high-RS food ingestion on a primary incretin hormone, GLP-1, seem to be contradictory. Bodinham et al. reported that plasma GLP-1 concentrations were lower after ingestion of high-amylose maize RS type 2 (HAM-RS2) than a matched placebo in healthy males [24]. Similarly, Maziarz et al. indicated that consuming muffins with HAM-RS2 daily for 6 weeks did not significantly increase plasma total GLP-1 concentrations after meal as compared with intake of control muffins in overweight healthy adults [25]. Conversely, Zhang et al. reported that serum GLP-1 levels after meal were increased by RS intervention with 4-week HAM-RS2 intake relative to control starch consumption in subjects with normal weights [26]. Furthermore, a clinical study in patients with well-controlled type 2 diabetes showed that fasting plasma total GLP-1 levels after HAM-RS2 ingestion for 12 weeks were significantly lower than those after placebo ingestion, whereas postprandial GLP-1 excursions during a meal tolerance test were significantly greater after HAM-RS2 ingestion [27]. In several animal studies, an enhancement of GLP-1 secretion by RS diet has been shown [28,29,30,31]. Thus, there are inconsistent findings regarding the effect of RS ingestion on GLP-1 secretion, especially in clinical studies. Consistent with the observation reported by Bodinham et al. [24], our data show that ingestion of the newly developed high-RS cooked rice with ss3a/be2b suppresses postprandial plasma GLP-1 elevation, which may partially contribute to an attenuation in postprandial insulin responses (Fig. 3). On the other hand, the impact of high-RS food ingestion on the release of another primary incretin hormone, GIP, remains unclear. Although repeated measures data on plasma GIP analyzed using mixed effects models indicated a significant difference due to test food, iAUC-GIP was not significantly different between after ingestion of control and RS cooked rice. Focusing on iAUC-GIP, we speculate that postprandial plasma GIP levels might not be affected by the high-RS cooked rice intake (Fig. 3), and this might be explained by the concept that reduction in luminal glucose concentrations after the high-RS cooked rice ingestion is relatively mild in the proximal small intestine where GIP-secreting K-cells are located. Collectively, the present results indicate that the high-RS cooked rice ingestion attenuates rapid release of GLP-1 but not GIP after meal. These findings might be explained by the following points. First, luminal glucose concentrations in the small intestine are reduced after ingestion of such high-RS cooked rice as compared with low-RS cooked rice, since the high-RS cooked rice is slowly digested to glucose molecules. Second, GLP-1-releasing L-cells are localized in more distal part of the small intestine than GIP-secreting K-cells, perhaps leading to less glucose exposure and absorption there under the lower luminal glucose concentrations. The high-RS cooked rice is gradually digested in the proximal small intestine and may be more resistance to digestion at distal part of the small intestine. Through the resistance to digestion of the high-RS cooked rice into glucose and the subsequent reduction of glucose-stimulus for the L-cells, the ingestion of such high-RS cooked rice may attenuate GLP-1 release after meal.
It has been well appreciated that GLP-1 acts to slow gastric emptying and thereby to delay absorption of nutrients in the small intestine [11, 12, 32]. Importantly, gastric emptying tied to nutrient delivery is a key determinant of extrapancreatic GLP-1 action on postprandial glucose control [11]. Recent clinical studies have clearly documented that pharmacological GLP-1 concentration by administration of GLP-1 receptor agonists leads to a significantly delayed gastric emptying [18, 33]. In the present study, we observed a significant suppression of plasma GLP-1 elevation after the high-RS cooked rice ingestion. However, such change within the physiological GLP-1 range did not affect gastric emptying in healthy subjects (Fig. 4). It appears to be still controversial whether endogenous GLP-1, similar to exogenous GLP-1 and GLP-1 receptor agonists, exerts an effect on gastric emptying. In several clinical studies, the role of endogenous GLP-1 in gastric emptying was evaluated through blocking its action by administration of a GLP-1 receptor antagonist, exendin (9–39) amide in healthy subjects. While two studies showed that gastric emptying was not changed by GLP-1 receptor antagonism [34, 35], one of these studies indicated that GLP-1 receptor antagonism accelerated gastric emptying [36]. Although this issue still remains to be addressed, the present results, which can be assessed excluding the confounding factors accompanied with the use of drug such as GLP-1 receptor antagonist, clearly demonstrate that the alteration of plasma GLP-1 levels within the physiological range after the high-RS cooked rice ingestion does not affect the gastric emptying. On the other hand, a previous clinical study reported that the addition of fat to a carbohydrate load slowed gastric emptying and reduced postprandial glycemia in healthy men [37]. Therefore, further studies should be conducted to clarify the potential for co-ingestion of other nutrients to alter gastric emptying in future.
High-RS cooked rice ingestion may affect the gut microbiome composition which is known to be associated with the development of metabolic syndrome and glucose metabolism. A recent clinical study showed that HAM-RS2 ingestion for 4 weeks reduced the intra-abdominal and subcutaneous fat areas, and decreased the levels of several gut bacteria genera in normal-weight subjects [26]. However, a recent review indicates that changes in fecal bacterial composition by RS ingestion are inconsistent not only between human studies but also between animal studies [38]. To clarify such changes to gut bacterial diversity by RS ingestion, further studies would be needed.
There are several limitations to this study. First, this work was a pilot trial in a non-randomized crossover design performed in the small number of participants, and was not a placebo-controlled study. Second, only males were included as a participant in this study. Due to limited resources, and considering well-known differences in gastric emptying between men and women [39, 40], we enrolled only healthy men for this pilot study. We calculated total sample size for analysis of GIP, which seems to be smallest effect of the outcomes, with α = 0.05 and 1 − β = 0.8 using G*Power software (Heinrich Heine University), and the required sample size in future studies based on our current pilot data was estimated to be approximately 30 subjects. Therefore, further studies in the large number of participants including both males and females or clinical populations with impaired glucose tolerance are required to support the present findings.

Proposed mechanism of attenuation in postprandial responses of glucose, insulin, and GLP-1 after high-RS cooked rice ingestion. High-RS cooked rice is more resistant to digestion into glucose molecule as compared with low-RS cooked rice, and therefore the amount of glucose reaching small intestine is diminished after high-RS cooked rice ingestion. Lowered luminal glucose concentration in the small intestine could lead to reduction in intestinal glucose absorption and subsequent attenuation in glucose-stimulated insulin secretion. Furthermore, since GLP-1-secreting L-cells are located in more distal part of small intestine than GIP-secreting K-cells, the amount of glucose reaching there would be markedly decreased after high-RS cooked rice ingestion, consequently leading to attenuation in nutrient (glucose)-stimulated GLP-1 release and further suppression of insulin secretion through GLP-1 receptor signaling
Conclusions
The current pilot study offers the first evidence that ingestion of high-RS cooked rice with ss3a/be2b attenuates postprandial responses of glucose, insulin and GLP-1 but not GIP without affecting gastric emptying. The suppressive effects of the high-RS cooked rice on postprandial glucose and insulin elevation may be provided through attenuation in GLP-1 secretion along with its low digestibility into glucose, different from postprandial glucose-lowering and insulin-elevating mechanism by GLP-1 receptor agonists. Possible mechanism underlying the effects of high-RS cooked rice ingestion on postprandial responses of glucose, insulin, and incretin hormones is summarized in Fig. 5. Finally, we suggest that the newly developed high-RS rice with ss3a/be2b may serve as a better carbohydrate source and also as a functional food for dietary interventions to improve postprandial hyperglycemia and hyperinsulinemia without both enhancing GLP-1 secretion and affecting gastric emptying in patients with diabetes.
References
Brubaker PL, Ohayon EL, D’Alessandro LM, Norwich KH. A mathematical model of the oral glucose tolerance test illustrating the effects of the incretins. Ann Biomed Eng. 2007;35:1286–300.
Holst JJ, Gribble F, Horowitz M, Rayner CK. Roles of the gut in glucose homeostasis. Diabetes Care. 2016;39:884–92.
Imai S, Fukui M, Kajiyama S. Effect of eating vegetables before carbohydrates on glucose excursions in patients with type 2 diabetes. J Clin Biochem Nutr. 2014;54:7–11.
Kuwata H, Iwasaki M, Shimizu S, Minami K, Maeda H, Seino S, et al. Meal sequence and glucose excursion, gastric emptying and incretin secretion in type 2 diabetes: a randomised, controlled crossover, exploratory trial. Diabetologia. 2016;59:453–61.
Bae JH, Kim LK, Min SH, Ahn CH, Cho YM. Postprandial glucose-lowering effect of premeal consumption of protein-enriched, dietary fiber-fortified bar in individuals with type 2 diabetes mellitus or normal glucose tolerance. J Diabetes Investig. 2018;9:1110–8.
Englyst HN, Kingman SM, Cummings JH. Classification and measurement of nutritionally important starch fractions. Eur J Clin Nutr. 1992;46(Suppl 2):S33-50.
Birt DF, Boylston T, Hendrich S, Jane JL, Hollis J, Li L, et al. Resistant starch: promise for improving human health. Adv Nutr. 2013;4:587–601.
Saito Y, Watanabe T, Sasaki T, Watanabe K, Hirayama M, Fujita N. Effects of single ingestion of rice cracker and cooked rice with high resistant starch on postprandial glucose and insulin responses in healthy adults: two randomized, single-blind, cross-over trials. Biosci Biotechnol Biochem. 2020;84:365–71.
Granfeldt Y, Drews A, Björck I. Arepas made from high amylose corn flour produce favorably low glucose and insulin responses in healthy humans. J Nutr. 1995;125:459–65.
Yamada Y, Hosoya S, Nishimura S, Tanaka T, Kajimoto Y, Nishimura A, et al. Effect of bread containing resistant starch on postprandial blood glucose levels in humans. Biosci Biotechnol Biochem. 2005;69:559–66.
Drucker DJ. The biology of incretin hormones. Cell Metab. 2006;3:153–65.
Baggio LL, Drucker DJ. Biology of incretins: GLP-1 and GIP. Gastroenterology. 2007;132:2131–57.
Asai H, Abe N, Matsushima R, Crofts N, Oitome NF, Nakamura Y, et al. Deficiencies in both starch synthase IIIa and branching enzyme IIb lead to a significant increase in amylose in SSIIa-inactive japonica rice seeds. J Exp Bot. 2014;65:5497–507.
Fujita N, Yoshida M, Kondo T, Saito K, Utsumi Y, Tokunaga T, et al. Characterization of SSIIIa-deficient mutants of rice: the function of SSIIIa and pleiotropic effects by SSIIIa deficiency in the rice endosperm. Plant Physiol. 2007;144:2009–23.
Nishi A, Nakamura Y, Tanaka N, Satoh H. Biochemical and genetic analysis of the effects of amylose-extender mutation in rice endosperm. Plant Physiol. 2001;127:459–72.
Tsuiki K, Fujisawa H, Itoh A, Sato M, Fujita N. Alterations of starch structure lead to increased resistant starch of steamed rice: Identification of high resistant starch rice lines. J Cereal Sci. 2016;68:88–92.
McCleary BV, Monaghan DA. Measurement of resistant starch. J AOAC Int. 2002;85:665–75.
Suganuma Y, Shimizu T, Sato T, Morii T, Fujita H, Harada Sassa M, et al. Magnitude of slowing gastric emptying by glucagon-like peptide-1 receptor agonists determines the amelioration of postprandial glucose excursion in Japanese patients with type 2 diabetes. J Diabetes Investig. 2020;11:389–99.
Bonora E, Muggeo M. Postprandial blood glucose as a risk factor for cardiovascular disease in type II diabetes: the epidemiological evidence. Diabetologia. 2001;44:2107–14.
Ruige JB, Assendelft WJ, Dekker JM, Kostense PJ, Heine RJ, Bouter LM. Insulin and risk of cardiovascular disease: a meta-analysis. Circulation. 1998;97:996–1001.
Slavin J, Carlson J. Carbohydrates. Adv Nutr. 2014;5:760–1.
Seung D. Amylose in starch: towards an understanding of biosynthesis, structure and function. New Phytol. 2020;228:1490–504.
Magallanes-Cruz PA, Flores-Silva PC, Bello-Perez LA. Starch structure influences its digestibility: a review. J Food Sci. 2017;82:2016–23.
Bodinham CL, Al-Mana NM, Smith L, Robertson MD. Endogenous plasma glucagon-like peptide-1 following acute dietary fibre consumption. Br J Nutr. 2013;110:1429–33.
Maziarz MP, Preisendanz S, Juma S, Imrhan V, Prasad C, Vijayagopal P. Resistant starch lowers postprandial glucose and leptin in overweight adults consuming a moderate-to-high-fat diet: a randomized-controlled trial. Nutr J. 2017;16:14.
Zhang L, Ouyang Y, Li H, Shen L, Ni Y, Fang Q, et al. Metabolic phenotypes and the gut microbiota in response to dietary resistant starch type 2 in normal-weight subjects: a randomized crossover trial. Sci Rep. 2019;9:4736.
Bodinham CL, Smith L, Thomas EL, Bell JD, Swann JR, Costabile A, et al. Efficacy of increased resistant starch consumption in human type 2 diabetes. Endocr Connect. 2014;3:75–84.
Zhou J, Martin RJ, Tulley RT, Raggio AM, McCutcheon KL, Shen L, et al. Dietary resistant starch upregulates total GLP-1 and PYY in a sustained day-long manner through fermentation in rodents. Am J Physiol Endocrinol Metab. 2008;295:E1160–6.
Vidrine K, Ye J, Martin RJ, McCutcheon KL, Raggio AM, Pelkman C, et al. Resistant starch from high amylose maize (HAM-RS2) and dietary butyrate reduce abdominal fat by a different apparent mechanism. Obesity (Silver Spring). 2014;22:344–8.
Hira T, Ikee A, Kishimoto Y, Kanahori S, Hara H. Resistant maltodextrin promotes fasting glucagon-like peptide-1 secretion and production together with glucose tolerance in rats. Br J Nutr. 2015;114:34–42.
Shen L, Keenan MJ, Martin RJ, Tulley RT, Raggio AM, McCutcheon KL, et al. Dietary resistant starch increases hypothalamic POMC expression in rats. Obesity (Silver Spring). 2009;17:40–5.
Marathe CS, Rayner CK, Jones KL, Horowitz M. Effects of GLP-1 and incretin-based therapies on gastrointestinal motor function. Exp Diabetes Res. 2011;2011: 279530.
Quast DR, Schenker N, Menge BA, Nauck MA, Kapitza C, Meier JJ. Effects of lixisenatide versus liraglutide (short- and long-acting GLP-1 receptor agonists) on esophageal and gastric function in patients with type 2 diabetes. Diabetes Care. 2020;43:2137–45.
Nicolaus M, Brodl J, Linke R, Woerle HJ, Goke B, Schirra J. Endogenous GLP-1 regulates postprandial glycemia in humans: relative contributions of insulin, glucagon, and gastric emptying. J Clin Endocrinol Metab. 2011;96:229–36.
Witte AB, Gryback P, Jacobsson H, Naslund E, Hellstrom PM, Holst JJ, et al. Involvement of endogenous glucagon-like peptide-1 in regulation of gastric motility and pancreatic endocrine secretion. Scand J Gastroenterol. 2011;46:428–35.
Deane AM, Nguyen NQ, Stevens JE, Fraser RJ, Holloway RH, Besanko LK, et al. Endogenous glucagon-like peptide-1 slows gastric emptying in healthy subjects, attenuating postprandial glycemia. J Clin Endocrinol Metab. 2010;95:215–21.
Cunningham KM, Read NW. The effect of incorporating fat into different components of a meal on gastric emptying and postprandial blood glucose and insulin responses. Br J Nutr. 1989;61:285–90.
Bendiks ZA, Knudsen KEB, Keenan MJ, Marco ML. Conserved and variable responses of the gut microbiome to resistant starch type 2. Nutr Res. 2020;77:12–28.
Cordova-Fraga T, De la Roca-Chiapas JM, Solis S, Sosa M, Bernal-Alvarado J, Hernandez E, et al. Gender difference in the gastric emptying measured by magnetogastrography using a semi-solid test meal. Acta Gastroenterol Latinoam. 2008;38:240–5.
Datz FL, Christian PE, Moore J. Gender-related differences in gastric emptying. J Nucl Med. 1987;28:1204–7.
Acknowledgements
The authors would like to thank all study participants and all medical staff members. The authors would also like to thank Ms. Hiromi Fujishima for her excellent technical support.
Funding
This work was supported by the Science and Technology Research Promotion Program for Agriculture, Forestry and Fisheries and Food Industry (N. Fujita, 25033AB and 28029C). The Rapid Service Fee was funded by the authors.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Conceptualization: Kazuyuki Takahashi, Hiroki Fujita, and Yuichiro Yamada; Methodology: Kazuyuki Takahashi, Hiroki Fujita, Naoko Fujita, and Yuichiro Yamada; Formal analysis and investigation: Kazuyuki Takahashi, Hiroki Fujita, Yuya Takahashi, Shunsuke Kato, Tatsunori Shimizu, Yumi Suganuma, and Takehiro Sato; Writing—original draft preparation: Kazuyuki Takahashi; Writing—review and editing: Hiroki Fujita, Naoko Fujita, Hironori Waki, and Yuichiro Yamada; Funding acquisition: Naoko Fujita; Resources: Naoko Fujita; Supervision: Hiroki Fujita, Naoko Fujita, Hironori Waki, and Yuichiro Yamada.
Disclosures
Kazuyuki Takahashi, Hiroki Fujita, Naoko Fujita, Yuya Takahashi, Shunsuke Kato, Tatsunori Shimizu, Yumi Suganuma, Takehiro Sato, Hironori Waki, and Yuichiro Yamada declare that they have no conflict of interest.
Compliance with Ethics Guidelines
This study was approved by the Ethics Committees of Akita University (approval number 2220), and was performed in accordance with the Helsinki Declaration of 1964 and its later amendments. Written informed consent was obtained from all participants.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Takahashi, K., Fujita, H., Fujita, N. et al. A Pilot Study to Assess Glucose, Insulin, and Incretin Responses Following Novel High Resistant Starch Rice Ingestion in Healthy Men. Diabetes Ther 13, 1383–1393 (2022). https://doi.org/10.1007/s13300-022-01283-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-022-01283-3