
Abstract
Introduction
This Delphi study aims to provide evidence-based expert opinion on the usage and current position of gliclazide in type 2 diabetes mellitus (T2DM) management in India.
Methods
The single interaction modified Delphi-based methodology was used to collect opinions on gliclazide usage and its position in diabetes management from 338 endocrinologists/diabetologists who have had clinical experience with gliclazide. Participants, using a 9-point scale, were asked to rate eight statements comprising a total of 52 items on the related topics.
Results
The Delphi consensus suggests that in drug-naïve patients with T2DM, intolerant to metformin or in whom metformin is contraindicated, dual therapy of gliclazide/gliclazide-modified release (MR) should be considered along with a dipeptidyl peptidase 4 (DPP4) inhibitor if glycated hemoglobin A1c level is greater than 7.5% and with insulin if the A1c level is greater than 9%. If the patients are inadequately controlled with metformin (A1c greater than 6.5% after 3 months of therapy), gliclazide/gliclazide-MR shall be added on to the treatment regimen to achieve greater and sustained reductions in A1c levels. However, it was not preferred over other antidiabetic classes in such clinical settings except alpha-glucosidase inhibitors (AGI). Early addition of gliclazide/gliclazide-MR shall be preferred over the up-titration of metformin beyond half-maximal dose for effective management of T2DM. Gliclazide/gliclazide-MR can be used safely in patients with diabetes and cardiovascular and chronic kidney disease. It can be used in older patients with T2DM as it does not have active metabolites and has a low risk of hypoglycemia.
Conclusion
The expert panel proposed consideration of monotherapy or dual therapy of gliclazide as an ideal choice in patients with T2DM because of its efficacy, long-term glycemic control, favorable renal outcomes, cardiovascular safety, and an optimal safety profile.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Limited information is available about current use of gliclazide in Indian routine clinical practice. | |
The study aims to provide expert opinion on the usage and current position of gliclazide in India. | |
This is a single interaction modified Delphi-based study including 338 endocrinologists/diabetologists. | |
The expert panel preferred gliclazide as monotherapy or dual therapy in patients with diabetes. | |
The expert consensus-based opinion justified the role of gliclazide in different clinical situations associated with diabetes. |
Digital Features
This article is published with digital features, including a summary slide, to facilitate understanding of the article. To view digital features for this article go to https://doi.org/10.6084/m9.figshare.13507329
Introduction
Nearly 80% of the world’s diabetes population lives in low- to middle-income countries [1]. In 2019, 77 million Indians aged 20–79 years had diabetes, and this number is projected to rise to 134.2 million by 2045 [2]. More than ever, safe and cost-effective therapies to treat diabetes are needed. Although new antidiabetic drugs offer certain benefits over their predecessors, they are available at higher costs and are not without safety concerns. Sulfonylureas (SUs) are widely used in India because of their glucose-lowering efficacy and affordability, with glimepiride and gliclazide being the most commonly prescribed SUs. A retrospective cross-sectional study from India found an increase in the use of SUs from 23.12% in patients with diabetes for 0–5 years to 70.77% in patients with diabetes for 10–15 years [3].
Multiple guidelines, such as the American Diabetes Association (ADA) 2020 guidelines, the International Diabetes Federation (IDF) clinical practice recommendations for managing type 2 diabetes mellitus (T2DM) in primary care 2017, Indian Council of Medical Research (ICMR) 2005 and Research Society for the Study of Diabetes in India (RSSDI), and Endocrine Society of India (ESI) clinical practice recommendations for the management of T2DM 2020, recommend oral antihyperglycemic drugs such as SUs to be used as monotherapy (if metformin is not tolerated) or as combination therapy [4,5,6,7].
Interestingly, few guidelines on diabetes management specifically suggest gliclazide as the second-line treatment, instead of SUs as a class [8]. The low risk of hypoglycemia, weight neutrality, cardiovascular (CV) safety, and favorable renal outcomes especially in patients with chronic kidney disease (CKD) appear to be the reasons for preference of gliclazide over other SUs [9]. Also, gliclazide protects β-cells by acting specifically on the pancreatic sulfonylurea receptor 1 (SUR1) and thereby delays the development of secondary treatment failure [9]. Further, gliclazide has been included along with metformin and insulin in the World Health Organization (WHO) model list of essential medicines 2019 under medicine for diabetes [10].
Although results from large studies have shown high diabetes burden, and high SUs prescription rate in India, limited information is available about their current use in diabetes management in routine clinical practice in India. Therefore, a collaborative Delphi methodology was considered appropriate to explore a set of questions drafted by a panel of experts in the field of diabetes and endocrinology. The current consensus is intended to provide opinion on the usage and current position of gliclazide across the diabetes continuum in India.
Methods
Survey Participants
Design
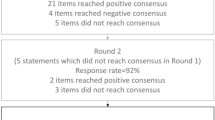
The Delphi method uses a structured group communication technique to explore novel concepts, answer research questions, and solve differences of opinions by looking at the pros and cons of specific arguments from all angles [11]. The present rank-based expert opinion is compiled adopting a single interaction collaborative Delphi process. This modification uses a combination of surveys and meetings involving a large group of endocrinologists and diabetologists (Fig. 1). The adopted methodology allows for arriving at a group consensus with reliability and help in clinical decision-making.

The Delphi process
The questionnaire was drafted by the steering committee (50 experts in the field of diabetes and endocrinology) after a thorough review of the literature on gliclazide and included seven statements comprising 46 items. Selection criteria for steering committee members are shown in Fig. 1 and were based on experience and research orientation so that collectively consensus can be formed on most pertinent research questions. After the expert review of the first draft, the final draft of eight statements comprising a total of 52 items was developed by the panel members to identify areas of agreement, relevance, and disagreement. Specifically, the questionnaire addressed the following issues:
-
1.
Decision to use gliclazide/gliclazide-modified release (MR) as valid option for drug-naïve patients with T2DM
-
2.
Decision to use gliclazide/gliclazide-MR as second-line treatment option for T2DM
-
3.
Decision to switch to gliclazide/gliclazide-MR-based combination therapy from other combination therapies in uncontrolled diabetes
-
4.
Efficacy of gliclazide/ gliclazide-MR in patients with diabetes and cardiovascular disease (CVD)
-
5.
Efficacy of gliclazide/ gliclazide-MR in patients with diabetes and CKD
-
6.
Dosing of the gliclazide-MR
-
7.
Safety and tolerability of gliclazide/gliclazide-MR
-
8.
Gliclazide/gliclazide MR in special populations
These eight statements comprising a total of 52 items were then sent to 338 participants through multiple meetings and emails in different parts of the country. All the participants were clinicians with strong experience in the use of gliclazide/gliclazide-MR as shown in Table 1. The participants were asked to rate each item using a 9-point scale, where the scores of 1, 2, 3, or 4 indicated degrees of disagreement and the scores of 6, 7, 8, or 9 indicated increasing degrees of agreement. A score of 5 was considered a neutral opinion. All the participants had the liberty to modify the statements and respond to them.
The rank was determined by calculating the percentage of participants agreeing or disagreeing (ranking) to each item in the eight statements. Items getting more than 30% responses were included in the final analysis. The items that were agreed upon by more than 50% of respondents were considered to be expert panel opinions.
Compliance with Ethics Guidelines
This study is based on a clinical practice questionnaire that does not involve the participation of human subjects or patient data management and does not aim to modify the current clinical practice of participants. As such, this study was deemed exempt from requiring ethical approval. Consent for publication of survey results was granted from all the experts participating in the program and undertaking the survey.
Result
Expert Panel Member Participation
A total of 338 doctors participated in this modified Delphi survey from 19 different cities of India. 39 respondents were from a northern city (Delhi, Jaipur), 88 from western cities (Mumbai, Pune, Nagpur, Indore, and Jabalpur), 54 from eastern cities (Kolkata, Ranchi, and Guwahati), and 157 from southern cities (Bangalore, Hyderabad, Thrissur, Kannur, Vijayawada, Trivandrum, Chennai, and Madurai) of India.
At the end of the Delphi study, the panel agreed on 48 items and disagreed on three items. Approved sentences underlying each statement are summarized in Table 2.
Decision to Use Gliclazide/Gliclazide-MR as Valid Option for Drug-Naïve Patients with T2DM
Current guidelines recommend metformin as the first-line, initial monotherapy, and as part of combination therapy for patients with T2DM [7, 12]. In case metformin is not suitable, the IDF recommends use of SU, dipeptidyl peptidase 4 (DPP4) inhibitor, or alpha-glucosidase inhibitors (AGI) for the treatment and prevention of T2DM [13, 14]. Several clinical trials comparing gliclazide with other antidiabetic agents such as metformin, pioglitazone, vildagliptin, or insulin have reported similar glycemic efficacy [15, 16]. In the EASYDia trial, nearly half of the treatment-naïve patients with diabetes successfully achieved an A1c of 7.0% or less at month 3 with gliclazide-MR therapy [17]. However, initiating therapy with multiple antidiabetes agents in patients with newly diagnosed T2DM, especially those with A1c greater than 8.0% to 8.5%, represents a rational approach to achieve the target A1c level while minimizing side effects. Indeed, the American Association of Clinical Endocrinology (AACE) recommends starting newly diagnosed diabetic subjects with A1c greater than 7.5% on multiple antidiabetes agents [18].
Opinions from experts on gliclazide use as first-line agent in drug-naïve patients with T2DM intolerant or contraindicated to metformin |
Gliclazide/gliclazide-MR and insulin dual therapy can be used in patients with A1c levels of > 9.0% (63.0%) |
Gliclazide/gliclazide-MR and DPP4 inhibitors dual therapy can be used in patients with A1c levels of 7.5–8.0% (51.2%) |
Decision to Use Gliclazide/Gliclazide-MR as Second-Line Treatment Option for T2DM
Several meta-analyses and randomized controlled trials have demonstrated the addition of SUs to metformin providing optimal glycemic control with acceptable safety [19, 20]. With the use of gliclazide-MR as a second-line antidiabetic agent, Schernthaner et al. demonstrated a significant reduction of 1.0% in A1c from 8.4% to 7.4% in patients with T2DM uncontrolled by metformin [21]. Australian and WHO guidelines (global resource-limited setting) recommend gliclazide as one of the preferred options for second-line therapy if hypoglycemia is a concern, while guidelines from the Canada and India specify gliclazide as the agent of choice for second-line therapy [6, 22,23,24]. In contrast, the 2018 consensus report from ADA and the European Association for the Study of Diabetes (EASD) recommends SU as second-line agents if the cost is a compelling issue. Indian consensus by Kalra et al. has also recommended SUs over glucagon-like peptide 1 (GLP-1) receptor agonists owing to similar glycemic efficacy and acceptable safety at a lower cost [19]. However, several studies have reported weight gain in patients on metformin and SUs and weight loss in patients on metformin and GLP-1 receptor agonists [25,26,27,28]. In 2016, a systematic review and network meta-analysis found a non-significant reduction in the incidence of hypoglycemia among patients with T2DM on GLP-1 receptor agonists compared to SUs [29]. It also recommends the addition of SU to metformin rather than metformin up-titration beyond half-maximal dose for better glycemic control [19]. HARMONY-3, a 104-week study, comparing metformin (more than 1500 mg daily) versus metformin (1500 mg or less daily) plus glimepiride also favored the combination therapy over metformin monotherapy with a between-group difference in A1c of 0.63% [30]. Several clinical studies have observed a sustained A1c reduction with gliclazide-based therapy. The action in diabetes and vascular disease: Preterax and Diamicron MR controlled evaluation (ADVANCE) study comparing intensive gliclazide-MR-based therapy with standard therapy reported gradually reduction in A1c levels to 6.5% and then maintained them for a median of 5 years [31]. Another study found that patients with diabetes taking gliclazide can avoid escalation to insulin treatment for a longer period (14.5 years) than those taking glibenclamide (mean of 8 years) [32]. However, patients with diabetes who are inadequately controlled with oral antidiabetic drugs can benefit from the addition of once-daily insulin glargine to the gliclazide-MR regimen. In 2015, Zhou et al. demonstrated that once-daily insulin glargine plus gliclazide-MR also decrease A1c more effectively than the twice-daily premixed insulin regimen [33].
Opinions from experts on gliclazide use as second-line agent in patients with T2DM |
Combination of gliclazide/gliclazide-MR and metformin is always associated with greater reduction in A1c than metformin monotherapy (92.0%) |
Combination of gliclazide/gliclazide-MR and metformin is always associated with sustained reduction in A1c (over at least 2 years) vs. metformin monotherapy (84.9%) |
Gliclazide or gliclazide-MR preferred over GLP-1 receptor agonist owing to low cost (73.4%) |
Combination of gliclazide/gliclazide-MR and basal insulin is effective vs. basal insulin alone for patients with T2DM having reduced glycemic response with SUs (70.4%) |
Early use of metformin plus gliclazide/gliclazide-MR combination is preferred over up-titration of metformin beyond half-maximal dose (1.0 g) during the initial treatment duration of 3 months for effective management of T2DM (55.0%) |
Gliclazide or gliclazide-MR can be used as second-line treatment for patients with T2DM (add-on to metformin) if A1c level remains > 6.5% after 3 months of therapy (52.9%) |
Decision to Switch to Gliclazide/Gliclazide-MR-Based Combination Therapy from Other Combination Therapies in Uncontrolled Diabetes
Rational treatment decisions regarding second-line therapy for T2DM require a comprehensive assessment of the relative merits and disadvantages of the available therapeutic options. Several systematic reviews and meta-analyses have found that the second-line agents are similar in terms of A1c-lowering efficacy but differ concerning the attainment of an A1c goal of less than 7% [34, 35]. In 2018, Colagiuri et al. found that the percentage of patients with diabetes achieving an A1c goal was highest with the SUs (48%), followed by DPP4 inhibitors and glinides (39% for each), TZDs (33%), and AGIs (26%) [9]. Multiple studies investigating the SUs have shown adequate glycemic control with gliclazide regardless of baseline A1c level [36, 37]. A meta-analysis of 12 randomized studies (10,982 patients with T2DM) comparing DPP4 inhibitors with SUs also favored SUs regarding A1c reduction (weighted mean difference 0.105, 95% CI 0.103–0.107) [38]. However, two trials comparing SUs and sodium/glucose cotransporter 2 (SGLT2) inhibitors (added to metformin as dual therapy) reported that the A1c reduction was significantly higher with SGLT2 inhibitors compared with SUs [39, 40].
Expert opinion on switch to gliclazide/gliclazide-MR-based combination therapy from other combination therapies | |
Combination of gliclazide or gliclazide MR and metformin shows better glycemic effectiveness than AGI plus metformin in uncontrolled T2DM (53.8%) |
Efficacy of Gliclazide/Gliclazide-MR in Patients with Diabetes and CVD
CVDs are the leading cause of death among patients with diabetes, though risk was low in those taking pancreatic β-cell-specific SUs like gliclazide and glimepiride [41]. However, the EASD/ADA and ESC/EASD consensus guidelines reserve SUs for fifth-line therapy after newer agents (SGLT2i and GLP-1RA) on the basis of the evidence which suggests an increased risk of CVD with SUs compared with other newer agents [42,43,44,45]. In 2004, Katakami et al. showed that gliclazide significantly (P < 0.05) and independently reduced the progression of carotid artery intima-media thickness (atherosclerosis) as a result of its antioxidant properties [46]. The ADVANCE study also found that the intensive gliclazide-MR-based glucose control strategy reduced cardiovascular death by 12% (P = 0.12) [31]. However, the STENO-2 study reported about a 50% reduction in CVD risk with gliclazide-based intensive therapy after the mean follow-up of 7.8 years [47]. At 13.3 years of follow-up, a significantly lower risk of death from CV causes (HR 0.43, 95% CI 0.19–0.94; P = 0.04) and CV events (HR 0.41, 95% CI 0.25–0.67; P < 0.001) was observed [48]. Recent data from a 21.2-year follow-up of the STENO-2 study reported an increase of a median of 7.9 years in the patient’s lifespan attributed to the intensified multifactorial approach. This life gain was matched by the time free of incident ischemic heart disease of 8.1 years [49].
Expert opinion on gliclazide/gliclazide-MR use in patients with diabetes and CVD |
Gliclazide/gliclazide-MR is associated with lower risk of CV-related mortality as compared to old-generation SUs because of more specific action on pancreatic receptors (75.1%) |
Gliclazide/gliclazide-MR could improve endothelial function in diabetes, which may be related to its antioxidant properties (65.7%) |
Gliclazide/gliclazide-MR is favorable among SUs for reducing the left ventricular mass in patients with T2DM (57.1%) |
Efficacy of Gliclazide/Gliclazide-MR in Patients with Diabetes and CKD
The Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guideline 2020 recommends lifestyle therapy, first-line treatment with metformin and an SGLT2i, and additional drug therapy including SUs as needed for glycemic management in patients with T2D and CKD [50]. The antihyperglycemic agents should be selected and dosed according to eGFR [51]. In patients with renal diseases, the recommendation is to limit the use or avoid SUs (long-acting or cleared by the kidney) at low eGFR as inadequate clearance of SUs or its active metabolite may increase the risk for symptomatic and severe hypoglycemia [50, 52, 53]. The Kidney Disease Outcomes Quality Initiative (KDOQI) Clinical Practice Guideline for Diabetes and CKD recommends no dose adjustment for gliclazide in patients with stage 3–5 CKD, thus alleviating issues regarding dose adjustment [53]. Also, modern SUs like gliclazide and glipizide are not contraindicated by the joint position statement of the Italian Diabetes Society and the Italian Society of Nephrology in patients with renal dysfunction, since these SUs are metabolized by the liver and excreted in the urine as inactive metabolites. However, the position statement recommends dose adjustment and caution with these agents [52]. The ADVANCE study has provided data on gliclazide throughout the clinical course of renal disease. Compared with standard control, intensive glucose-control strategy involving gliclazide-MR in the ADVANCE trial significantly reduced renal events including new-onset microalbuminuria (HR 0.91, 95% CI 0.85–0.98; P = 0.02), macroalbuminuria (2.9% vs. 4.1% with standard control; HR 0.70, 95% CI 0.57–0.85; P < 0.001), new or worsening nephropathy (HR 0.79, 95% CI 0.66–0.93; P = 0.006), and need for renal replacement therapy or death from renal causes (0.4% vs. 0.6%; HR 0.64, 95% CI 0.38–1.08; P = 0.09) [54]. In 2015, Lee et al. also revealed a lower risk of sustained doubling of serum creatinine with gliclazide compared with glimepiride in patients with good controlled glycemia (A1c less than 7%, HR 0.35, 95% CI 0.14–0.86), preserved renal function (GFR at least 60 mL/min/1.73 m2, HR 0.21, 95% CI 0.04–0.99), and older age (62 years or older, HR 0.52, 95% CI 0.27–0.99), suggesting that gliclazide may have a protective role against renal disease progression [55]. This unique clinical benefit of gliclazide-MR in renal protection may be explained in part by its antioxidant properties.
Expert opinion on gliclazide/gliclazide-MR use in patients with diabetes and CKD |
Gliclazide/gliclazide-MR has a lower risk for prolonged and severe hypoglycemia owing to its metabolism to inactive metabolites in patients with CKD (79.6%) |
Gliclazide/gliclazide-MR is associated with a significantly lower risk for the development of sustained doubling of serum creatinine in patients with preserved renal function (69.8%) |
Gliclazide/gliclazide-MR is the preferred treatment option to improve glycemic control and prevent diabetic nephropathy (69.2%) |
Gliclazide/gliclazide-MR could improve diabetic nephropathy, which may be related to its antioxidant properties (52.1%) |
Safety and Tolerability of Gliclazide/Gliclazide-MR
Once-daily dosing of gliclazide-MR has been associated with higher compliance rate (odds ratio [OR] 3.50, 95% CI 1.73, 7.08; P < 0.001) and adherence rate (OR 3.07, 95% CI 1.80, 5.23; P < 0.001) compared with more than once-daily dosing [56]. Gliclazide-MR also has a lower risk of hypoglycemia compared to other SUs as it gets metabolized into inactive metabolites and a gradual increase in drug concentrations [9]. This finding was supported by a meta-analysis which found a significantly lower risk of hypoglycemia with gliclazide compared with other SUs (risk ratio [RR] 0.47, 95% CI 0.77–0.70; P = 0.004) [57]. However, a meta-analysis comparing DPP4 inhibitors with SUs found a lower risk of hypoglycemia with DPP4 inhibitors (OR 0.13, 95% CI 0.11–0.16) [38]. Similarly, another meta-analysis (13 studies, n = 5175) found a lower risk for hypoglycemia with SGLT2 inhibitors when compared with SUs [58].
When considered as a class, SU monotherapy has been reported to cause a weight gain of 1.5–2.5 kg [59]. In the ADVANCE study, there was a gain of 0.1 kg weight and frequent hypoglycemia (12 per 1000 patient-years) in the intensive gliclazide MR-based glucose control group compared to 0.8 kg weight reduction and nine episodes of hypoglycemia per 1000 patient-years in the standard control group over the 5 years of follow-up. However, a mean weight loss of 0.5 kg was observed in people with obesity (BMI 30 kg/m2 or higher) when analyzed by baseline BMI subgroup [60]. Data from thiazolidinediones or sulfonylureas cardiovascular accidents intervention trial (TOSCA.IT) showed a moderate weight gain (less than 2 kg, on average) in both pioglitazone and SUs groups while the Rosiglitazone Evaluated for Cardiac Outcomes and Regulation of Glycaemia in Diabetes (RECORD) trial showed no increase in the weight of patients allocated to dual therapy with metformin and a SU [61, 62].
Expert opinion on safety and tolerability of gliclazide/gliclazide-MR |
Gliclazide-MR once-daily approach also improves compliance (81.4%) |
Risk of hypoglycemia is also low with gliclazide vs. older SUs (79.3%) |
Gliclazide-MR once daily is a more effective and well-tolerable approach than gliclazide twice daily in patients with T2DM (68.6%) |
Dosing of Gliclazide-MR
The dose of gliclazide-MR may vary from 30 to 120 mg once daily and should be adjusted according to clinical response. The recommended starting dose for gliclazide-MR is 30 mg daily. If blood glucose is not adequately controlled, the dose may be increased to 60, 90, or 120 mg daily, in successive steps. The interval between each dose increment should be at least 1 month except in patients whose blood glucose has not been reduced after 2 weeks of treatment. In such cases, the dose may be increased at the end of the second week of treatment. The maximum recommended daily dose is 120 mg. In the observational study to analyze titration of Diamicron MR 60 mg (EASYDia) study, a step-by-step intensification of the gliclazide-MR formulation (up to 120 mg once daily) helped the patients with diabetes and different baseline target values to achieve glycemic control as the difference between those taking gliclazide-MR 30 mg and gliclazide-MR 120 mg at month 6 was 1.1 mmol/L for fasting plasma glucose (FPG) [17]. The Xrise study investigating the once-daily breakable gliclazide extended-release (XR) 60 mg in patients with T2D (n = 679), uncontrolled with diet alone or metformin monotherapy, reported effective glycemic control with a low frequency of hypoglycemia. At month 4, FPG was reduced by 66.0 (61.1–70.9, P < 0.01) mg/dl with one tablet, by 80.1 (71.2–88.5, P < 0.01) mg/dl with 1.5 tablets, and by 106.5 (93.4–119.5, P < 0.01) mg/dl with two tablets from baseline in patients with T2DM [63].
Expert opinion on dosing of gliclazide-MR |
The usual starting dose for gliclazide-MR is 30–60 mg administered once daily with the morning/evening main meal (85.2%) |
Initiating gliclazide/gliclazide-MR with the higher dose when the A1c target is more than 0.5% from the prevailing A1c level increases the likelihood of achieving A1c goals (76.0%) |
The dose can be escalated by 30 to 60 mg every 1–4 weeks, guided by fasting glucose levels (73.6%) |
Gliclazide/Gliclazide-MR in Special Populations
Careful selection of antidiabetic agents paying particular attention to drug safety and the risk of hypoglycemia is important in optimizing diabetic therapy for older people with T2DM. In 1994, Tessier et al. compared glibenclamide with gliclazide for the frequency of hypoglycemic events and glycemic control in older people (more than 71 years of age) with T2DM. They found comparable glycemic control (A1c glibenclamide 7.4 ± 0.2% vs. gliclazide 7.9 ± 0.5%; P = not significant)] at 6 months with both drugs, but the incidence of hypoglycemic episodes was significantly greater with glibenclamide when compared with gliclazide [64]. A subgroup analysis comparing gliclazide-MR versus glimepiride in patients with diabetes and more than 75 years of age found that most hypoglycemic episodes occurred at the lowest treatment doses (15 on 30–60 mg gliclazide-MR out of 22 episodes, and 48 on glimepiride 1–2 mg out of 56 episodes) [21].
Expert opinion on gliclazide/gliclazide-MR use in special populations | |
Gliclazide is a safe option for older patients with T2DM (68.1%) |
Limitation of the Survey
Limitation of this Delphi survey is the single round design. Another shortcoming includes a lower response rate for some statements in this survey, though face-to-face contact with participants has been found useful in increasing the response rate. Consideration must be given to the fact that individual time constraints and lack of familiarity with the Delphi technique may have prevented some participants from being able to make responses on time. Nonetheless, the quality of the responses provided made clear that those who did take part were firmly committed to offering us detailed and extremely thoughtful answers to our statements. The findings may offer an overly optimistic picture. This needs to be borne in mind when interpreting the findings.
Conclusion
When deciding on a treatment strategy for diabetes it is essential to consider both patient- and drug-specific characteristics. The collaborative Delphi methodology provided expert consensus-based opinion which could help to justify the role of gliclazide in different clinical situations associated with diabetes. Although gliclazide has the risk of mild hypoglycemia, and small weight gain, it is preferred in patients with T2DM because of its sustained glycemic efficacy maintained over the long term, unique end stage kidney disease prevention, and CV safety at lower cost.
References
Misra A, Gopalan H, Jayawardena R, et al. Diabetes in developing countries. J Diabetes. 2019;11(7):522–39.
Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res Clin Pract. 2019;157:107843.
Singla R, Bindra J, Singla A, Gupta Y, Kalra S. Drug prescription patterns and cost analysis of diabetes therapy in India: audit of an endocrine practice. Indian J Endocrinol Metab. 2019;23(1):40–5.
American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes—2020. Diabetes Care. 2020;43(Suppl 1):S98.
International Diabetes Federation. IDF clinical practice recommendations for managing type 2 diabetes in primary care. IDF. 2020. https://www.idf.org/e-library/guidelines/128-idf-clinical-practice-recommendations-for-managing-type-2-diabetes-in-primary-care.html. Accessed 16 Dec 2020.
Kalra S, Aamir AH, Raza A, et al. Place of sulfonylureas in the management of type 2 diabetes mellitus in South Asia: a consensus statement. Indian J Endocrinol Metab. 2015;19(5):577–96.
Chawla R, Madhu SV, Makkar BM, Ghosh S, Saboo B, Kalra S. RSSDI-ESI clinical practice recommendations for the management of type 2 diabetes mellitus 2020. Indian J Endocrinol Metab. 2020;24(1):1–122.
Rutten G, De Grauw W, Nijpels G, et al. NHG-Standaard Diabetes mellitus type 2 (derde herziening). Huisarts Wet. 2013;56(10):512–25.
Colagiuri S, Matthews D, Leiter LA, Chan SP, Sesti G, Marre M. The place of gliclazide MR in the evolving type 2 diabetes landscape: a comparison with other sulfonylureas and newer oral antihyperglycemic agents. Diabetes Res Clin Pract. 2018;143:1–14.
Jarvis JD, Woods H, Bali A, Oronsaye E, Persaud N. Selection of WHO-recommended essential medicines for non-communicable diseases on National Essential Medicines Lists. PLoS One. 2019;14(8):e0220781.
Rauch W. The decision Delphi. Technol Forecast Soc Chang. 1979;15(3):159–69.
American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: Standards of Medical Care in Diabetes—2019. Diabetes Care. 2019;42(Supplement 1):S90–102.
Aschner P. New IDF clinical practice recommendations for managing type 2 diabetes in primary care. Diabetes Res Clin Pract. 2017;132:169–70.
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35(6):1364–79.
Foley JE, Sreenan S. Efficacy and safety comparison between the DPP-4 inhibitor vildagliptin and the sulfonylurea gliclazide after two years of monotherapy in drug-naïve patients with type 2 diabetes. Horm Metab Res. 2009;41(12):905–9.
Landman GW, de Bock GH, van Hateren KJ, et al. Safety and efficacy of gliclazide as treatment for type 2 diabetes: a systematic review and meta-analysis of randomized trials. PLoS One. 2014;9(2):e82880.
Leiter LA, Shestakova MV, Satman I. Effectiveness of gliclazide MR 60 mg in the management of type 2 diabetes: analyses from the EASYDia trial. Diabetol Metab Syndr. 2018;10:30.
Rodbard HW, Jellinger PS, Davidson JA, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract. 2009;15(6):540–59.
Kalra S, Bahendeka S, Sahay R, et al. Consensus recommendations on sulfonylurea and sulfonylurea combinations in the management of type 2 diabetes mellitus—International Task Force. Indian J Endocrinol Metab. 2018;22(1):132–57.
Bolen S, Tseng E, Hutfless S, et al. Diabetes medications for adults with type 2 diabetes: an update. 2016. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Apr. Report No.: 16-EHC013-EF.
Schernthaner G, Grimaldi A, Di Mario U, et al. GUIDE study: double-blind comparison of once-daily gliclazide MR and glimepiride in type 2 diabetic patients. Eur J Clin Invest. 2004;34(8):535–42.
Royal Australian College of General Practitioners. General practice management of type 2 diabetes: 2016–18. RACGP. 2016. https://www.racgp.org.au/FSDEDEV/media/documents/Clinical%20Resources/Guidelines/Diabetes/General-practice-management-of-type-2-diabetes_1.pdf. Accessed 21 Jan 2020.
Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2018;61(12):2461–98.
World Health Organization. Guidelines on second-and third-line medicines and type of insulin for the control of blood glucose levels in non-pregnant adults with diabetes mellitus. Guidelines on second-and third-line medicines and type of insulin for the control of blood glucose levels in non-pregnant adults with diabetes mellitus. 2018. Geneva: WHO.
Ahrén B, Mathieu C, Bader G, Schweizer A, Foley JE. Efficacy of vildagliptin versus sulfonylureas as add-on therapy to metformin: comparison of results from randomised controlled and observational studies. Diabetologia. 2014;57(7):1304–7.
Yang W, Chen L, Ji Q, et al. Liraglutide provides similar glycaemic control as glimepiride (both in combination with metformin) and reduces body weight and systolic blood pressure in Asian population with type 2 diabetes from China, South Korea and India: a 16-week, randomized, double-blind, active control trial. Diabetes Obes Metab. 2011;13(1):81–8.
Derosa G, Putignano P, Bossi AC, et al. Exenatide or glimepiride added to metformin on metabolic control and on insulin resistance in type 2 diabetic patients. Eur J Pharmacol. 2011;666(1–3):251–6.
Derosa G, Maffioli P, Salvadeo SA, et al. Effects of sitagliptin or metformin added to pioglitazone monotherapy in poorly controlled type 2 diabetes mellitus patients. Metabolism. 2010;59(6):887–95.
Li Z, Zhang Y, Quan X, et al. Efficacy and acceptability of glycemic control of glucagon-like peptide-1 receptor agonists among type 2 diabetes: a systematic review and network meta-analysis. PLoS One. 2016;11(5):e0154206.
Ahrén B, Johnson SL, Stewart M, et al. HARMONY 3: 104-week randomized, double-blind, placebo- and active-controlled trial assessing the efficacy and safety of albiglutide compared with placebo, sitagliptin, and glimepiride in patients with type 2 diabetes taking metformin. Diabetes Care. 2014;37(8):2141–8.
Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–72.
Satoh J, Takahashi K, Takizawa Y, et al. Secondary sulfonylurea failure: comparison of period until insulin treatment between diabetic patients treated with gliclazide and glibenclamide. Diabetes Res Clin Pract. 2005;70(3):291–7.
Zhou J, Zheng F, Guo X, et al. Glargine insulin/gliclazide MR combination therapy is more effective than premixed insulin monotherapy in Chinese patients with type 2 diabetes inadequately controlled on oral antidiabetic drugs. Diabetes Metab Res Rev. 2015;31(7):725–33.
McIntosh B, Cameron C, Singh SR, Yu C, Dolovich L, Houlden R. Choice of therapy in patients with type 2 diabetes inadequately controlled with metformin and a sulphonylurea: a systematic review and mixed-treatment comparison meta-analysis. Open Med. 2012;6(2):e62-74.
Phung OJ, Scholle JM, Talwar M, Coleman CI. Effect of noninsulin antidiabetic drugs added to metformin therapy on glycemic control, weight gain, and hypoglycemia in type 2 diabetes. JAMA. 2010;303(14):1410–8.
Makrilakis K. The role of DPP-4 inhibitors in the treatment algorithm of type 2 diabetes mellitus: when to select, what to expect. Int J Environ Res Public Health. 2019;16(15):2720.
Polavarapu NK, Kale R, Sethi B, et al. Effect of gliclazide or gliclazide plus metformin combination on glycemic control in patients with T2DM in India: a real-world, retrospective, longitudinal, observational study from electronic medical records. Drugs Real World Outcomes. 2020;7(4):271–9.
Zhang Y, Hong J, Chi J, Gu W, Ning G, Wang W. Head-to-head comparison of dipeptidyl peptidase-IV inhibitors and sulfonylureas - a meta-analysis from randomized clinical trials. Diabetes Metab Res Rev. 2014;30(3):241–56.
Ridderstråle M, Andersen KR, Zeller C, Kim G, Woerle HJ, Broedl UC. Comparison of empagliflozin and glimepiride as add-on to metformin in patients with type 2 diabetes: a 104-week randomised, active-controlled, double-blind, phase 3 trial. Lancet Diabetes Endocrinol. 2014;2(9):691–700.
Del Prato S, Nauck M, Durán-Garcia S, et al. Long-term glycaemic response and tolerability of dapagliflozin versus a sulphonylurea as add-on therapy to metformin in patients with type 2 diabetes: 4-year data. Diabetes Obes Metab. 2015;17(6):581–90.
Simpson SH, Lee J, Choi S, Vandermeer B, Abdelmoneim AS, Featherstone TR. Mortality risk among sulfonylureas: a systematic review and network meta-analysis. Lancet Diabetes Endocrinol. 2015;3(1):43–51.
Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycemia in type 2 diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41(12):2669–701.
Cosentino F, Grant PJ, Aboyans V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41(2):255–323.
Ekström N, Svensson AM, Miftaraj M, et al. Cardiovascular safety of glucose-lowering agents as add-on medication to metformin treatment in type 2 diabetes: report from the Swedish National Diabetes Register. Diabetes Obes Metab. 2016;18(10):990–8.
Mogensen UM, Andersson C, Fosbøl EL, et al. Metformin in combination with various insulin secretagogues in type 2 diabetes and associated risk of cardiovascular morbidity and mortality–a retrospective nationwide study. Diabetes Res Clin Pract. 2015;107(1):104–12.
Katakami N, Yamasaki Y, Hayaishi-Okano R, et al. Metformin or gliclazide, rather than glibenclamide, attenuate progression of carotid intima-media thickness in subjects with type 2 diabetes. Diabetologia. 2004;47(11):1906–13.
Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med. 2003;348(5):383–93.
Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358(6):580–91.
Oellgaard J, Gæde P, Rossing P, et al. Reduced risk of heart failure with intensified multifactorial intervention in individuals with type 2 diabetes and microalbuminuria: 21 years of follow-up in the randomised Steno-2 study. Diabetologia. 2018;61(8):1724–33.
Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2020;98(4s):S1-S115.
Neumiller JJ, Alicic RZ, Tuttle KR. Therapeutic considerations for antihyperglycemic agents in diabetic kidney disease. J Am Soc Nephrol. 2017;28(8):2263–74.
Pugliese G, Penno G, Natali A, et al. Diabetic kidney disease: new clinical and therapeutic issues. Joint position statement of the Italian Diabetes Society and the Italian Society of Nephrology on “The natural history of diabetic kidney disease and treatment of hyperglycemia in patients with type 2 diabetes and impaired renal function.” J Nephrol. 2020;33(1):9–35.
KDOQI Clinical Practice Guideline for Diabetes and CKD. 2012 Update. Am J Kidney Dis. 2012;60(5):850–86.
Perkovic V, Heerspink HL, Chalmers J, et al. Intensive glucose control improves kidney outcomes in patients with type 2 diabetes. Kidney Int. 2013;83(3):517–23.
Lee YH, Lee CJ, Lee HS, et al. Comparing kidney outcomes in type 2 diabetes treated with different sulphonylureas in real-life clinical practice. Diabetes Metab. 2015;41(3):208–15.
Srivastava K, Arora A, Kataria A, Cappelleri JC, Sadosky A, Peterson AM. Impact of reducing dosing frequency on adherence to oral therapies: a literature review and meta-analysis. Patient Prefer Adher. 2013;7:419–34.
Chan SP, Colagiuri S. Systematic review and meta-analysis of the efficacy and hypoglycemic safety of gliclazide versus other insulinotropic agents. Diabetes Res Clin Pract. 2015;110(1):75–81.
Vasilakou D, Karagiannis T, Athanasiadou E, et al. Sodium-glucose cotransporter 2 inhibitors for type 2 diabetes: a systematic review and meta-analysis. Ann Intern Med. 2013;159(4):262–74.
Nichols GA, Gomez-Caminero A. Weight changes following the initiation of new anti-hyperglycaemic therapies. Diabetes Obes Metab. 2007;9(1):96–102.
Zoungas S, Chalmers J, Kengne AP, et al. The efficacy of lowering glycated haemoglobin with a gliclazide modified release-based intensive glucose lowering regimen in the ADVANCE trial. Diabetes Res Clin Pract. 2010;89(2):126–33.
Vaccaro O, Masulli M, Nicolucci A, et al. Effects on the incidence of cardiovascular events of the addition of pioglitazone versus sulfonylureas in patients with type 2 diabetes inadequately controlled with metformin (TOSCA.IT): a randomised, multicentre trial. Lancet Diabetes Endocrinol. 2017;5(11):887–97.
Home PD, Pocock SJ, Beck-Nielsen H, et al. Rosiglitazone evaluated for cardiovascular outcomes in oral agent combination therapy for type 2 diabetes (RECORD): a multicentre, randomised, open-label trial. Lancet. 2009;373(9681):2125–35.
Mohan V, Chopra V, Sanyal D, Jain S, Jayaprakashsai J. Treatment of type 2 diabetes with a breakable extended release gliclazide formulation in primary care: the Xrise Study. J Assoc Phys India. 2015;63(12):26–9.
Tessier D, Dawson K, Tétrault JP, Bravo G, Meneilly GS. Glibenclamide vs gliclazide in type 2 diabetes of the elderly. Diabet Med. 1994;11(10):974–80.
Acknowledgements
Dr. Reddy Laboratories India helped in the organization and logistic support for this expert forum meeting. The content published herein represents the views and opinions of the various contributing authors and does not necessarily represent the views or opinion of Dr. Reddy Laboratories and/or its affiliates. The details published herein are intended for informational, educational, academic, and/or research purposes and are not intended to substitute for professional medical advice, diagnosis, or treatment. The authors would also like to thank the panel of experts for their participation in the Delphi study.
Funding
Sponsorship for this study and Rapid Service Fee were funded by Dr. Reddy Laboratories Pvt. Ltd.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Medical Writing, Editorial, and Other Assistance
Medical writing assistance was provided by Dr. Rajiv Kumar and Dr. Ankit Pathak from WorkSure India. Support for this assistance was funded by Dr. Reddy Laboratories Pvt. Ltd.
Disclosure
Dr. Sanjay Kalra is the editorial board member of the Diabetes Therapy journal; Dr Nareen Krishna Polavarapu and Dr. Kumar Gaurav are employees of Dr. Reddy’s Laboratories Limited, Hyderabad, India. Dr. Sanjay Kalra, Dr. Unnikrishnan A G, Dr. Sambit Das and Dr. Ganapathi Bantwal have received speaker/honorarium fees form Dr. Reddy’s Laboratories Ltd.
Compliance with Ethics Guidelines
This study is based on a clinical practice questionnaire that does not involve the participation of human subjects nor patient data management and does not aim to modify the current clinical practice of participants. Consequently, as per ethical approval procedures in India, the questionnaires compiled in this study did not require ethical approval. Consent for publication of survey results was granted from all the experts participating in the program and undertaking the survey.
Data Availability
All data generated or analyzed during this study are included in this published article/as supplementary information files.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Kalra, S., Unnikrishnan, A.G., Bantwal, G. et al. The Position of Gliclazide in the Evolving Landscapes and Disease Continuum of T2DM: A Collaborative Delphi Survey-Based Consensus from India. Diabetes Ther 12, 679–695 (2021). https://doi.org/10.1007/s13300-021-01002-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-021-01002-4