
Abstract
Background
In type 2 diabetes mellitus (T2DM), progressive loss of beta cell function over time requires treatment intensification and eventually initiation of insulin for many patients. Relative to metformin, a greater rate of decline in beta cell function over time has been observed with sulfonylurea treatment. The present study examined the association between initial monotherapy with metformin or sulfonylurea and subsequent initiation of insulin in older subjects with T2DM.
Methods
In a retrospective cohort study using the GE electronic medical record database, eligible subjects with T2DM included those ≥65 years who received their first prescription of sulfonylurea or metformin as initial monotherapy between January 1, 2003 to December 31, 2008. The follow-up period lasted to the end of 2009 or the subject’s latest data available. Insulin initiation was determined by prescription records. Logistic regression analysis evaluated the likelihood of insulin addition. A Cox regression model estimated time to initiation of insulin. Differences in baseline characteristics were controlled for using propensity score matching.
Results
Overall, 12,036 subjects were included in the analysis. Mean age was 75 years and 50% were male. Subjects who initiated with sulfonylurea had a significantly (P < 0.001) higher incidence of insulin addition (2.8% vs. 1.4%) compared to those initiated with metformin within 1 year of follow-up. The likelihood of initiating insulin was higher in subjects initiated with sulfonylurea than with metformin (adjusted odds ratio 1.82, 95% confidence interval [CI] 1.40–2.38; P < 0.001). Sulfonylurea use was also significantly associated with a shorter time to insulin use compared to metformin (adjusted hazards ratio 2.10, 95% CI 1.83–2.39; P < 0.001).
Conclusion
In a cohort of older subjects with T2DM initiating antihyperglycemic therapy, new users of sulfonylurea monotherapy were more likely to receive insulin therapy and received it earlier than those starting with metformin.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Type 2 diabetes mellitus (T2DM) is characterized by hyperglycemia related to a progressive loss of beta cell function [1]. The selection of initial antihyperglycemic therapy influences treatment failure and the need for additional therapy in individuals with T2DM [2]. Metformin and sulfonylureas are the two most commonly prescribed oral antihyperglycemic agents for initial therapy for T2DM because of their well-defined clinical profiles and cost [3]. These agents work by distinct mechanisms, with metformin primarily reducing hepatic glucose production and insulin resistance, and sulfonylureas stimulating insulin release by binding to their receptor on the pancreatic beta cell. In recently diagnosed patients with T2DM, monotherapy treatment with the sulfonylurea, glyburide, was associated with an increased likelihood of treatment failure compared with metformin (and rosiglitazone) over 4 years [4]. Despite a larger initial (within 6 months) increase in beta cell function with glyburide, greater treatment failure with glyburide was related to a greater decline in beta cell function overall relative to metformin (and rosiglitazone) [4, 5].
Beta cell function also declines with aging [6]. In older individuals with T2DM, sulfonylurea use tends to increase and metformin use declines [7–9]. Given the greater loss of beta cell function over time with sulfonylureas and the reduced beta cell function associated with aging, the present retrospective observational study was performed to examine the influence of initial monotherapy with metformin or a sulfonylurea on the subsequent use of insulin therapy in older subjects with T2DM.
Observational studies are used to estimate treatment effects when randomized controlled trials are not feasible. However, the lack of randomization may lead to imbalances in subject characteristics due to channeling bias [10]. Differences in baseline characteristics must be adjusted for in order to minimize channeling bias and determine treatment effect. Propensity score matching is a statistical technique used to generate well-defined cohorts matched on specific baseline characteristics in order to control for potential confounding [11]. Therefore, the present analysis used propensity score matching to generate two well-matched cohorts of older subjects initially treated with metformin or a sulfonylurea.
Methods
Study Design and Subject Selection
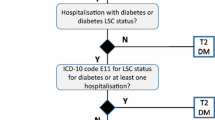
Data for this retrospective cohort study of US subjects were obtained using GE Healthcare’s Clinical Data Services electronic medical record database. For the index period of January 1, 2003 to December 31, 2008, subjects with newly or previously diagnosed T2DM were included in the analysis if they were at least 65 years of age, received their first prescription for metformin or sulfonylurea as monotherapy during the index period, and continued monotherapy for at least 90 days following the index date (i.e., date of first prescription, Fig. 1). Subjects also had to have no prescriptions for any antihyperglycemic agents within the 1-year period prior to the index date, and were required to be continually enrolled in the database for at least 1 year before the index date (i.e., baseline data), and to have at least 1 year of follow-up data. The follow-up period was censored at the end of 2009 or the date of the subjects’ latest available data.

Study design
The 1-year period before the index date was used to ensure adequate time to capture baseline characteristics on all subjects. Baseline variables included the following measurements: age, gender, body mass index, blood pressure, and laboratory measurements (glycated hemoglobin [HbA1c], total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, serum creatinine, and liver enzymes). History of cardiovascular conditions, microvascular complications, renal and liver disease, and smoking were collected in the baseline period. Due to the nature of the database and limited baseline collection period used, the duration of diabetes was not assessed. The presence of T2DM and baseline history of cardiovascular or microvasculature events were identified in the database using the International Classification of Diseases, Ninth revision diagnosis/procedure and Current Procedural Terminology codes.
Outcomes
The proportion of subjects initiating insulin therapy during the 1-year follow-up period was the primary outcome of interest. Factors influencing the likelihood of or time to initiating insulin therapy were also evaluated. The time from initial oral monotherapy with metformin or sulfonylurea to insulin initiation was estimated based on prescription records. Additional analyses extended the follow-up period to 2 or 3 years.
Statistical Analysis
To control for confounding, propensity score matching was used to generate matched cohorts of subjects treated with metformin or sulfonylurea monotherapy and at least 1 year of follow-up data. A multivariate logistic regression model was constructed first to calculate the propensity score, defined as the conditional probability of initiating sulfonylurea versus metformin monotherapy as a function of all measured baseline factors described above. A one-to-one greedy matching algorithm was employed as the next step to match propensity scores of the two treatment cohorts from best to next best [12]. Best matches were defined as pairs with the highest digit match (0.00001) on propensity score. The matching algorithm proceeded sequentially to the next highest digit match. No more matches can be made below the lowest allowable digit 0.1.
Data are presented as the mean or proportion for each treatment group (metformin or sulfonylurea). To confirm adequate matching, between-group differences in the baseline characteristics were assessed with t tests for continuous variables and χ2 tests for categorical variables. Significance was assessed at P < 0.05. Logistic regression analyses were used to estimate the odds ratio (OR) associated with the likelihood of initiating insulin therapy within the fixed follow-up period. A Cox proportional hazards regression model was used to estimate the time to insulin initiation. The regression analyses were adjusted for baseline characteristics. Additional analyses were based on matched cohorts with at least 2 or 3 years of follow-up data.
Results
Of the 20,764 older subjects with T2DM who received their first prescription with metformin or sulfonylurea and had at least 1 year of follow-up data, matched cohorts of 6,018 subjects per treatment were generated using propensity score matching (Table 1). Baseline demographics, laboratory measures, and comorbid conditions for these well-matched cohorts are shown in Table 2. Briefly, these subjects (50% male) had a mean age of 75 years, mean body mass index of 31 kg/m2, and mean HbA1c of 7.2% (Table 2).
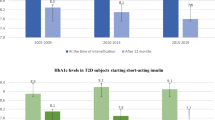
The proportion of subjects initiating insulin within 1 year was significantly higher (2.8% vs. 1.4%; P < 0.001) with sulfonylurea compared to metformin (Fig. 2). After adjusting for baseline characteristics, the likelihood of initiating insulin therapy within 1 year of follow-up was higher in subjects who started with sulfonylurea monotherapy than with metformin (adjusted OR 1.82, 95% confidence interval [CI] 1.40–2.38; P < 0.001). Higher HbA1c and elevated serum creatinine were also associated with initiating insulin therapy (Table 3). Male gender was associated with a lower likelihood of initiating insulin therapy. Sulfonylurea use was also associated with a shorter time to initiating insulin therapy compared to metformin (adjusted hazards ratio 2.10, 95% CI 1.83–2.39; P < 0.001) (Table 4). Higher HbA1c and elevated serum creatinine were associated with a shorter time to initiating insulin therapy (Table 4).

Proportion of subjects who initiated insulin within 1, 2, or 3 years after starting monotherapy with metformin or sulfonylurea (see text for number of subjects per treatment group at each time point)
In an analysis using matched cohorts with at least 2 years of follow-up data (n = 4,691 per treatment), significantly more subjects initiated with sulfonylurea therapy started insulin therapy compared to those initiated with metformin (Fig. 2). After adjusting for baseline characteristics for this cohort, the likelihood of initiating insulin therapy within 2 years of follow-up was higher in subjects initiated with sulfonylurea than with metformin (adjusted OR 2.27, 95% CI 1.82–2.82; P < 0.001).
Similar results were identified for a matched cohorts with at least 3 years of follow-up data (n = 3,312 per treatment). Significantly more subjects initiated with sulfonylurea therapy started insulin therapy compared to those initiated with metformin (Fig. 2). After adjusting for baseline characteristics for this cohort, the likelihood of initiating insulin therapy within 3 years of follow-up was also higher in subjects initiated with sulfonylurea than with metformin (adjusted OR 1.98, 95% CI 1.59–2.45; P < 0.001).
Discussion
The present study evaluated the effect of initial treatment with metformin or sulfonylurea monotherapy on subsequent treatment intensification with insulin therapy in US subjects with T2DM and aged ≥65 years. Older adults with T2DM were examined because older age is associated with reduced beta cell function [6]. Thus, any treatments with negative effects on beta cell function may increase the requirement for insulin therapy in this population. Comparisons between treatments may be confounded by channeling bias and the present study attempts to control for this by using propensity score matching [10]. In the present study in two well-matched groups of older subjects, approximately twice as many subjects initiated insulin therapy within 1, 2, or 3 years of receiving their first prescription for sulfonylurea monotherapy compared with metformin monotherapy. The annualized rates of insulin initiation were approximately 1.5% for those started with metformin and 3% for those started with sulfonylureas. These rates on insulin initiation are generally similar to the annualized rates reported for a Canadian (1%) and a Swedish cohort (3.5%) of patients who initiated therapy with an oral antihyperglycemic agent [13, 14]. Furthermore, initiating treatment with sulfonylurea monotherapy was significantly associated with a shorter time to insulin use compared to initiating with metformin monotherapy.
The present results in US subjects are generally consistent with those in cohort studies from other countries. In a cohort of older Canadian subjects with T2DM (age ≥ 66 years), new users of insulin secretagogues (including sulfonylureas) were more likely to initiate insulin therapy than new users of metformin [13]. In a Swedish cohort of subjects with T2DM, initial metformin monotherapy use was associated with a lower probability of initiating insulin relative to non-metformin therapy (primarily sulfonylurea) [14]. In a German cohort, treatment with a sulfonylurea was associated with a higher probability of initiating insulin therapy compared with metformin [15]. Furthermore, initial monotherapy with sulfonylurea led to more subsequent use of insulin relative to metformin use in cohorts from Scotland [16] and Canada [17]. Although these studies did not specifically match cohorts of initial metformin and sulfonylurea users for baseline characteristics, it is apparent that sulfonylurea use relative to metformin is an important factor contributing to the initiation of insulin therapy.
Secondary failure occurs with all types of antihyperglycemic treatments [2, 4, 18]. Secondary failure with sulfonylureas has been associated with desensitization of insulin secretion to prolonged exposure to sulfonylureas [19] and sulfonylurea-induced apoptosis of the beta cell [20–22]. Conversely, metformin reduces hepatic glucose output and increases insulin sensitivity; thus potentially reducing the burden on the beta cell to secrete insulin. The results of the present study suggest that selecting a treatment that is not associated with negative effects on an underlying pathophysiology of T2DM (i.e., declining beta cell function) prolongs the time from treatment initiation to intensification with insulin therapy. The difference may even be greater depending on the type of sulfonylurea, as there are differences in secondary failure within this class [23].
Baseline factors were also associated with initiating insulin therapy, including worse glycemic control and elevated serum creatinine. Higher HbA1c was a significant factor leading to insulin initiation in other cohort studies [14–16]. These factors may have precipitated more office visits and, hence, more opportunity for physicians to intensify or alter antihyperglycemic treatment with insulin.
There are several strengths and limitations related to this analysis. With regard to strengths, the study included large, well-matched cohorts of >6,000 subjects per treatment with at least 1 year of follow-up data. Similar findings in matched cohorts with 2 or 3 years of follow-up data also lend support to the robustness of the present findings. However, the following limitations need to be considered when interpreting the present results. This was a retrospective study and subjects were not randomly assigned to initial treatments. Although propensity score matching generated well-matched cohorts, additional factors that were not available from the data and, thus, were not accounted for (e.g., measures of on-treatment glycemic control, duration of diabetes) may have influenced the results. Subjects were only required to be on monotherapy for 90 days for inclusion in the analysis population, and subsequent discontinuation or switching of initial therapy or prescriptions for additional oral antihyperglycemic therapies were not accounted for in this analysis. This approach is similar-to-intent to treat within clinical trial studies. Finally, changes in treatment paradigms for T2DM and the availability of additional antihyperglycemic therapies over time may have contributed to the differences between groups.
Conclusion
In a US cohort of older subjects with T2DM initiating antihyperglycemic therapy, new users of sulfonylurea monotherapy were more likely to receive insulin therapy and received it earlier than those who started with metformin monotherapy.
References
UK Prospective Diabetes Atudy 16. Overview of 6 years’ therapy of type II diabetes: a progressive disease. Diabetes. 1995;44:1249–58.
Turner RC, Cull CA, Frighi V, Holman RR. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49). UK Prospective Diabetes Study (UKPDS) Group. JAMA. 1999;281:2005–12.
Inzucchi SE. Oral antihyperglycemic therapy for type 2 diabetes: scientific review. JAMA. 2002;287:360–72.
Kahn SE, Haffner SM, Heise MA, ADOPT Study Group, et al. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med. 2006;355:2427–43.
Kahn SE, Lachin JM, Zinman B, ADOPT Study Group, et al. Effects of rosiglitazone, glyburide, and metformin on beta-cell function and insulin sensitivity in ADOPT. Diabetes. 2011;60:1552–60.
Gong Z, Muzumdar RH. Pancreatic function, type 2 diabetes, and metabolism in aging. Int J Endocrinol. 2012;2012:320482.
Zhang Q, Rajagopalan S, Marrett E, Davies MJ, Radican L, Engel SS. Time to treatment initiation with oral antihyperglycaemic therapy in US patients with newly diagnosed type 2 diabetes. Diabetes Obes Metab. 2012;14:149–54.
Sinclair AJ, Alexander CM, Davies MJ, Zhao C, Mavros P. Factors associated with initiation of antihyperglycaemic medication in UK patients with newly diagnosed type 2 diabetes. BMC Endocr Disord. 2012;12:1.
Riedel AA, Heien H, Wogen J, Plauschinat CA. Loss of glycemic control in patients with type 2 diabetes mellitus who were receiving initial metformin, sulfonylurea, or thiazolidinedione monotherapy. Pharmacotherapy. 2007;27:1102–10.
Lobo FS, Wagner S, Gross CR, Schommer JC. Addressing the issue of channeling bias in observational studies with propensity scores analysis. Res Social Adm Pharm. 2006;2:143–51.
Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects. Biometrika. 1983;70:41–55.
Parsons LS. Reducing bias in a propensity score matched-pair sample using greedy matching techniques (paper 214–26). Paper presented at: SUGI 26 Proceedings (Proceedings of the 26th annual SAS users group international conference), Long Beach, CA, April 22–25, 2001; Cary, NC.
Perez N, Moisan J, Sirois C, Poirier P, Gregoire JP. Initiation of insulin therapy in elderly patients taking oral antidiabetes drugs. Can Med Assoc J. 2009;180:1310–6.
Ringborg A, Lindgren P, Yin DD, Martinell M, Stalhammar J. Time to insulin treatment and factors associated with insulin prescription in Swedish patients with type 2 diabetes. Diabetes Metab. 2010;36:198–203.
Kostev K, Dippel FW. Predictors for the initiation of a basal supported oral therapy (BOT) in type 2 diabetic patients under real-life conditions in Germany. Prim Care Diabetes. 2012 (Epub ahead of print).
Donnan PT, Steinke DT, Newton RW, Morris AD. Changes in treatment after the start of oral hypoglycaemic therapy in type 2 diabetes: a population-based study. Diabet Med. 2002;19:606–10.
Eurich DT, Simpson SH, Majumdar SR, Johnson JA. Secondary failure rates associated with metformin and sulfonylurea therapy for type 2 diabetes mellitus. Pharmacotherapy. 2005;25:810–6.
Cook MN, Girman CJ, Stein PP, Alexander CM. Initial monotherapy with either metformin or sulphonylureas often fails to achieve or maintain current glycaemic goals in patients with type 2 diabetes in UK primary care. Diabet Med. 2007;24:350–8.
Rustenbeck I. Desensitization of insulin secretion. Biochem Pharmacol. 2002;63:1921–35.
Maedler K, Carr RD, Bosco D, Zuellig RA, Berney T, Donath MY. Sulfonylurea induced beta-cell apoptosis in cultured human islets. J Clin Endocrinol Metab. 2005;90:501–6.
Takahashi A, Nagashima K, Hamasaki A, et al. Sulfonylurea and glinide reduce insulin content, functional expression of K(ATP) channels, and accelerate apoptotic beta-cell death in the chronic phase. Diabetes Res Clin Pract. 2007;77:343–50.
Kim JY, Lim DM, Park HS, et al. Exendin-4 protects against sulfonylurea-induced beta-cell apoptosis. J Pharmacol Sci. 2012;118:65–74.
Satoh J, Takahashi K, Takizawa Y, et al. Secondary sulfonylurea failure: comparison of period until insulin treatment between diabetic patients treated with gliclazide and glibenclamide. Diabetes Res Clin Pract. 2005;70:291–7.
Acknowledgments
The analysis and article processing charges were sponsored by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Whitehouse Station, NJ, USA. Dr. Qiu is the guarantor for this article, and takes responsibility for the integrity of the work as a whole.
Conflict of interest
Dr. Fu has received research grant support from Merck. Dr. Qiu, Dr. Davies, and Dr. Engel are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Whitehouse Station, NJ, USA, and may own stock or stock options in Merck.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Fu, A.Z., Qiu, Y., Davies, M.J. et al. Initial Sulfonylurea Use and Subsequent Insulin Therapy in Older Subjects with Type 2 Diabetes Mellitus. Diabetes Ther 3, 12 (2012). https://doi.org/10.1007/s13300-012-0012-9
Received:
Published:
DOI: https://doi.org/10.1007/s13300-012-0012-9