
Abstract
Purpose
Precise localization of the cervicothoracic vertebral levels is essential for accurate placement of epidural catheters. Previous studies have demonstrated that anesthesiologists are inaccurate when using surface anatomy to locate lumbar vertebral levels. Our study was designed to determine the agreement between anatomical landmarks and the ultrasound technique in identifying the T7-8 and C7-T1 intervertebral spaces.
Methods
Adult healthy volunteers were assessed for the identification of cervicothoracic intervertebral spaces, initially in the anatomic position (AP)—upright, back straight, arms at the sides, and palms forward and then in the epidural position (EP) routinely used for epidural placement—seated, back arched, neck flexed, and arms across the chest. The T7 and C7 spinous processes were identified by one investigator using the inferior tip of the scapula and the vertebra prominens, respectively, as landmarks. Ultrasound was then used by a second investigator to identify the intervertebral spaces corresponding to the previously marked levels.
Results
Fifty-five volunteers (23 males, 32 females) were recruited. The T7-8 intervertebral space determined by ultrasound coincided with the landmark findings in the AP and in the EP in 18% and 36% of the cases, respectively. The C7-T1 interspace identified by ultrasound corresponded with the surface landmarks in the AP and in the EP in 53% and 58% of the cases, respectively. In most cases, when the surface landmark and ultrasound findings of T7-8 did not agree, the surface landmark identified a lower interspace than ultrasound.
Conclusion
Identification of cervicothoracic intervertebral spaces by surface landmarks corresponded poorly with their identification using ultrasound. However, compared with the upright position, agreement in identifying the T7-8 interspace improved in the epidural position.
Résumé
Objectif
La localisation précise des niveaux vertébraux cervicothoraciques est cruciale pour positionner de façon précise les cathéters périduraux. Des études ont précédemment démontré que les anesthésiologistes sont peu précis lorsqu’ils se servent des repères anatomiques pour localiser les niveaux vertébraux lombaires. Notre étude a été conçue afin de déterminer la correspondance des résultats obtenus en se fondant sur des repères anatomiques ou une technique par échographie pour déterminer l’emplacement des espaces intervertébraux T7-8 et C7-T1.
Méthode
Des volontaires sains adultes ont été évalués afin de déterminer l’emplacement des espaces intervertébraux cervicothoraciques, d’abord en position anatomique (PA) – soit debout, le dos droit, les bras le long du corps et les paumes vers l’avant, puis en position péridurale (PP), communément utilisée pour l’installation des péridurales – soit assis, le dos cambré, le cou fléchi et les bras croisés devant la poitrine. Les apophyses épineuses T7 et C7 ont été identifiées par un chercheur qui s’est servi de la pointe inférieure de l’omoplate et de la septième vertèbre cervicale (vertèbre proéminente), respectivement, comme repères. Un deuxième chercheur s’est ensuite servi de l’échographie pour déterminer l’emplacement des espaces intervertébraux correspondant aux niveaux précédemment marqués.
Résultats
Cinquante-cinq volontaires (23 hommes, 32 femmes) ont été recrutés. L’espace intervertébral T7-8 déterminé par échographie correspondait à l’espace déterminé par repère anatomique en PA et en PP dans 18 % et 36 % des cas, respectivement. L’espace intervertébral C7-T1 tel que déterminé par échographie correspondait à celui déterminé par repère anatomique en PA et en PP dans 53 % et 58 % des cas, respectivement. Dans la plupart des cas, lorsque les repères anatomiques et les résultats par échographie ne correspondaient pas au niveau T7-8, le repère anatomique avait identifié un espace intervertébral plus bas que l’échographie.
Conclusion
La détermination de l’emplacement des espaces intervertébraux cervicothoraciques par des repères anatomiques correspond mal à leur localisation à l’aide de l’échographie. Toutefois, il existe une meilleure correspondance entre les deux techniques pour l’espace intervertébral T7-8 en position péridurale qu’en position anatomique.
Similar content being viewed by others


Thoracic epidural administration of local anesthetics provides excellent anesthesia and analgesia for thoracic and abdominal surgeries, improves postoperative outcome, and reduces postoperative pulmonary complications.1 Accurate identification of the vertebral level is essential for assuring optimal anesthesia and analgesia with minimal side effects. However, palpation of anatomical landmarks has been shown to be inaccurate at identifying lumbar spinous processes and intervertebral levels.2,3 For the cervicothoracic spine, two surface anatomical landmarks are frequently used: a) a line joining the inferior tip of the scapula, which corresponds to the spinous process of the seventh thoracic vertebra (T7); and b) the spinous process of vertebra prominens (C7).4 These surface landmarks have been used in clinical practice to indicate the level of sensory blockade which correlates with the segmental spinal nerve. Ultrasound has recently been introduced into anesthesia practice to facilitate the placement of lumbar neuraxial blocks,5-8 and it has been proven to increase the accuracy of identifying the intervertebral level9,10 as well as needle placement, even in difficult cases.11 The main objective of our study was to determine the agreement between the surface landmark method and the ultrasound technique in identifying the T7-8 and C7-T1 interspaces in healthy adults. The secondary objective was to evaluate the influence that changing the subjects’ posture would have on these findings. We hypothesized that the surface landmark method would not agree with the ultrasound technique in predicting the targeted cervicothoracic interspaces.
Methods
We followed the General Guidelines for Reporting Reliability and Agreement Studies (GRRAS) supported by The EQUATOR Network (Enhancing the QUAlity and Transparency Of health Research).12 This prospective observational study was approved by the Mount Sinai Hospital Research Ethics Board, and volunteer participants were enrolled after they provided written informed consent. Study participants were healthy adults aged 18-40 yr with a body mass index (BMI) < 30 kg·m−2. We excluded all participants with obvious or known spinal deformity (e.g., kyphosis, scoliosis) or previous spine trauma or surgery. One of the investigators performed the spinal assessment by locating the T7-8 and C7-T1 intervertebral levels using anatomical landmarks, while a second investigator subsequently performed the ultrasound scanning.
Surface landmark method
With subjects in the classical anatomic position (upright, back straight, arms at the sides, and palms forward), one investigator palpated the inferior angle of each scapula. The spinous process intersected by a horizontal line connecting the two scapular angles was identified as the T7 spinous process, and the first interspace below T7 was identified as the T7-8 thoracic interspace. This interspace level was marked on the subject’s skin by a line (A). Next, the C7 vertebra (vertebra prominens) was identified by the same investigator as the most prominent spinous process at the base of the neck, and the first interspace below C7 was identified as the C7-T1 interspace. This interspace level was marked on the subject’s skin by a second line (B). The palpatory identification procedure was repeated using the same anatomical landmarks with subjects in the epidural position (seated, back arched, neck flexed, and arms across the chest). Another pair of lines was marked on the subject’s skin at each level using the landmarks described above—one identifying the T7-8 interspace (A′) and the other identifying the C7-T1 interspace (B′). The investigator then measured the vertical distance between the two lines at each level and labelled them as interscapular distance (ISD) for the distance between A and A′ and intercervical distance (ICD) for the distance between B and B′ (with the subject remaining in the epidural position). We used the ISD and ICD to assess the degree of flexion at the thoracic and cervical levels, respectively, similar to Shober’s test in the lumbar spine.13
Ultrasound assessment technique
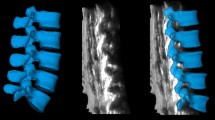
Following assessment using the surface landmark method, a second investigator with at least two years of experience in lumbar and thoracic ultrasound scanning used a portable ultrasound system equipped with a 2-5 MHz curved array probe (SonoSite M-TurboTM Canada Inc., Markham, ON, Canada) to identify the interspace represented by each of the four lines previously marked at the thoracic and cervical levels (A, A′, B, B′) as well as the position of the targeted interspace. The ultrasound probe was placed in a right paramedian plane 2 cm from the midline at the level of the sacrum, and the first key ultrasound landmark was then visualized on the screen as a continuous and horizontal hyperechoic line. The probe was then slid in a cephalad direction and tilted towards the midline. This allowed identification of alternate lamina and interspaces which were visualized as a hyperechoic “saw-tooth” pattern with the teeth of the saw representing the lamina interrupted by interspaces. In this way, the L5-S1 interspace and each successive intervertebral space were identified on the ultrasound screen in a systematic “counting-up” approach as the probe was moved in a cephalad direction.5,14,15 The ultrasound examination was performed with the subjects placed in the epidural position. In order to minimize the potential for identification error due to the presence of lumbosacral anomalies (sacralization of L5 or lumbarization of S1), we also included identification of the 12th rib and its articulation with the T12 vertebra as a second key ultrasound landmark of this counting-up approach.16 The spinal assessment was always performed in the same order, i.e., surface landmarks first and ultrasound second. The methodological considerations and typical sonoanatomy of a thoracic interspace in a right paramedian plane are depicted in Fig. 1.

Methodological considerations. (A) Subject in the anatomic position. (B) Subject in the epidural position. Lines were drawn on the skin at the level of T7-8 and C7-T1 interspaces. ISD = interscapular distance at the T7-8 level, and ICD = intercervical distance at the C7-T1 level. (C) Typical sonoanatomy of a thoracic interspace in a right-paramedian plane. Ultrasonographic structures identified: La = lamina; Lf/Dm = Ligamentum Flavum-Dura Mater complex; Vb = vertebral body
The primary outcome of the study was to determine the agreement between the surface landmark method and the ultrasound technique in identifying the T7-8 and C7-T1 interspaces in adult healthy volunteers. The secondary outcome was to establish whether such level of agreement would be influenced by positioning the subjects in the anatomic or the epidural posture.
Statistical analysis
Descriptive statistics, including the mean, standard deviation (SD), and range, were calculated for continuous data, and percentages were calculated for discrete data. In order to compare the surface landmark method and the ultrasound technique, we calculated the proportion of agreement between the two techniques in identifying the same vertebral level in both the anatomic and the epidural positions. We then compared the proportions of specific agreement for the two positions using the Fisher’s exact test. Means were compared using Student’s t test. A P value < 0.05 was considered statistically significant. All statistical analyses were carried out using STATA 9.2 for Macintosh (College Station, TX, USA).
For the sample size calculation, we considered the agreement results from two studies. In identifying thoracic interspaces, Holmaas et al.17 found an agreement of 26.7% between the clinical palpatory method and magnetic resonance imaging (MRI), while Teoh et al.18 found a 10% agreement between the scapular tip and T7 spinous process when using chest radiography to confirm the clinical palpatory method. For a two-sided type I error of 5% and a type II error of 20%, 45 subjects were needed to estimate the rate of agreement between the ultrasound and palpatory techniques within the range of the above mentioned results. Assuming a possible dropout rate of 20%, we planned to enrol 54 subjects.
Results
Fifty-five healthy adult volunteers were recruited for this study (23 males and 32 females) from August 1, 2009 to September 31, 2010. The demographic variables, including age, height, weight and BMI, are presented in Table 1.
There was poor agreement between the landmark and the ultrasound techniques in identifying the T7-8 interspace; however, agreement improved when the subjects were assessed in the epidural rather than in the anatomic position (36% vs 18%, respectively; Fisher’s exact test, P = 0.035). On the other hand, agreement in identifying the C7-T1 interspace was better than that for the T7-8 interspace, and it was unaffected by position (53% vs 58%, the anatomic or epidural position, respectively; Fisher’s exact test, P = 0.572) (Table 2). When the surface landmark method did not agree with the ultrasound identification of T7-8, it was more likely to correspond with a lower rather than a higher interspace in relation to the ultrasound assessment (83% vs 18%, respectively; Fisher’s exact test, P < 0.0001). For the C7-T1 interspace, the disagreement was as likely to be in the caudal as in the cephalad direction (45% vs 55%; Fisher’s exact test, P = 0.547) (Fig. 2). The skin markings obtained were always lower in the epidural position than in the anatomic position, thus, the distance between the skin markings was oriented caudally when changing from the anatomic to the epidural position. This distance was greater at the T7-8 interspace 1.6 (1.1) cm than at the C7-T1 interspace 0.9 (0.8) cm (Student’s t test, P = 0.0003).

Level determined by ultrasound of (A) the T7-T8 level identified by palpation as corresponding to the tip of the scapula and (B) the C7-T1 level identified by palpation as the vertebra prominens. Agreement is depicted by black circles, disagreement by grey circles. The circle surface area is proportional to the number of subjects
Discussion
This study shows that surface landmarks traditionally described to identify cervicothoracic interspaces do not correspond with those identified by ultrasound. The agreement of the surface landmark method in identifying the C7-T1 interspace is similar regardless of subject position; however, at the T7-8 interspace, agreement is improved in the epidural position.
Previous research using MRI found that only 26.7% of the thoracic interspaces were identified correctly by palpation (using vertebra prominens and the iliac crest as landmarks), and in 76.4% of cases, the MRI indicated a level that was more in the cephalad direction than that of palpation.17 Similarly, a study to compare palpation of surface landmarks with chest radiography in patients in the anatomic position found that both the vertebra prominens and the scapular tip were inaccurate landmarks for identifying the T7 spinous process (29% vs 10% accuracy, respectively).18 In our study, the agreement was better in the epidural position than in the anatomic position when using the scapula as a landmark. In our view, these findings may stem from the fact that the spine is more flexible at the level of the T7-8 interspace than at the C7-T1 interspace (ISD > ICD). Moreover, switching from the anatomic position to the epidural position also translates into an upwards and outwards rotation of the scapula when crossing the arms on the chest, which may cause the tips of the scapula to correspond with a higher interspace. For the C7-T1 level, the epidural position adds only a small degree of flexion to the cervical spine, making the C7 spinous process a more stable and reliable anatomic landmark than the scapular tip. Nevertheless, studies have shown that vertebra prominens corresponds to C7 in 58.8% of males and 78.7% of females. It can also correspond to C6 or T1 19 which might also explain the disagreement when using vertebra prominens as a landmark. These observations have practical implications for physicians performing epidural procedures, as they show the relative importance of positioning the patients in the epidural posture while selecting the interspace using a surface landmark method. In addition, they suggest that vertebra prominens is a more reliable marker than the tip of the scapula if surface landmarks are to be used to estimate an interspace. Recent review data suggest that ultrasound is useful not only to increase the accuracy of identification of vertebral interspaces but also to facilitate the placement of the epidural catheter.15 A preprocedure scan could help obtain the information required to calculate the appropriate needle insertion site and trajectory.
Studies have also demonstrated the inaccuracy of the surface landmark method for the lumbar vertebral region. Furness et al. showed that the correct intervertebral level of non-pregnant subjects was identified by palpation in only 30% of cases when using lumbar radiograph as the gold standard.9 In another study, the accuracy of detecting a particular lumbar interspace was 29% when using the intercristal line as a landmark.2 Moreover, for the lumbar vertebral region, it has been shown that clinicians are more likely to select interspaces that are one or two spaces higher than the correct space.2,20 When trying to identify the T7-8 interspace in our study, the surface landmark method was more likely to indicate a more caudal interspace than ultrasonography. When using chest radiography as a gold standard for the thoracic spine, the inaccuracy has been to identify lower interspaces.18
One limitation of this study is that we compared the surface landmark method with the ultrasound technique, which is not a “gold standard” imaging technique, such as radiography, computed tomography, or MRI, for the examination of the vertebral column. Despite the higher imaging quality offered by these standard techniques, they are not suitable for a rapid prepuncture assessment of the spine, mainly because they are costly and time-consuming, the equipment is stationary, and they can be used only by highly trained personnel. On the contrary, bedside ultrasound is widely available, mobile, faster, and easier to handle, making it a more appropriate tool for rapid evaluation of the vertebral column. When compared with these standard techniques, ultrasound has been reported to have an accuracy of 68-76% depending on the method used for comparison.9,10,16 However, a recent study showed an increase (from 68% to at least 90%) in the accuracy of ultrasound for identification of lumbar interspinous spaces after appropriate training when computed tomography was used as the gold standard for confirmation.16 Another limitation of this study is the potential source of bias introduced by marking lines on the skin, which may have biased the second investigator who was not blinded. However, in our study design, this was deemed necessary in order to compare the exact interspace identified by palpation with the one identified by ultrasound.
Our study was conducted on healthy young volunteers who are not representative of the majority of patients in clinical practice. However, the aim of this study was to show as proof of principle and with minimal confounders that, in a majority of instances, the surface landmark method differed from the ultrasound technique when identifying cervicothoracic interspaces, even in subjects with normal spinal anatomy.
In counting up all interspaces from the sacrum, the ultrasound exam was more comprehensive than the landmark exam. This process was performed to maximize the accuracy of the ultrasound technique in identifying the spinal interspaces. In clinical practice, scanning the interspaces can be performed by relying on the hyperechoic reference of the sacrum or by identifying the 12th rib and its articulation with the T12 vertebra.15,16
In conclusion, the identification of cervicothoracic interspaces by palpation of surface landmarks does not correspond with their identification using ultrasound. Compared with the anatomic position, use of the surface landmark method in the epidural position improves agreement with the ultrasound technique for identification of T7-8. Additionally, there is a tendency with palpation to predict a lower thoracic interspace. We recommend placing patients in the epidural position for the conventional surface landmark method, and whenever possible, we suggest using the ultrasound technique to evaluate the level for epidural procedure. Although our results show consistency with previous findings, a study comparing ultrasonography with a gold standard imaging technique is necessary to confirm the usefulness of ultrasonography for identification of cervicothoracic intervertebral spaces. Also, future studies are needed to investigate the role of ultrasound in facilitating the placement of thoracic epidurals and to evaluate patient satisfaction.
References
Groeben H. Epidural anesthesia and pulmonary function. J Anesth 2006; 20: 290-9.
Broadbent CR, Maxwell WB, Ferrie R, Wilson DJ, Gawne-Cain M, Russell R. Ability of anaesthetists to identify a marked lumbar interspace. Anaesthesia 2000; 55: 1122-6.
Van Gessel EF, Forster A, Gamulin Z. Continuous spinal anesthesia: where do spinal catheters go? Anesth Analg 1993; 76: 1004-7.
Gray H. Anatomy of the Human Body, 20th ed. Philadelphia: Lea & Febiger; 1918; Bartleby.com, 2000. Available from URL: http://www.bartleby.com/107/ (accessed November 2010).
Carvalho JC. Ultrasound-facilitated epidurals and spinals in obstetrics. Anesthesiol Clin 2008; 26: 145-58.
Chin KJ, Perlas A, Singh M, et al. An ultrasound-assisted approach facilitates spinal anesthesia for total joint arthroplasty. Can J Anesth 2009; 56: 643-50.
Grau T, Leipold RW, Conradi R, Martin E, Motsch J. Ultrasound imaging facilitates localization of the epidural space during combined spinal and epidural anesthesia. Reg Anesth Pain Med 2001; 26: 64-7.
Arzola C, Davies S, Rofaeel A, Carvalho JC. Ultrasound using the transverse approach to the lumbar spine provides reliable landmarks for labor epidurals. Anesth Analg 2007; 104: 1188-92.
Furness G, Reilly MP, Kuchi S. An evaluation of ultrasound imaging for identification of lumbar intervertebral level. Anaesthesia 2002; 57: 277-80.
Watson MJ, Evans S, Thorp JM. Could ultrasonography be used by an anaesthetist to identify a specified lumbar interspace before spinal anaesthesia? Br J Anaesth 2003; 90: 509-11.
Balki M, Lee Y, Halpern S, Carvalho JC. Ultrasound imaging of the lumbar spine in the transverse plane: the correlation between estimated and actual depth to the epidural space in obese parturients. Anesth Analg 2009; 108: 1876-81.
Kottner J, Audige L, Brorson S, et al. Guidelines for reporting reliability and agreement studies (GRRAS) were proposed. J Clin Epidemiol 2011; 64: 96-106.
Bickley LS. Bates’ Guide to Physical Examination and History Taking. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2007. p. 534-6.
Borges BC, Wieczorek P, Balki M, Carvalho JC. Sonoanatomy of the lumbar spine of pregnant women at term. Reg Anesth Pain Med 2009; 34: 581-5.
Chin KJ, Karmakar MK, Peng P. Ultrasonography of the adult thoracic and lumbar spine for central neuraxial blockade. Anesthesiology 2011; 114: 1459-85.
Halpern SH, Banerjee A, Stocche R, Glanc P. The use of ultrasound for lumbar spinous process identification: a pilot study. Can J Anesth 2010; 57: 817-22.
Holmaas G, Frederiksen D, Ulvik A, Vingsnes SO, Ostgaard G, Nordli H. Identification of thoracic intervertebral spaces by means of surface anatomy: a magnetic resonance imaging study. Acta Anaesthesiol Scand 2006; 50: 368-73.
Teoh DA, Santosham KL, Lydell CC, Smith DF, Beriault MT. Surface anatomy as a guide to vertebral level for thoracic epidural placement. Anesth Analg 2009; 108: 1705-7.
Stonelake PS, Burwell RG, Webb JK. Variation in vertebral levels of the vertebra prominens and sacral dimples in subjects with scoliosis. J Anat 1988; 159: 165-72.
Whitty R, Moore M, Macarthur A. Identification of the lumbar interspinous spaces: palpation versus ultrasound. Anesth Analg 2008; 106: 538-40.
Acknowledgement
The authors thank Mrs. Kristi Downey for technical assistance during ultrasound scanning.
Financial support
Departmental funds.
Conflict of interests
None declared.
Author information
Authors and Affiliations
Corresponding author
Additional information
Cristian Arzola and Sinziana Avramescu are co-first authors.
Rights and permissions
About this article
Cite this article
Arzola, C., Avramescu, S., Tharmaratnam, U. et al. Identification of cervicothoracic intervertebral spaces by surface landmarks and ultrasound. Can J Anesth/J Can Anesth 58, 1069–1074 (2011). https://doi.org/10.1007/s12630-011-9587-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-011-9587-2