
Abstract
Objectives
Due to the increased morbidity, mortality, and cost of community-acquired pneumonia (CAP) in older people, strategies directed at improving disease evaluation and prevention are imperative. We independently compared the 30-day in-hospital mortality prediction ability of a frailty index based on laboratory data (FI-Lab) with that of the CURB-65 and the Pneumonia Severity Index (PSI) and then proposed combining them to further improve prediction efficiency.
Design
Retrospective cohort study.
Setting and Participants
Patients aged ≥ 65 years (n = 2039) with CAP who were admitted to Jiangsu Provincial People’s Hospital of Nanjing Medical University and Jiangsu Provincial Hospital of Chinese Medicine from January 2019 to June 2022.
Measures
The 29-item FI-Lab, PSI and, CURB-65 were administered at admission. We defined frailty by the cut-off value of the FI-Lab score (> 0.43). Multivariable logistic regression analysis, together with the calculation of the area under the receiver operating characteristic curve (ROC-AUC), was conducted to identify stratified risks and relationships between the three indices and 30-day mortality. Participants were divided into the following three groups based on age: 65–74 years, 75–84 years, and ≥ 85 years. Hazard ratios (HRs) and 95% confidence intervals (CIs) for mortality due to frailty were calculated.
Results
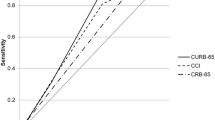
A total of 495 participants ranging from 65 to 100 years of age were ultimately included and divided into age groups (65–74 years, n = 190, 38.4%; 75–84 years, n = 183, 37.0%; ≥ 85 years, n = 122, 24.6%). A total of 142 (28.7%) of the 495 patients were defined as having frailty. All three scores tested in this study were significantly associated with 30-day mortality in the total sample. The ORs were as follows: 1.06 (95% CI: 1.03–1.09, P < 0.001) and 2.33 (95% CI: 1.26–4.31, P = 0.007) for the FI-Lab when the score was treated as a continuous and categorical variable, respectively; 1.04 (95% CI: 1.02–1.05, P < 0.001) for the PSI; and 3.70 (95% CI: 2.48–5.50, P < 0.001) for the CURB-65. In the total sample, the ROC-AUCs were 0.783 (95% CI: 0.744–0.819) for the FI-Lab, 0.812 (95% CI: 0.775–0.845) for the PSI, and 0.799 (95% CI: 0.761–0.834) for the CURB-65 (P < 0.001). The ROC-AUC slightly improved when the FI-Lab was added to the PSI (AUC 0.850, 95% CI: 0.809–0.892, P = 0.031) and to the CURB-65 (AUC 0.839, 95% CI: 0.794–0.885, P = 0.002). Older patients with frailty showed a higher risk of in-hospital mortality, with an HR of 2.25 (95% CI: 1.14–3.58, P < 0.001).
Conclusion and Implications
The FI-Lab seems to generate simple and readily available data, suggesting that it could be a useful complement to the CURB-65 and the PSI as effective predictors of 30-day mortality due to CAP in older populations.



Similar content being viewed by others


References
Brown JD, Harnett J, Chambers R, Sato R. The relative burden of community-acquired pneumonia hospitalizations in older adults: a retrospective observational study in the United States. BMC Geriatr. 2018;18(1):92. doi:https://doi.org/10.1186/s12877-018-0787-2
Chen J-H, Chang S-S, Liu JJ, Chan R-C, Wu J-Y, Wang W-C, et al. Comparison of clinical characteristics and performance of pneumonia severity score and CURB-65 among younger adults, elderly and very old subjects. Thorax. 2010;65(11):971–7. doi:https://doi.org/10.1136/thx.2009.129627
Tokioka F, Okamoto H, Yamazaki A, Itou A, Ishida T. The prognostic performance of qSOFA for community-acquired pneumonia. J Intensive Care. 2018;6:46. doi:https://doi.org/10.1186/s40560-018-0307-7
Cillóniz C, Dominedò C, Pericàs JM, Rodriguez-Hurtado D, Torres A. Community-acquired pneumonia in critically ill very old patients: a growing problem. Eur Respir Rev. 2020;29(155). doi:https://doi.org/10.1183/16000617.0126-2019
Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–75. doi:https://doi.org/10.1016/S0140-6736(19)31786-6
Fan J, Yu C, Guo Y, Bian Z, Sun Z, Yang L, et al. Frailty index and all-cause and cause-specific mortality in Chinese adults: a prospective cohort study. Lancet Public Health. 2020;5(12):e650–e60. doi:https://doi.org/10.1016/s2468-2667(20)30113-4
Vetrano DL, Triolo F, Maggi S, Malley R, Jackson TA, Poscia A, et al. Fostering healthy aging: The interdependency of infections, immunity and frailty. Ageing Res Rev. 2021;69:101351. doi:https://doi.org/10.1016/j.arr.2021.101351
Qu JM, Cao B. [Guidelines for the diagnosis and treatment of adult community acquired pneumonia in China (2016 Edition)]. Zhonghua Jie He He Hu Xi Za Zhi. 2016;39(4):241–2. doi:https://doi.org/10.3760/cma.j.issn.1001-0939.2016.04.001
Chen Y-Z, Huang S-T, Wen Y-W, Chen L-K, Hsiao F-Y. Combined Effects of Frailty and Polypharmacy on Health Outcomes in Older Adults: Frailty Outweighs Polypharmacy. Journal of the American Medical Directors Association. 2021;22(3). doi:https://doi.org/10.1016/j.jamda.2020.07.019
Howlett SE, Rockwood MRH, Mitnitski A, Rockwood K. Standard laboratory tests to identify older adults at increased risk of death. BMC Medicine. 2014;12:171. doi:https://doi.org/10.1186/s12916-014-0171-9
Rockwood K, McMillan M, Mitnitski A, Howlett SE. A Frailty Index Based on Common Laboratory Tests in Comparison With a Clinical Frailty Index for Older Adults in Long-Term Care Facilities. Journal of the American Medical Directors Association. 2015;16(10):842–7. doi:https://doi.org/10.1016/j.jamda.2015.03.027
Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. The New England Journal of Medicine. 1997;336(4):243–50.
Lim WS, van der Eerden MM, Laing R, Boersma WG, Karalus N, Town GI, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377–82.
Erdogan A, Can FE, Gönüllü H. Evaluation of the prognostic role of NLR, LMR, PLR, and LCR ratio in COVID-19 patients. J Med Virol. 2021;93(9):5555–9. doi:https://doi.org/10.1002/jmv.27097
Zan Y, Song W, Wang Y, Shao J, Wang Z, Zhao W, et al. Nomogram for predicting in-hospital mortality of nonagenarians with community-acquired pneumonia. Geriatr Gerontol Int. 2022;22(8):635–41. doi:https://doi.org/10.1111/ggi.14430
Lasko TA, Bhagwat JG, Zou KH, Ohno-Machado L. The use of receiver operating characteristic curves in biomedical informatics. J Biomed Inform. 2005;38(5):404–15.
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44(3):837–45.
Calle A, Márquez MA, Arellano M, Pérez LM, Pi-Figueras M, Miralles R. Geriatric assessment and prognostic factors of mortality in very elderly patients with community-acquired pneumonia. Arch Bronconeumol. 2014;50(10):429–34. doi:https://doi.org/10.1016/j.arbres.2014.01.012
Baek MS, Park S, Choi J-H, Kim C-H, Hyun IG. Mortality and Prognostic Prediction in Very Elderly Patients With Severe Pneumonia. J Intensive Care Med. 2020;35(12):1405–10. doi:https://doi.org/10.1177/0885066619826045
Ilg A, Moskowitz A, Konanki V, Patel PV, Chase M, Grossestreuer AV, et al. Performance of the CURB-65 Score in Predicting Critical Care Interventions in Patients Admitted With Community-Acquired Pneumonia. Ann Emerg Med. 2019;74(1):60–8. doi:https://doi.org/10.1016/j.annemergmed.2018.06.017
van Vught LA, Endeman H, Meijvis SC, Zwinderman AH, Scicluna BP, Biesma DH, et al. The effect of age on the systemic inflammatory response in patients with community-acquired pneumonia. Clin Microbiol Infect. 2014;20(11):1183–8. doi:https://doi.org/10.1111/1469-0691.12717
Yang M, Zhuo Y, Hu X, Xie L. Predictive validity of two frailty tools for mortality in Chinese nursing home residents: frailty index based on common laboratory tests (FI-Lab) versus FRAIL-NH. Aging Clin Exp Res. 2018;30(12):1445–52. doi:https://doi.org/10.1007/s40520-018-1041-7
Gu JJ, Liu Q, Zheng LJ. A Frailty Assessment Tool to Predict In-Hospital Mortality in Patients with Acute Exacerbations of Chronic Obstructive Pulmonary Disease. Int J Chron Obstruct Pulmon Dis. 2021;16:1093–100. doi:https://doi.org/10.2147/COPD.S300980
Govoni S, Fagiani F, Lanni C, Allegri N. The Frailty Puzzle: Searching for Immortality or for Knowledge Survival? Front Cell Neurosci. 2022;16:838447. doi:https://doi.org/10.3389/fncel.2022.838447
Lang P-O, Michel J-P, Zekry D. Frailty syndrome: a transitional state in a dynamic process. Gerontology. 2009;55(5):539–49. doi:https://doi.org/10.1159/000211949
Becerra-Muñoz VM, Núñez-Gil IJ, Eid CM, García Aguado M, Romero R, Huang J, et al. Clinical profile and predictors of in-hospital mortality among older patients hospitalised for COVID-19. Age Ageing. 2021;50(2):326–34. doi:https://doi.org/10.1093/ageing/afaa258
Corrales-Medina VF, Alvarez KN, Weissfeld LA, Angus DC, Chirinos JA, Chang C-CH, et al. Association between hospitalization for pneumonia and subsequent risk of cardiovascular disease. JAMA. 2015;313(3):264–74. doi:https://doi.org/10.1001/jama.2014.18229
Ysea-Hill O, Gomez CJ, Mansour N, Wahab K, Hoang M, Labrada M, et al. The association of a frailty index from laboratory tests and vital signs with clinical outcomes in hospitalized older adults. J Am Geriatr Soc. 2022;70(11):3163–75. doi:https://doi.org/10.1111/jgs.17977
Wang C, Fang X, Tang Z, Hua Y, Zhang Z, Gu X, et al. A frailty index based on routine laboratory data predicts increased risk of mortality in Chinese community-dwelling adults aged over 55 years: a five-year prospective study. BMC Geriatr. 2022;22(1):679. doi:https://doi.org/10.1186/s12877-022-03374-z
Abel GA, Klepin HD. Frailty and the management of hematologic malignancies. Blood. 2018;131(5):515–24. doi:https://doi.org/10.1182/blood-2017-09-746420
Cespedes Feliciano EM, Hohensee C, Rosko AE, Anderson GL, Paskett ED, Zaslavsky O, et al. Association of Prediagnostic Frailty, Change in Frailty Status, and Mortality After Cancer Diagnosis in the Women’s Health Initiative. JAMA Netw Open. 2020;3(9):e2016747. doi:https://doi.org/10.1001/jamanetworkopen.2020.16747
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The present study was carried out with the approval of the institutional review board (application number: 2021-SRFA-446). Informed consent was waived due to the retrospective design of the study.
Additional information
Conflict of interest
All the authors declare no conflict of interest.
Electronic Supplementary Material
Rights and permissions
About this article

Cite this article
Zan, Y.M., Zheng, T.P., Wang, Y. et al. Combining a Frailty Index Based on Laboratory Data and Pneumonia Severity Assessments to Predict In-Hospital Outcomes in Older Adults with Community-Acquired Pneumonia. J Nutr Health Aging 27, 270–276 (2023). https://doi.org/10.1007/s12603-023-1905-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12603-023-1905-1