
Abstract
Background
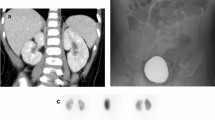
99mTc-dimercaptosuccinic acid (DMSA) scan is the golden standard for the diagnosis of acute pyelonephritis and renal scaring. We investigated the use of acute phase DMSA scan in infants presented promptly to the hospital because of the first episode of their febrile urinary tract infection (UTI).
Methods
Ninety-eight infants with microbiologically confirmed first episode of febrile UTI were studied. DMSA scans were carried out within 7 days in these infants after admission. Infants with an abnormal acute DMSA scan underwent a second DMSA scan 6–12 months later.
Results
Overall, acute DMSA scan was abnormal in 16 (16.3%) of the 98 patients. There were no differences in sex, age, fever over 38.5°C, blood inflammation indices, or evidence of vesicoureteral reflux (VUR) between patients with normal and abnormal acute DMSA scan (P>0.05). However, infants with grade III to V VUR as well as those with delayed treatment presented significantly increased renal involvement by acute DMSA scan (P<0.05). The sensitivity and specificity of abnormal acute DMSA scan to predict grade III to V VUR were 50% and 88% respectively. Its positive and negative likelihood ratios were 4.16 and 0.57, respectively. Of 16 children with abnormal initial DMSA scan results, 14 underwent a second DMSA scan. Follow-up DMSA scans were normal in 12 of the 14 children.
Conclusions
Parenchymal damage found in a minority of infants with febrile UTI presented promptly to the hospital. Acute phase DMSA scan should be carried out only in selected patients. An abnormal acute DMSA scan is a moderate predictor for dilated VUR and its ability to exclude VUR is restricted.
Similar content being viewed by others


References
Wald E. Urinary tract infections in infants and children: a comprehensive overview. Curr Opin Pediatr 2004;16:85–88.
Hellerstein S. Long-term consequences of urinary tract infections. Curr Opin Pediatr 2000;12:125–128.
Coulthard MG, Verber I, Jani JC, Lawson GR, Stuart CA, Sharma V, et al. Can prompt treatment of childhood UTI prevent kidney scarring? Pediatr Nephrol 2009;24:2059–2063.
Aktaş GE, Inanir S, Turoğlu HT. Renal cortical involvement in children with fi rst UTI: does it differ in the presence of primary VUR? Ann Nucl Med 2008;22:877–881.
Zaffanello M, Cataldi L, Brugnara M, Franchini M, Bruno C, Fanos V. Hidden high-grade vesicoureteral reflux is the main risk factor for chronic renal damage in children under the age of two years with fi rst urinary tract infection. Scand J Urol Nephrol 2009;43:494–500.
Rushton HG. The evaluation of acute pyelonephritis and renal scarring with technetium 99m-dimercaptosuccinic acid renal scintigraphy: evolving concepts and future directions. Pediatr Nephrol 1997;11:108–120.
Camacho V, Estorch M, Fraga G, Mena E, Fuertes J, Hernández MA, et al. DMSA study performed during febrile urinary tract infection: a predictor of patient outcome? Eur J Nucl Med Mol Imaging 2004;31:862–866.
Garin EH, Olavarria F, Araya C, Broussain M, Barrera C, Young L. Diagnostic signifi cance of clinical and laboratory fi ndings to localize site of urinary infection. Pediatr Nephrol 2007;22:1002–1006.
Hardy RD, Austin JC. DMSA renal scans and the top-down approach to urinary tract infection. Pediatr Infect Dis J 2008;27:476–477.
Piepsz A, Hahn K, Roca I, Ciofetta G, Toth G, Gordon I, et al. A radiopharmaceuticals schedule for imaging in paediatrics. Paediatric Task Group European Association Nuclear Medicine. Eur J Nucl Med 1990;17:127–129.
Bauer R, Kogan BA. New developments in the diagnosis and management of pediatric UTIs. Urol Clin North Am 2008;35:47–58; vi.
Jodal V. The natural history of bacteriuria in childhood. Infect Dis Clin North Am 1987;1:713–729.
Committee on Quality Improvement. Subcommittee on Urinary Tract Infection Practice parameter: the diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. American Academy of Pediatrics. Pediatrics 1999;103:843–852.
Rushton HG, Majd M. Dimercaptosuccinic acid renal scintigraphy for the evaluation of pyelonephritis and scarring: a review of experimental and clinical studies. J Urol 1992;148(5 Pt 2):1726–1732.
Jakobsson B, Soderlundh S, Berg U. Diagnostic signifi cance of 99mTc-dimercaptosuccinic acid (DMSA) scintigraphy in urinary tract infection. Arch Dis Child 1992;67:1338–1342.
Benador D, Benador N, Slosman DO, Nusslé D, Mermillod B, Girardin E. Cortical scintigraphy in the evaluation of renal parenchymal changes in children with pyelonephritis. J Pediatr 1994;124:17–20.
Jakobsson B, Berg U, Svensson L. Renal scarring after acute pyelonephritis. Arch Dis Child 1994;70:111–115.
Stokland E, Hellström M, Jacobsson B, Jodal U, Lundgren P, Sixt R. Early 99mTc dimercaptosuccinic acid (DMSA) scintigraphy in symptomatic first-time urinary tract infection. Acta Paediatr 1996;85:430–436.
Linné T, Fituri O, Escobar-Billing R, Karlsson A, Wikstad I, Aperia A, et al. Functional parameters and 99mtechnetium-dimercaptosuccinic acid scan in acute pyelonephritis. Pediatr Nephrol 1994;8:694–699.
Smellie JM, Ransley PG, Normand IC, Prescod N, Edwards D. Development of new renal scars: a collaborative study. BMJ 1985;290:1957–1960.
Jodal U, Winberg J. Management of children with unobstructed urinary tract infection. Pediatr Nephrol 1987;11:647–656.
Development of renal scars in children: missed opportunities in management. South Bedfordshire Practitioners’ Group. BMJ 1990;301:1082–1084.
Fernández-Menéndez JM, Málaga S, Matesanz JL, Solís G, Alonso S, Pérez Méndez C. Risk factors in the development of early technetium 99m-dimercaptosuccinic acid renal scintigraphy lesions during first urinary tract infection in children. Acta Paediatr 2003;92:21–26.
Hansson S, Dhamey M, Sigström O, Sixt R, Stokland E, Wennerström M, et al. Dimercapto-succinic acid renal scintigraphy instead of voiding cystogrophy for infants with urinary tract infection. J Urol 2004;172:1071–1074.
Preda I, Jodal U, Sixt R, Hansson S. Normal Dimercaptosuccinic acid scintigraphy makes cysteurethrogrophy unnecessary after urinary tract infection. J Pediatr 2007;151:581–584.
Tseng MH, Lin WJ, Lo WT, Wang SR, Chu ML, Wang CC. Does a normal DMSA obviate the performance of voiding cystourethrography in evaluation of young children after their fi rst urinary tract infection? J Pediatr 2007;150:96–99.
Fouzas S, Krikelli E, Vassilakos P, Gkentzi D, Papanastasiou DA, Salakos C. DMSA scan for revealing vesicoureteral reflux in young children with urinary tract infection. Pediatrics 2010;126:e513–519.
Hoberman A, Charron M, Hickey RW, Baskin M, Kearney DH, Wald ER. Imaging studies after a first febrile urinary tract infection in young children. N Engl J Med 2003;16;195–202.
Rossleigh MA. Scintigraphic imaging in renal infections. Q J Nucl Med Mol Imaging 2009;53:72–77.
Skoog SJ, Peters CA, Arant BS Jr, Copp HL, Elder JS, Hudson RG, et al. Pediatric Vesicoureteral Reflux Guidelines Panel Summary Report: Clinical Practice Guidelines for Screening Siblings of Children With Vesicoureteral Reflux and Neonates/Infants With Prenatal Hydronephrosis. J Urol 2010;184:1145–1151.
Peters C, Rushton HG. Vesicoureteral reflux associated renal damage: congenital reflux nephropathy and acquired renal scarring. J Urol 2010;184:265–273.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Printza, N., Farmaki, E., Piretzi, K. et al. Acute phase 99mTc-dimercaptosuccinic acid scan in infants with first episode of febrile urinary tract infection. World J Pediatr 8, 52–56 (2012). https://doi.org/10.1007/s12519-012-0335-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12519-012-0335-7