
Abstract
A large body of research demonstrated that individuals with attention deficit hyperactivity disorder (ADHD) suffer from various neuropsychological deficits. In contrast, less is known and only divergent evidence exists on perceptual functions of individuals with ADHD. This is problematic as neuropsychological and perceptual functions are closely interrelated and are often difficult to disentangle in behavioral assessments. This study presents the conduct and results of a systematic literature review on perceptual functions in children and adults with ADHD. This review considers studies using psychophysical methods (objective measurements) and self- and informant reports (subjective measurements). Results indicate that individuals with ADHD have altered perceptual functions in various domains as compared to typically developing individuals. Increased perceptual functions in individuals with ADHD were found with regard to olfactory detection thresholds, whereas reduced perceptual functions were evident for aspects of visual and speech perception. Moreover, individuals with ADHD were found to experience discomfort to sensory stimuli at a lower level than typically developing individuals. Alterations of perceptual functions in individuals with ADHD were shown to be moderated by various factors, such as pharmacological treatment, cognitive functions, and symptom severity. We conclude by giving implications for daily life functioning and clinical practice.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a childhood-onset neurodevelopmental disorder affecting approximately 5% of children worldwide (Polanczyk et al. 2007; American Psychiatric Association 2013). The majority of children with ADHD continue to show symptoms in adolescence and adulthood, frequently struggling in various domains of life (Wasserstein 2005). The diagnosis ADHD is defined based on behavioral criteria, comprising symptoms of inattention, hyperactivity, and impulsivity (American Psychiatric Association 2013). To support the diagnostic process, a clinical evaluation of ADHD often involves a neuropsychological assessment in order to objectify and characterize the individual level of cognitive functioning (Goldstein and Jansen 2008). Research indicates that neuropsychological functions most commonly affected in ADHD comprise aspects of attention and executive functions, including selective attention, divided attention sustained attention, working memory, and response inhibition (Fuermaier et al. 2015; Thome et al. 2012; Tucha et al. 2008; Lange et al. 2014). Even though standardized neuropsychological assessment can be considerably helpful in the clinical evaluation of individuals with ADHD, it must be stressed that not all patients with ADHD exhibit neuropsychological difficulties and that the profile and intensity of neuropsychological deficits vary greatly among those affected.
Despite being one of the most extensively studied psychiatric disorders, the pathophysiology underlying ADHD symptoms remains only poorly understood (Albrecht et al. 2015; Sharma and Couture 2014; Thapar et al. 2013). A vast amount of research demonstrated that ADHD has strong biological underpinnings, including abnormalities in neurotransmitter systems in the brain. Research has especially tried to link alterations in the dopaminergic neurotransmitter system to neuropsychological deficits associated with ADHD. For example, it has been suggested that reduced dopaminergic inputs to the prefrontal cortex in ADHD may account for deficits in working memory and attention (Arnsten and Li 2005). Moreover, associations between sustained attention and variants of a dopamine receptor gene have been observed in ADHD (Bellgrove et al. 2005). However, it is well known that an intact dopaminergic neurotransmitter system is not only important for higher cognitive functions, but also for aspects of human perception, such as olfaction (Hsia et al. 1999; Cave and Baker 2009), audition (Majic et al. 2011; Kashino and Kondo 2012; Li et al. 2013), or vision (Müller and Huston 2007). The relevance of dopamine for human perception on the one hand, and the dysfunctional dopaminergic system in ADHD on the other hand, stimulates the assumption of altered perceptual functions in individuals with ADHD. Conclusive findings on altered perceptual functions in individuals with ADHD compared to typically developing individuals, however, could not be derived from research so far.
Associations between perceptional functions and alterations in the dopaminergic system are well described in several psychiatric and neurological conditions. For instance, it is well established that patients with schizophrenia, Parkinson’s disease, and Alzheimer’s disease often suffer from olfactory impairments, possibly, among others, due to dysregulation of the dopaminergic system (Moberg et al. 1997, 2014; Doty 2012). Moreover, disturbances in color vision are found in various medical conditions involving altered dopaminergic synaptic transmission, such as Tourette syndrome (Melun et al. 2001), Huntington’s disease (Büttner et al. 1994), Parkinson’s disease (Pieri et al. 2000), and in cocaine-dependent patients (Roy et al. 2003). Furthermore, it has been reported that context-independent dopamine release in patients with psychotic disorders is often accompanied by experiencing sharpened senses (Kapur et al. 2005). Thus, literature suggests clear associations between abnormalities in perceptual functions and the dopaminergic system in several psychiatric and neurological conditions. Given these findings, it appears plausible that also individuals with ADHD may experience alterations in perceptual functions as compared to typically developing individuals.
A fine-grained investigation of perceptual functions in ADHD has high clinical relevance, since it was shown that perceptual abilities may affect cognitive functions and psychosocial development (Dunn 2001). For example, reduced participation and enjoyment of daily life activities have been observed in children with sensory processing problems (Bar-Shalita et al. 2008). Furthermore, individuals with auditory processing disorders often experience language, reading, and spelling problems (Tallal et al. 1993; Bamiou 2001). Thus, neurocognitive functions are highly interrelated and allied with perception (Lindenberger and Baltes 1997; Tacca 2011; Cahen and Tacca 2013). Since both—clinical practice and research on ADHD—often include behavioral neuropsychological assessments, it is of importance to disentangle perception and higher-level cognitive functions as much as possible. Hence, understanding perceptual functioning in ADHD may contribute to a clearer conception of the pathophysiology of ADHD and is, thus, of theoretical and clinical importance.
The goal of the present systematic literature review is, therefore, to identify and evaluate studies which investigate perceptional functioning in children and adults with ADHD in comparison with normal controls (NCs). For this purpose, we included both studies using psychophysical measurements (objective assessments) as well as self- and informant reports (subjective assessments) on perceptual functioning in ADHD. Psychophysics studies the relationship between physical properties of a stimulus and the perception of that stimulus. The field of psychophysics usually distinguishes between four conventional ways of measuring perception. Detection and discrimination measures are the most fundamental aspects of perception and are complemented by identification and scaling measures (Coren et al. 2003a). Detection and discrimination tasks are both aimed at establishing thresholds, i.e., the minimum intensity at which a stimulus can be perceived, in case of a detection task, and the minimum intensity at which a difference between two stimuli can be perceived, in case of a discrimination task. Identification tasks assess the participant’s ability to attach a label or to name a certain stimulus, whereas scaling tasks require the participant to assign relative values to their perceptions. Identification and scaling tasks are assumed to involve higher cognitive functions, such as semantic memory, and are, therefore, referred to as “Complex Perception” in this review. Table 1 presents an overview of the four psychophysical approaches for studying perception and their definitions. In addition to reviewing objective psychophysical studies on perception in ADHD, we included studies using self- and informant reports in our review in order to account for the subjective experiences of patients and observations of patients’ behaviors in response to perceptual stimuli. In exploratory analysis of the reviewed studies, we aimed at identifying variables which may moderate perceptional functioning in ADHD. Furthermore, possible implications of the findings of the present review for daily life functioning and clinical practice will be discussed.
Methods
A systematic search of the existing literature was conducted in the scientific databases PubMed and PsycINFO including all available literature up until the date of June 10, 2016. The search term “ADHD” was combined with terms signifying aspects of perception (see Table 2 for the detailed search strategy). We filtered results to only include English- and German-written literature on human subjects of all age groups (i.e., children/adolescents and adults), published in peer-reviewed academic journals. Reference lists of identified studies were used to identify additional studies. Duplicates were removed, and titles and abstracts of remaining records were screened. Finally, full-text articles were assessed for eligibility.
Inclusion criteria
For inclusion, each study had to feature all of the following criteria.
Clinical diagnosis
A study had to include a group of subjects who received an expert clinical diagnosis of ADHD according to DSM-III-R criteria, or according to criteria of newer DSM editions, or according to ICD-10 criteria (American Psychiatric Association 1987; World Health Organization 1992). For studies with an uncertain origin of ADHD diagnoses, diagnoses had to be confirmed by diagnostic or screening instruments specific to ADHD, such as the Adult ADHD Self-Report Scale (Kessler et al. 2005) or the Conners’ Adult ADHD Rating Scales (Conners et al. 1999).
Normal control (NC) group
The patient group had to be compared to a psychiatric and neurologically healthy NC group. A single study conducted by Gansler et al. (1998) did not include a NC group as a comparison, instead, this study compared patients with the ADHD-hyperactive/impulsive subtype to patients of the ADHD-inattentive subtype. As this study may contribute to the understanding of perceptional functioning in ADHD, we nevertheless included it in our systematic review.
Assessment of perception
In order to be included in the review, a study had either to utilize at least one of the four psychophysical methods of measuring perception (i.e., detection, discrimination, identification, scaling; see Table 1), or to evaluate self- or informant reports on perceptual functioning. Studies investigating higher levels of perception with high attentional demands were excluded from the present review as perceptual demands cannot be clearly differentiated from demands in attentional resources in these studies, e.g., when participants were requested to select stimuli among streams of sensory input, such as orienting, filtering, searching, or preparing. Studies using other ways of measuring perception (e.g., electrophysiological studies) were also not taken into account for the systematic review.
Group comparisons
A study had to present its data in a way which allows group comparisons between individuals with ADHD and NCs, i.e., by indicating the significance of a difference, as well as by deriving the effect size of a group difference (Cohen’s d). According to Cohen’s conventional guidelines effect sizes of 0.20 ≤ d < 0.50 are considered as small, whereas effect sizes of 0.50 ≤ d < 0.80 and d ≥ 0.80 are considered as moderate and large size, respectively (Cohen 1977). The effect size phi φ was calculated for one study conducting Chi-square tests to investigate differences in frequency data between groups. Effect sizes of φ ≥ 0.10 are considered as small, whereas effect sizes of φ ≥ 0.30 and φ ≥ 0.50 are considered as moderate and large size, respectively (Cohen 1992).
Results
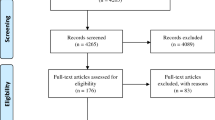
The systematic search identified 36 studies published between 1996 and 2016 which examined perceptual functioning in ADHD and NCs. An overview of the systematic search is illustrated in Fig. 1. Study characteristics and effect sizes are shown in Table 3. Identified studies included data on children and adults and were grouped into the following categories (1) psychophysical studies, including studies on auditory perception, gustatory perception, olfactory perception, tactile perception, and visual perception, and (2) self-/informant-based studies, including self- and informant reports on perception.

PRISMA flow diagram. Selection of studies according to the guidelines of preferred reporting items for systematic reviews and meta-analyses (PRISMA)
Psychophysical studies (objective measurements)
Auditory perception
The present review includes seven studies on auditory perception of individuals with ADHD. Given the observed nonsignificant differences of small size, it can be concluded that the detection of pure tones in children with ADHD is largely intact compared to NCs (Cohen’s d ranged from 0.25 to 0.33, Breier et al. 2002, 2003; Gray et al. 2002). It should, however, be noted that Breier et al. (2003) did report an overall effect of ADHD on several psychoacoustic tasks which was revealed by a repeated measures analysis of variance (ANOVA). Since the authors did not present any post hoc analyses, we conducted simple group comparisons for tone detection tasks on the basis of the statistical information reported in the paper of Breier et al. (2002). Results of this comparison could not reveal significant group differences, with only small effect sizes (Cohen’s d = 0.32 for 32 mms tones and Cohen’s d = 0.25 for 512 ms tones) and are, thus, in agreement with the findings reported by Breier et al. (2002) and Gray et al. (2002).
Breier et al. (2003) also examined tone discrimination in ADHD and NCs. Again, no post hoc analyses were carried out. Our calculated group differences failed to reach statistical significance with, yet, a small effect size (Cohen’s d = 0.41), indicating that participants with ADHD had a slightly, although not significantly, higher detection threshold compared to NCs.
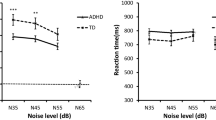
Two auditory perception studies investigated recognition thresholds for speech sounds and reported thresholds to be significantly reduced in children with ADHD when compared to NCs, with medium to large effect sizes; Cohen’s d ranged from 0.74 to 0.89 (Lucker et al. 1996; Söderlund and Jobs 2016). Moreover, symptoms of inattention and hyperactivity were found to be related to reduced speech recognition thresholds (Söderlund and Jobs 2016). Notably, Söderlund and Jobs (2016) did not include any girls in their study, and Lucker et al. (1996) included around 79 and 65% males in the ADHD and NC group, respectively.
Lucker et al. (1996) also examined perceived loudness and found that children with ADHD required significantly softer levels to judge speech as comfortable or as tolerable compared to NCs, with large effect sizes; Cohen’s d ranged from 0.88 to 1.06, with slightly smaller effects found in the left ear condition than in the right ear condition (Lucker et al. 1996). In addition, compared to NCs, children with ADHD had a significantly narrower dynamic range which is the difference between speech recognition threshold and tolerance level of speech loudness. A large effect size was found for this difference (Cohen’s d = 1.13).
Word identification ability of auditory presented words is often tested with the Goldman–Fristoe–Woodcock Test of Auditory Discrimination (GFW; Goldman et al. 1970). This test requires participants to make word-picture associations by pointing at the picture of a word they have heard, with four-alternative response options. Performance of adults and children with ADHD did not differ significantly from performance of NCs on this test; group differences were negligible (d = 0.14 for differences between adults with ADHD and NCs; d = 0.03 for differences between children with ADHD and NCs; Corbett and Stanczak 1999; Geffner et al. 1996). When word identification was, however, tested with the NU-6 Test which requires participants to verbally repeat presented words (Tillman and Carhart 1966), children with ADHD were found to have significantly reduced word identification ability for the right ear. Group differences were of small to medium size (d = 0.55 for right ear; d = 0.36 for left ear).
Gustatory perception
So far, information on gustatory perception is scarce with only one study examining this type of perception in ADHD (Weiland et al. 2011). The authors found no significant difference in the identification rates of different tastes (sweet, sour, bitter, and no taste) for children with ADHD and NCs with a negligible effect size (d = 0.03). However, patients with ADHD perceived bitter taste as significantly more intense compared to NCs. The effect size we could calculate for this difference was large (φ = 0.53). Moreover, we estimated that the odds of being sensitive to bitter taste were 15.50 times greater for someone with ADHD than for a NC participant.
Olfactory perception
Results of the present review indicate that stimulant medication naïve children with ADHD had significantly lower olfactory detection thresholds compared to NCs, as indicated by large effects of 1.25 and 1.26 (Cohen’s d) (Romanos et al. 2008; Lorenzen et al. 2016). Furthermore, olfactory bulb volume was shown to be significantly increased in children with ADHD as compared to NCs (Lorenzen et al. 2016). In contrast, children with ADHD who regularly take stimulant medication as well as adults with ADHD with and without medication do not seem to differ significantly from NCs in their ability to detect odors, as underlined by negligible to small effect sizes; Cohen’s d ranged from 0.03 to 0.39 (Romanos et al. 2008; Schecklmann et al. 2011a, b; Weiland et al. 2011).
Olfactory discrimination was found to be largely similar in ADHD and NCs, as shown by nonsignificant differences of negligible to small size; Cohen’s d ranged from 0.08 to 0.43 (Romanos et al. 2008; Schecklmann et al. 2011a, b). One study (Schecklmann et al. 2011b), however, employed a within-subjects design and revealed equal (nonsignificantly different) olfactory discrimination in children with ADHD on stimulants during the assessment and NCs, with a small effect size (d = 0.43), but significantly improved olfactory discrimination in the same children who had not taken any stimulant medication prior to the assessment. The effect found for this group difference was of medium, nearly large size (d = 0.79).
Two studies found olfactory identification to be significantly reduced in children and adults with ADHD, when compared to NCs with small to large effect sizes; Cohen’s d ranged from 0.39 to 2.01 (Murphy et al. 2001; Karsz et al. 2008). Three further studies could not reveal any significant group differences, with only negligible to small effect sizes; Cohen’s d ranged from 0.09 to 0.33 (Romanos et al. 2008; Schecklmann et al. 2011a, b). It should be noted that studies which failed to find significant group differences utilized a different task, the so-called Sniffin’ Sticks test (Burghart Instruments, Germany), than studies which did find significant group differences. Another study found that patients with the ADHD-inattentive subtype demonstrated significantly lower identification performance compared to patients with the ADHD-hyperactive/impulsive subtype (Gansler et al. 1998). Moreover, Murphy et al. (2001), who initially found significantly reduced performance on the University of Pennsylvania Smell Identification Test (UPSIT) for the ADHD group, reported that these differences were reduced to non-significance when accounted for IQ.
Tactile perception
Tactile discrimination thresholds were found to be intact in children with ADHD on a task requiring participants to discriminate between smooth and rough paper sheets, as indicated by a nonsignificant difference of small size (d = 0.34) (Parush et al. 1997). However, compared to NCs, children with ADHD were less able to actually differentiate between painful and non-painful stimuli, as indicated by a significant difference of medium size (d = 0.59) (Scherder et al. 2008).
Evidence for over-responsivity to pain in ADHD was presented by Treister et al. (2015) who found decreased cold pain thresholds and decreased cold pain tolerance in adults with ADHD. Compared to NCs, adults with ADHD showed significantly reduced cold pain tolerance when they were not on stimulant medication during the assessment, with a large effect size (d = 0.91). When patients with ADHD were on medication, they did not differ significantly from NCs in pain tolerance (d = 0.29). Furthermore, the groups did not differ significantly in cold pain scaling; a self-report measure where participants had to indicate their maximal experience pain intensity during the pain tolerance assessment, with negligible to small effect sizes; Cohen’s d ranged from 0.05 to 0.21.
Visual perception
One aspect of visual perception is the ability to discern between luminances of different intensity, called contrast sensitivity. Results concerning contrast sensitivity were inconsistent. One study reported significantly reduced contrast sensitivity in children with the ADHD-combined subtype compared to NCs, with medium effect sizes (Cohen’s d ranged from 0.63 to 0.73; Bartgis et al. 2009), while two further studies failed to find significantly reduced contrast sensitivity in ADHD, with observed negligible to small effect sizes; Cohen’s d ranged from 0.10 to 0.38 (Kim et al. 2015; Stevens et al. 2012). One of these studies found that medicated patients with ADHD who stopped stimulant medication for at least 24 h prior to the assessment had a lower, although not significantly lower, detection threshold compared to non-medicated patients, with a medium effect size (d = 0.57 for binocular vision; Kim et al. 2015). However, it should be noted that patients who took stimulant medication were mostly those with attentional problems. Moreover, age varied across studies, namely Bartgis et al. (2009) studied contrast sensitivity in children, whereas Kim et al. (2015) and Stevens et al. (2012) and colleagues tested adolescents and adults, respectively. Finally, differences between studies may also be attributable to differences in test measures. While Bartgis et al. (2009) utilized the Functional Acuity Contrast Test (FACT; Ginsburg 1998), Kim et al. (2015) used the Pelli–Robson Contrast Sensitivity Test (Pelli et al. 1988) and Stevens et al. (2012) used a test they designed specifically for this study.
Kim et al. (2014a) did not find any significant differences between adults with ADHD and NCs in performance on a contrast discrimination task, where participants had to decide which stimulus out of two (sinusoidal gratings) “looks higher in contrast”. Our calculated Cohen’s d for the difference in contrast discrimination between men with ADHD and men in the NC group was found to be small (d = 0.21), whereas the Cohen’s d for the differences between women with and without ADHD was found to be of medium size (d = 0.63). Since the samples were divided according to gender, rather small subsamples remained for these comparisons (15 individuals per group). In combination with the medium effect size found for differences between females with ADHD and NCs, it may be that this test was underpowered.
Kim et al. (2014a) also investigated color saturation discrimination which is the ability to discriminate between different intensities of a specific hue and found that females with ADHD had significantly reduced color saturation discrimination compared to females of the NC group, with large effect sizes; Cohen’s d ranged from 0.85 to 1.01 (Kim et al. 2014a). Males with ADHD did not differ significantly from their male peers.
A further aspect of visual perception, hue (color) discrimination, is the ability to discriminate between different tones of color (i.e., red, blue, green). Adults with ADHD performed largely similar compared to NCs on hue discrimination tasks, with nonsignificant differences of negligible to medium size; Cohen’s d ranged from 0.11 to 0.51 (Kim et al. 2014a, b). Merely one study reported deficits for adults with ADHD along the blue spectrum only, as indicated by a significant effect of medium size (d = 0.58; Kim et al. 2014b). In contrast, children with ADHD appear to have deficits in hue discrimination, especially along the blue-yellow axis (as indicated by significant effects of large size; Cohen’s d ranged from 1.06 to 1.23), but they also seem to have difficulties with color discrimination along the red-green axis, as shown by significant effects of medium to large size; Cohen’s d ranged from 0.75 to 0.98 (Banaschewski et al. 2006; Roessner et al. 2008).
Self- and informant reports (subjective measurements)
A total of 15 subjective studies with 10 informant reports and 5 self-reports on perception in ADHD were identified. Study characteristics and calculated effect sizes are shown in Table 4. The most commonly utilized measurement was the Sensory Profile (Dunn 1999) and variants of it, i.e., the Short Sensory Profile (McIntosh et al. 1999) and the Chinese Sensory Profile (Tseng and Cheng 2008), all being parent-report questionnaires. These questionnaires contain items on sensory processing, modulation, and behavioral outcomes in relation to perception. Parents report the frequency with which their child engages in each behavior. For the present review, we only investigated subscales explicitly pertaining to the five senses (“auditory processing,” “visual processing,” “touch processing,” “oral processing,” and “taste/smell processing”). Results point to significantly more perception problems in ADHD compared to NCs. Differences of medium to mostly large effect sizes (Cohen’s d ranging from 0.52 to 2.75) became evident in all studies and on all subscales. Yochman et al. (2007) found nearly half of the children with ADHD in their sample to have deficits on the Sensory Profile. Perceptual problems were found to be most pronounced in the auditory domain, with large effect sizes; Cohen’s d ranged from 1.17 to 2.75. Moreover, compared to NCs, children with ADHD showed a significant increase in sensory processing issues with increasing age, especially for auditory processing (Cheung and Siu 2009). Auditory processing difficulties have also been found to be related to lower participation in social, recreational, and informal activities (Engel-Yeger and Ziv-On 2011). Furthermore, symptoms of anxiety and of hyperactivity were found to be related to overall scores on the Sensory Profile (Yochman et al. 2004; Lane et al. 2010). Symptoms of inattention have been linked to abnormalities in auditory processing, whereas symptoms of hyperactivity and aggression have been connected to abnormalities in tactile perception (Mangeot et al. 2001; Shimizu et al. 2014). Finally, comorbidity was found to be related to more perceptional abnormalities (Shimizu et al. 2014).
Two studies utilized subjective measures specific to touch and found that children with ADHD were over-responsive to tactile stimuli (Parush et al. 1997; Bröring et al. 2008). The studies examined tactile defensiveness of individuals, which describes a disturbance in sensory processing with the tendency to react negatively and emotionally to certain touch situations. Individuals with “tactile defensiveness” avoid touch and interpret many forms of touch as threatening. Bröring et al. (2008) investigated tactile defensiveness in school-aged children and reported that 17% of females and 3% of males with ADHD were classified as being tactile defensive, suggesting that levels of tactile defensiveness may vary according to gender, with female patients showing higher levels of tactile defensiveness than male patients. Results of this study stand in contrast to the study conducted by Parush et al. (1997) that investigated tactile defensiveness in male preschoolers and revealed that 39.5% of participants with ADHD and no NC children were classified as being tactile defensive. It has been suggested that the different results may be explained by differences in measures (Bröring et al. 2008). Whereas Parush et al. (1997) used the Touch Inventory for Preschoolers (Royeen 1987) which is based on teacher-reports, Bröring et al. (2008) used the Touch Inventory for Elementary-School-Aged Children (Royeen and Fortune 1990), based on self-reports.
Scherder et al. (2008) utilized the Children’s Pain Inventory (McGrath et al. 1996) to assess the self-reported intensity of recently experienced pain and found self-reported intensity or emotionality of past experienced pain to be equal in children with ADHD and NCs. This finding stands in contrast to various self- and informant reports on abnormal tactile perception in ADHD.
Visual perception assessed by self-report measurements such as the Visual Activities Questionnaire (VAQ; Sloane et al. 1992) was found to be largely intact, as shown by nonsignificant effects of small to medium size; Cohen’s d ranged from 0.24 to 0.51. One study, however, found participants with ADHD to report significantly more visual problems on depth perception, peripheral vision, visual search, visual processing speed and when driving compared to NCs, with medium to large effect sizes; Cohen’s d ranged from 0.57 to 1.23 (Kim et al. 2014b).
The Sensory Gating Inventory (SGI; Hetrick et al. 2012), a self-report measurement, assesses (1) perceptual modulation (e.g., “My hearing is so sensitive that ordinary sounds become uncomfortable”), (2) over-inclusion (e.g., “I notice background noises more than other people”), (3) distractibility by sensory stimuli (e.g., “There are times when I can’t concentrate with even the slightest sounds going on”), and (4) fatigue-stress modulation (e.g., “it seems that sounds are more intense when I’m stressed”). Two studies utilized this questionnaire and reported significantly deviant scores for participants with ADHD on all subscales compared to NCs, with large effect sizes; Cohen’s d ranged from 1.26 to 3.28 (Micoulaud-Franchi et al. 2015a, b). The domain most severely affected in both studies was the distractibility domain, with large effect sizes; Cohen’s d ranged from 2.59 to 3.28. It should be noted that self-reported deficits on this domain might rather be attributable to symptoms of inattention than to perceptual problems. In line with this speculation, it was found that symptoms of inattention were related to SGI scores, especially to the distractibility dimension and the fatigue dimension. One study investigated next to the SGI, also the auditory event-related potential P50, and found significantly lower P50 suppression in ADHD compared to NCs indicating altered pre-attentive information processing in ADHD (Micoulaud-Franchi et al. 2015b). Moreover, the authors found a significant negative correlation between P50 suppression and SGT scores.
Discussion
The purpose of the present systematic review was to determine whether individuals with ADHD differ from healthy NCs without neurological and psychiatric conditions in aspects of perception (i.e., auditory, gustatory, olfactory, tactile, and visual perception), to quantify these differences, to evaluate the meaning of obtained results, and finally, to discuss implications. To this end, we examined studies on psychophysical measures, as well as subjective self- and informant reports on perceptual functioning. A total of 25 psychophysical studies with k = 8 on olfactory perception, k = 7 on auditory perception, k = 7 on visual perception, k = 3 on tactile perception, and k = 1 on gustatory perception were investigated. In addition, 13 subjective studies with k = 10 informant reports and k = 4 self-reports were reviewed. The most fundamental concepts of measuring perception are detection and difference threshold measures, involving the least amount of higher cognitive functions. For these reasons, results on fundamental perception tasks are discussed in distinction from results on perception tasks probably involving higher cognitive functions.
Fundamental perception in ADHD
One of the most striking results of the present review was the finding of improved olfactory detection in stimulant medication naïve children with ADHD, which seems to normalize by enduring effects of stimulant medication and possibly by age. Moreover, stimulant medication naïve children with ADHD were found to have an increased olfactory bulb volume. The olfactory bulb is a highly plastic brain region with dopamine playing a central role in it (Bonzano et al. 2016), providing a biological basis for the finding of improved olfactory detection in ADHD. Normalization of olfactory detection accompanied by stimulant medication treatment in ADHD may be associated with modulation of dopaminergic neurotransmission. Another fundamental olfactory function, i.e., olfactory discrimination, was also found to be affected by stimulant medication, namely a within-subjects study found olfactory discrimination to be increased in non-medicated patients with ADHD at the time of the assessment, but it was found to be normal in chronically medicated patients who also took medication at testing. It has been suggested that the methodological differences between olfactory detection and olfactory discrimination studies may account for the divergent effects of stimulants on the olfactory domains (Schecklmann et al. 2011a). Olfactory discrimination may be affected by short-lasting changes related to cessation of stimulant treatment, whereas long-term treatment may lead to chronic effects on olfactory detection in ADHD. Based on these findings, it has been suggested that olfactory detection may be a useful biomarker for ADHD (Schecklmann et al. 2011a; Thome et al. 2012). Since olfactory alterations in other psychiatric or neurological conditions point to reduced functioning, improved olfactory detection in ADHD may be specific to this disorder, especially considering the large effect sizes (Cohen’s d ≈ 1.25). However, further studies are needed in order to validate this new discovery. In line with psychophysical findings of increased olfactory detection in ADHD are parent-reports suggesting that compared to their typically developing peers, children with ADHD are more sensitive to olfactory stimuli (Cheung and Siu 2009; Lane et al. 2010; Mangeot et al. 2001). Thus, results of more objective psychophysical measures are echoed in parent-reports on olfactory perception in ADHD.
Studies on color discrimination in children with ADHD point to perceptual problems, especially for the blue-yellow axis, but also the red-green axis appears to be affected. In line with the finding of impaired blue-yellow color discrimination in ADHD is a study which found that opposed to red-green stimuli, blue-yellow stimuli resulted in decreased performance of participants with ADHD in a virtual reality computer game (Silva and Frère 2011). Results for color discrimination in adults with ADHD are inconsistent with one study finding decreased discrimination for the blue spectrum only, while another study could not reveal any differences between patients and NCs. In conclusion, it appears that color discrimination is differentially affected in children and adults with ADHD. It is very likely that adults with ADHD have developed compensation strategies to account for their perceptual problems in color discrimination. This finding is supported by the notion of a decreased color naming speed in adults with ADHD (Tannock et al. 2000; Banaschewski et al. 2006; Kim et al. 2014a, b). Moreover, greater amplitudes in the P1, an event-related potential in response to blue-yellow stimuli but not to red-green stimuli has been found in adolescents with ADHD which is assumed to indicate compensatory mechanisms for color deficiency that adolescents with ADHD develop over time (Kim et al. 2015). Self-reports on color discrimination in adults with ADHD could not reveal any deficits in this aspect of visual perception and are, therefore, in line with psychophysical studies on color discrimination in adults with ADHD.
Results on contrast sensitivity in ADHD are inconsistent with only three studies examining this type of perception in ADHD. One of these studies revealed deficits in ADHD, while the remaining two studies failed to reveal any significant group differences. Several factors, such as age, stimulant medication use, and symptoms of attention, may have contributed to the observed differences between studies. It is known that attention plays a critical role in contrast sensitivity (Carrasco et al. 2004). Since most patients with ADHD suffer from attentional impairments, a potential relationship between attentional problems and contrast sensitivity should be further investigated in ADHD. Inconsistency of study results may also be attributable to differences between measures. Bartgis et al. (2009) who found decreased contrast sensitivity in ADHD used the FACT, whereas Kim et al. (2015) and Stevens et al. (2012) who could not find any alterations in contrast sensitivity in ADHD used the Pelli–Robson Contrast Sensitivity Test and a homemade test, respectively. The gratings varying in contrast used in the FACT appear to be a more sensitive measure of contrast sensitivity compared to letters and numbers varying on contrast used in the Pelli–Robson Contrast Sensitivity Test and in the study by Stevens et al. (2012). This hypothesis is supported by a study revealing that the sizes of the letters tested by the Pelli–Robson chart are too large in order to be meaningful to everyday viewing and that the sensitivity of the FACT is greater than the sensitivity of the Pelli–Robson chart (Ginsburg 2003).
The remaining reviewed fundamental aspects of perception, namely auditory tone detection and discrimination, as well as tactile discrimination of rough and smooth paper stimuli appear to be intact in ADHD. This finding is not in line with self- and informant reports revealing increased tactile and auditory abnormalities in ADHD (Bröring et al. 2008; Cheung and Siu 2009; Dunn and Bennett 2002; Engel-Yeger and Ziv-On 2011; Mangeot et al. 2001; Parush et al. 1997; Shimizu et al. 2014). It should be noted that the recording of subjective reports does not aim at detecting pure perceptual deficits. Questionnaires measuring subjective pain contain items including various aspects of processing perceptual income, including aspects of attention. For example, one item on the Sensory Profile examines whether the participant has difficulty standing in line or close to people. Obtaining a problem score on this item does not necessarily reflect abnormalities in tactile perception. In fact, part of this item is also specified as an ADHD symptom of hyperactivity/impulsivity in the DSM-5 (American Psychiatric Association 2000). Therefore, it remains to be investigated whether reported tactile and auditory abnormalities in ADHD reflect tactile perceptional problems in the psychophysical sense, or whether these abnormalities can be explained by ADHD symptomatology.
One aspect of fundamental tactile perception, the perception of pain, however, does appear to be affected in patients with ADHD. More specifically, children with ADHD were less able to actually differentiate between painful and non-painful stimuli (Scherder et al. 2008). However, it should be noted that this study is not a traditional psychophysical discrimination study, but rather a qualitative examination of the participant’s tactile functions. In this study, contrary to traditional psychophysical studies, stimuli did not vary in intensity, but participants were exposed to each stimulus three times and had to indicate the temperature (cold or warm) or the sharpness (sharp or blunt). Number of errors (maximum of 6 for each test) was the dependent variable. Since the authors did not report whether patients with ADHD confused more blunt stimuli with sharp ones, or vice versa, or whether errors were equally distributed (the same holds for the temperature test), it remains to be unclear whether patients with ADHD are under- or over-responsive to pain, or whether they are indeed less able to differentiate between painful and non-painful tactile stimuli. Furthermore, adults with ADHD seem to have an increased sensitivity to cold water, an index of pain, which seems to normalize with the acute administration of stimulant medication (when given at the time of the assessment). This finding is in line with reports on increased prevalence of pain in ADHD (Kessler et al. 2009; Stray et al. 2013). It is known that dopamine plays a central role in pain perception (Wood 2008) and that ADHD is associated with alterations of the dopaminergic system (Albayrak et al. 2008; Thome and Reddy 2009). On the basis of these observations, it has been suggested that altered pain perception in ADHD may be related to alterations of the dopaminergic system (Treister et al. 2015). In contrast to the finding of altered pain perception in ADHD, as revealed by psychophysical studies, patients with ADHD do not seem to differ from NCs on self-reported levels of pain intensity (Scherder et al. 2008; Treister et al. 2015), demonstrating that objective pain assessments are not be in line with the subjective experience of painful stimuli.
Complex perception in ADHD
Findings indicate that individuals with ADHD perform as well as NCs on a rather brief test of olfactory identification, the Sniffin’ Sticks test, but perform worse on a more enduring test, the University of Pennsylvania Smell Identification Test (UPSIT). The UPSIT consists of 40 items, whereas the Sniffin’ Sticks test only consists of 16 items. It may, therefore, be the case that the UPSIT requires more attentional resources compared to the Sniffin’ Sticks and may, thus, place greater demands on attentional resources which caused patients with ADHD to perform lower on the UPSIT only. Indeed, research shows that olfactory identification, as opposed to olfactory detection, depends on executive functions and semantic memory (Hedner et al. 2010). Moreover, the present review identified a study reporting reduced olfactory identification in patients with the ADHD-inattentive subtype when compared to the ADHD-hyperactive/impulse subtype (Gansler et al. 1998) suggesting that symptoms of inattention may affect performance on the UPSIT. Finally, Murphy et al. (2001), who initially found reduced performance on the UPSIT for the ADHD group, reported that these differences were reduced to non-significance when accounted for IQ. To conclude, findings of the present review suggest that olfactory identification may be moderated by higher cognitive functions. However, this assumption needs verification by, for example, studies that investigate the causal relationships between higher cognitive functions and olfactory identification in ADHD.
In contrast to speech detection and discrimination, speech recognition seems to be reduced in ADHD. Research has shown that speech recognition thresholds are related to higher cognitive functions, such as working memory and attention (Lunner 2003; Xie et al. 2015). Given that patients with ADHD often experience working memory and attention problems, it may be speculated that lower speech recognition thresholds in ADHD are related to deficits in higher cognitive functions. Indeed, the present review found reduced speech recognition thresholds in ADHD to be associated with symptoms of inattention. Taken together, it seems that reduced speech recognition thresholds in ADHD are rather related to neurocognitive problems than to auditory perceptual problems per se. The exact mechanisms of this finding are subject to further research.
Although children with ADHD appear to have an increased speech recognition threshold, at the same time, they require softer levels of speech to judge speech as comfortable or as tolerable compared to their typically developing peers. Compared to NCs, they have a narrower dynamic range (i.e., a smaller difference between speech recognition threshold and tolerance level). Hence, children with ADHD appear to be overly sensitive to speech sounds, which are judged to be normally tolerable and normally comfortable by NCs. The underlying mechanisms of increased sensitivity to speech sounds in ADHD remain to be investigated. It has, however, been suggested that deficits in the sensory gating of auditory information might be accountable (Lucker et al. 1996). This hypothesis is in line with the finding of reduced P50 suppression in ADHD, a neurophysiological measure of sensory gating (Micoulaud-Franchi et al. 2015b). Taken together, the finding of increased sensitivity to speech sounds in combination with decreased P50 suppression in ADHD suggests that auditory information may not be adequately filtered in this disorder. In line with this are also results of reviewed self- and informant reports pointing to problems with auditory processing in ADHD (Cheung and Siu 2009; Engel-Yeger and Ziv-On 2011).
Word identification appears to be intact in children and adults with ADHD when tested with the GFW. This test does not involve any verbal responses, but participants are given four-choice closed-response options and are required to point at the picture of a word they think they have heard. However, children with ADHD do demonstrate deficits in word identification when required to verbally repeat auditory presented words on the NU-6 Test, especially when words were presented to the right ear. The NU-6 test was developed for adults, and research shows that, in comparison with both a test not requiring any verbal response and an open-response test developed for children, this test is the most difficult for children (Sanderson-Leepa and Rintelmann 1976). Word familiarity and even small maturation effects play a significant role in mastering this test. Unfortunately, Geffner et al. (1996) did not report on mean ages of the two groups or on other group characteristics such as education. It may, thus, have been the case that unrevealed group differences caused children with ADHD to perform below NCs on the NU-6 test. Lower performances on these tests of children with ADHD in combination with normal performance on the GFW in adults with ADHD may reflect a delay in neurodevelopmental trajectories evident in this disorder (Shaw et al. 2010). In general, it appears that the more complex perception of speech recognition is reduced in children with ADHD, possibly related to attentional problems associated with this disorder, while findings on word identification, even though inconsistent, point to intact functioning.
So far, only one study has investigated gustatory perception in ADHD and found that women with ADHD perceive bitter stimuli as more intense than NCs do, while taste identification seems to be intact in women with ADHD (Weiland et al. 2011). Results of this study should be replicated, especially in the light of small sample sizes used in this study (n = 12 per group) and the fact that this study included female participants only. Parent-reports on oral processing point to abnormalities in ADHD. More psychophysical studies on taste perception are needed in order to determine whether the parents’ reports of increased oral processing problems can be substantiated.
Interestingly, patients with ADHD appear to have increased visual problems when driving as revealed by one of the reviewed self-report studies suggesting that visual perceptual problems indeed affect the daily lives of patients. Moreover, Kim et al. (2014b) revealed that patients with ADHD reported perceptual problems in depth perception, peripheral vision, visual search, and visual processing speed, domains strongly affected by neurocognitive functions, but not in “purer” measures of visual perception, such as color discrimination, glare disability, light/dark adaption, and acuity/spatial vision. Informant reports on visual function in ADHD, however, suggest rather pronounced deficits in ADHD. Again, it should be stressed that informant reports do not aim at detecting pure perceptual deficits but rather problems related to perceptual processing. Findings on visual perception in ADHD stress the importance of detangling perception and cognitive functions and suggest that attention may influence several aspects of visual perception.
Potential moderator variables
Results of the present review were quite heterogeneous. In this respect, we identified some evidence that reported effects were moderated by several variables causing heterogeneity between studies. For instance, differences in test measures may have contributed to the observed differences between studies on contrast sensitivity. Evidence for deficits in contrast sensitivity in ADHD was only found by a study that used the FACT to assess this type of visual perception. The FACT is a very sensitive measure of contrast sensitivity, and instruments used in other studies may not have been sensitive enough to detect subtle impairments. Differential study results for olfactory identification in ADHD also seem to be related to differences in test measures applied with time/sustained attention likely being the decisive factor moderating performance. Individuals with ADHD were found to perform as well as NCs on a rather brief test of olfactory identification, the Sniffin’ Sticks test, but perform worse on a more enduring test, the UPSIT. Furthermore, word identification in children with ADHD was found to be moderated by test measure. Children with ADHD displayed no deficits on a rather easy nonverbal test of word identification but had difficulties on a test requiring verbal responses. In general, it appears that test measures that place greater demands on higher cognitive functions resulted in reduced performance in individuals diagnosed with ADHD. Whether problems on these tasks underlie real perceptual deficits remains to be investigated.
ADHD symptoms and higher cognitive functions were also likely to moderate outcomes on several perceptual tests. For example, symptoms of inattention and hyperactivity were found to be related to reduced speech recognition thresholds (Söderlund and Jobs 2016), auditory processing problems (Shimizu et al. 2014), and possibly moderate performance on contrast sensitivity (Bartgis et al. 2009). Moreover, individuals with ADHD appear to have more visual perceptual problems in tasks requiring attention. Symptoms of hyperactivity were found to be related to overall problem scores on the Sensory Profile as well as informant reported tactile abnormalities. Furthermore, it is likely that ADHD symptoms contributed to the observed high problem scores on self- and informant reports, since these measurements cannot disentangle perception and higher cognitive functions. Most items of these measures assess higher cognitive functions in addition to “pure” perceptual functioning.
Gender was found to moderate performance on several visual perceptual tests with female but not male patients demonstrating deficits on tests of contrast discrimination and color saturation discrimination. Considering this finding, it is possible that females with ADHD also have undetected problems on other visual perceptual tasks. Age possibly affects performance on contrast sensitivity, hue (color) discrimination, and olfactory detection. Moreover, sensory processing problems in individuals with ADHD appear to increase with age.
Lastly, acute administration of stimulant medication was found to moderate performance on olfactory detection and olfactory discrimination tasks. Abstinence from stimulant medication seems to be related to enhanced olfactory perception. Acute administration of stimulant medication also seems to normalize cold pain sensitivity and cold pain tolerance in ADHD.
In conclusion, perception in ADHD may be affected by several moderating variables, whereas further evidence is needed in order to support our conclusions and speculations. Moreover, it is warranted to investigate the magnitude of moderating variables on perception in ADHD and to examine to what extent individuals with ADHD are affected by real alterations in perception.
Implications for daily life functioning and clinical practice
Alterations in perception in ADHD as revealed by the present review may influence daily life functioning of patients and may have important consequences for clinical practice. For instance, contrast sensitivity is important for various daily live tasks, such as driving at night, reading, face recognition, and finding objects (Owsley 2003), some of which individuals with ADHD have difficulties with (Jerome et al. 2006; Markovska-Simoska and Pop-Jordanova 2010; American Psychiatric Association 2013). In addition, it was found that individuals with ADHD report more visual problems while driving compared to NCs (Kim et al. 2014b). Alterations in speech perception may also have widespread implications for the daily life of patients with ADHD. For instance, children with ADHD might perceive their teacher’s voice to be uncomfortably loud or not sufficiently loud in order to adequately process what has been said. Considering that children spend 45% to 60% of their school day listening (Rosenberg et al. 1999), alterations in speech recognition may interfere with adequate learning and development. Moreover, we identified evidence for elevated pain levels in ADHD. Elevated levels of pain have a negative impact on attention (Moore et al. 2012). For patients with ADHD who often already suffer from attentional problems, higher sensitivity to pain would, therefore, place additional burden on their attentional resources, possibly affecting daily life functioning. Finally, difficulties in auditory processing were found to be related to reduced participation in several types of activities, including social and physical activities (Engel-Yeger and Ziv-On 2011). This finding is supported by research suggesting that children with ADHD are less intensively involved in social and physical activities (Shimoni et al. 2010). Lower engagement in various types of activities may deprive patients from important learning experiences, affecting daily life functioning. Reduced functioning on daily live tasks may severely affect patients’ quality of life, and it is, therefore, crucial to investigate the relationship between perceptual and daily life functioning in ADHD systematically.
Alterations in perceptional functioning may not only influence daily live activities, but they may also affect conclusions drawn in clinical practice. For instance, perceptual alterations in ADHD may account for some neuropsychological impairments that have been associated with this disorder. Neuropsychological and perceptual functions are tightly interrelated and influence each other. Consequently, not only perceptual impairments might be over-estimated in ADHD (because of the cognitive difficulties), there is also a fair chance that cognitive impairments are over-interpreted because of the perceptual problems. Potential color discrimination deficits in ADHD question, for instance, the validity of neuropsychological test results which depend on intact color perception. For example, intact visual perception is a prerequisite for mastering many neuropsychological tests, such as the Stroop test (Kim et al. 2014b). It is, therefore, important to further investigate visual perception in ADHD and its relation to ADHD symptoms and assessment measures applied.
Limitations and future directions
Some limitations of the investigated studies and the review itself should be noted. First, sample sizes of reviewed psychophysical studies were often small, such that results may not be practically meaningful. For example, Kim et al. (2014a) concluded contrast discrimination to be equal in women with ADHD and NCs, basing their results on a subgroup of their sample with 15 subjects per group only. The small sample size in combination with a medium effect size (d = 0.63) suggests that the group comparison may have been underpowered. Since the same authors found color saturation discrimination to be reduced in females with ADHD, a potential gender effect in ADHD for contrast discrimination seems to be plausible. Future studies should include larger sample sizes in order to find effects of a magnitude large enough to be practically meaningful and to be generalizable to the population.
Second, studies often did not control for higher cognitive functions and ADHD symptoms. As discussed above, we nowadays know that cognitive functioning can affect various aspects of perception, such as olfactory identification (Hedner et al. 2010) and contrast sensitivity (Carrasco et al. 2004). Since ADHD is associated with various neuropsychological problems such as inattention or deficits in executive functions (Thome et al. 2012), we do not know whether decreased performance in individuals with ADHD on perceptual tasks relying on higher cognitive functions reflects perceptual or cognitive problems. Therefore, future studies should account for neuropsychological functioning and ADHD symptoms when studying perception in ADHD.
Third, results of the present review suggest that acute administration of stimulant medication moderates some aspects of perception, such as olfactory detection (Romanos et al. 2008; Schecklmann et al. 2011b) and pain sensitivity (Treister et al. 2015). Most studies, however, did not investigate potential long- or short-term effects of stimulant medication on perception. It may, therefore, be possible that some perceptual alterations in ADHD can be explained by the effects of stimulant medication treatment. Future research should be aimed at investigating potential medication effects in order to gain a better understanding of perceptual functions in ADHD.
Another limitation of the present review was that we compared studies on different age groups. As perceptional functions changes throughout the entire life span (Coren et al. 2003b), comparing different age groups is not desirable. It would be particularly interesting if longitudinal research is performed in order to study the effect of age on various perceptual functions in ADHD.
Finally, it must be noted that in the present review we compared studies using different methods to study perception. As already pointed out, subjective self- and informant report measurements cannot disentangle perception and higher cognitive function and are, therefore, not comparable to psychophysical studies. They, however, provide valuable additional information about patients’ experiences and the observations of patients’ reactions to perceptional stimuli. Further research may aim at investigating the relationship between subjective and objective studies on perception in ADHD. The latter two paragraphs describe limitations we could not avoid in our review, as we can only review the studies that are available. Currently, the number of studies on perception in ADHD is still small and the measures as well as designs applied are unfortunately very heterogeneous.
Conclusion
Overall, results of the present review point to alterations in both fundamental and more complex aspects of perception in ADHD. Perceptual abnormalities on olfactory detection and cold pain sensitivity may be related to dopaminergic alterations associated with ADHD. Deficits on more complex perceptual tasks, such as speech recognition, however, may rather be related to problems in higher cognitive functions than to perceptional deficits per se. Perception and higher cognitive functions are tightly related. Perceptual problems in ADHD may, therefore, aggravate symptoms of inattention, and symptoms of inattention may modulate perception in ADHD. Alterations in one domain altering functioning in the other may place additional burden on affected patients. Hence, it is crucial to disentangle perception and cognitive functions in ADHD as much as possible in order to gain a better understanding of mechanisms underlying ADHD symptoms which is of clinical and theoretical importance.
The present review also revealed that individuals with ADHD experience discomfort to sensory stimuli at a lower level than NCs do; they require lower levels of speech to judge speech as comfortable or as tolerable; they rate a bitter stimulus more intense; and they have a lower cold pain threshold as opposed to NCs. Hence, it appears that individuals with ADHD are more sensitive to several perceptual stimuli. Decreased speech comfortable and tolerance levels may be related to sensory gating deficits. Deficits in sensory gating may also be associated with increased sensitivity to bitter taste and cold pain.
Although individuals with ADHD are not affected by profound fundamental perceptual deficits, virtually all self- and informant reports on perceptual functions revealed significant problems in ADHD. Perception in the real-world is certainly more complex than psychophysical tests under laboratory conditions which may explain differences between psychophysical studies and subjective self- and informant reports. Perception and cognitive functions are highly interrelated, and subjective studies cannot control for this interrelation. An increased number of reported perceptual problems may also indicate problems with processing and/or responding to perceptual income.
The present review identified several implications of altered perception in ADHD. For instance, olfactory detection may be a potential biomarker for ADHD. Moreover, in light of potential alterations in perceptual functioning, the validity of neuropsychological tests relying on intact perception must be questioned in individuals with ADHD. Furthermore, children with ADHD may have difficulties in perceiving their teachers’ voices and may experience their teachers’ voices as uncomfortably loud which might lead to difficulties concentrating. Also potential alterations in contrast sensitivity may affect various domains of daily live.
In conclusion, research on perception in ADHD is scare with heterogeneous assessment methods and results. Future studies are warranted to in order to address open questions mentioned above and to draw firm conclusions.
References
Albayrak Ö, Friedel S, Schimmelmann GB et al (2008) Genetic aspects in attention-deficit/hyperactivity disorder. J Neural Transm 115:305–315. doi:10.1007/s00702-007-0839-9
Albrecht B, Uebel-von Sandersleben H, Gevensleben H, Rothenberger A (2015) Pathophysiology of ADHD and associated problems—starting points for NF interventions? Front. Hum. Neurosci 9:359. doi:10.3389/fnhum.2015.00359
American Psychiatric Association (1987) Diagnostic and statistical manual of mental disorders, 3rd ed. American Psychiatric Publishing, Washington
American Psychiatric Association (2000) Diagnostic and statistical manual of mental disorders, 4th ed. Washington
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Publishing, Arlington
Arnsten A, Li B (2005) Neurobiology of executive functions: catecholamine influences on prefrontal cortical functions. Biol Psychiatry 57:1377–1384. doi:10.1016/j.bps.2004.08.019
Bamiou D-E (2001) Aetiology and clinical presentations of auditory processing disorders—a review. Arch Dis Child 85:361–365. doi:10.1136/adc.85.5.361
Banaschewski T, Ruppert S, Tannock R et al (2006) Colour perception in ADHD. J Child Psychol Psychiatry 47:568–572. doi:10.1111/j.1469-7610.2005.01540.x
Bar-Shalita T, Vatine J-J, Parush S (2008) Sensory modulation disorder: a risk factor for participation in daily life activities. Dev Med Child Neurol 50:932–937. doi:10.1111/j.1469-8749.2008.03095.x
Bartgis J, Lefler EK, Hartung CM, Thomas DG (2009) Contrast sensitivity in children with and without attention deficit hyperactivity disorder symptoms. Dev Neuropsychol 34:663–682. doi:10.1080/87565640902964474
Bellgrove MA, Hawi Z, Lowe N et al (2005) DRD4 gene variants and sustained attention in attention deficit hyperactivity disorder (ADHD): effects of associated alleles at the VNTR and -521 SNP. Am J Med Genet Neuropsychiatr Genet 136 B:81–86. doi:10.1002/ajmg.b.30193
Bonzano S, Bovetti S, Gendusa C et al (2016) Adult Born Olfactory bulb dopaminergic interneurons: molecular determinants and experience-dependent plasticity. Front Neurosci 10:1–8. doi:10.3389/fnins.2016.00189
Breier JI, Gray LC, Klaas P et al (2002) Dissociation of sensitivity and response bias in children with attention deficit/hyperactivity disorder during central auditory masking. Neuropsychology 16:28–34. doi:10.1037/0894-4105.16.1.28
Breier JI, Fletcher JM, Foorman BR et al (2003) Auditory temporal processing in children with specific reading disability with and without attention deficit/hyperactivity disorder. J Speech Lang Hear Res 46:31–42. doi:10.1044/1092-4388(2003/003)
Bröring T, Rommelse N, Sergeant J, Scherder E (2008) Sex differences in tactile defensiveness in children with ADHD and their siblings. Dev Med Child Neurol 50:129–133. doi:10.1111/j.1469-8749.2007.02024.x
Büttner T, Schulz S, Kuhn W et al (1994) Impaired colour discrimination in Huntington’s disease. Eur J Neurol 1:153–157. doi:10.1111/j.1468-1331.1994.tb00064.x
Cahen A, Tacca MC (2013) Linking perception and cognition. Front Psychol 4:144. doi:10.3389/fpsyg.2013.00144
Carrasco M, Ling S, Read S (2004) Attention alters appearance. Nat Neurosci 7:308–313. doi:10.1038/nn1194
Cave JW, Baker H (2009) Dopamine systems in the forebrain. Adv Exp Med Biol 651:15–35. doi:10.1007/978-1-4419-0322-8_2
Cheung PPP, Siu AMH (2009) A comparison of patterns of sensory processing in children with and without developmental disabilities. Res Dev Disabil 30:1468–1480. doi:10.1016/j.ridd.2009.07.009
Cohen J (1977) Statistical power analysis for the behavioral sciences, rev edn. Lawrence Erlbaum Associates Inc, Hillsdale
Cohen J (1992) A power primer. Psychol Bull 112:155–159. doi:10.1037/0033-2909.112.1.155
Conners CK, Erhardt D, Sparrow E (1999) Conner’s adult ADHD rating scales: CAARS: technical manual. Multi-Health Systems, North Tonawanda
Corbett B, Stanczak DE (1999) Neuropsychological performance of adults evidencing attention-deficit hyperactivity disorder. Arch Clin Neuropsychol 14:373–387. doi:10.1016/S0887-6177(98)00037-7
Coren S, Ward LM, Enns JT (2003a) Measuring perception. In: Sensation and perception, 6th edn. Wiley, New York, pp 13–41
Coren S, Ward LM, Enns JT (2003b) Development. In: Sensation and perception. Wiley, New York, pp 449–470
Doty RL (2012) Olfaction in Parkinson’s disease and related disorders. Neurobiol Dis 46:527–552. doi:10.1016/j.nbd.2011.10.026
Dunn W (1999) The sensory profile. The Psychological Corporation, San Antonio
Dunn W (2001) The sensations of everyday life: empirical, theoretical, and pragmatic considerations. Am J Occup Ther 55:608–620. doi:10.5014/ajot.55.6.608
Dunn W, Bennett D (2002) Patterns of sensory processing in children with attention deficit hyperactivity disorder. Occup Ther J Res 22(1):4–15. doi:10.1177/153944920202200102
Engel-Yeger B, Ziv-On D (2011) The relationship between sensory processing difficulties and leisure activity preference of children with different types of ADHD. Res Dev Disabil 32:1154–1162. doi:10.1016/j.ridd.2011.01.008
Fuermaier ABM, Tucha L, Koerts J et al (2015) Cognitive impairment in adult ADHD—perspective matters! Neuropsychology 29(1):45–58. doi:10.1037/neu0000108
Gansler DA, Fucetola R, Krengel M et al (1998) Are there cognitive subtypes in adult attention deficit/hyperactivity disorder? J Nerv Ment Dis 186:776–781. doi:10.1097/00005053-199812000-00006
Geffner D, Lucker JR, Koch W (1996) Evaluation of auditory discrimination in children with ADD and without ADD. Child Psychiatry Hum Dev 26(3):169–180. doi:10.1007/BF02353358
Ginsburg AP (1998) Functional acuity contrast test FACT. Stereo Optical Inc, Chicago
Ginsburg AP (2003) Contrast sensitivity and functional vision. Int Ophthalmol Clin 43:5–15. doi:10.1097/00004397-200343020-00004
Goldman R, Fristoe M, Woodcock R (1970) The Goldman–Fristoe–Woodcock test of auditory discrimination. American Guidance Service, Circle Pines
Goldstein S, Jansen J (2008) The neuropsychology of ADHD. In: MacNeil Horton A, Wedding D (eds) The neuropsychology handbook, 3rd edn. Springer Publishing Co, New York, pp 651–680
Gray LC, Breier JI, Foorman BR, Fletcher JM (2002) Continuum of impulsiveness caused by auditory masking. Int J Pediatr Otorhinolaryngol 66:265–272
Hedner M, Larsson M, Arnold N et al (2010) Cognitive factors in odor detection, odor discrimination, and odor identification tasks. J Clin Exp Neuropsychol 32:1062–1067. doi:10.1080/13803391003683070
Hetrick WP, Erickson MA, Smith DA (2012) Phenomenological dimensions of sensory gating. Schizophr Bull 38:178–191. doi:10.1093/schbul/sbq054
Hsia AY, Vincent J-D, Lledo P-M (1999) Dopamine depresses synaptic inputs into the olfactory bulb. J Neurophysiol 82:1082–1085
Jerome L, Segal A, Habinski L (2006) What we know about ADHD and driving risk: a literature review, meta-analysis and critique. J Can Acad Child Adolesc Psychiatry 15:105–125
Kapur S, Mizrahi R, Li M (2005) From dopamine to salience to psychosis-linking biology, pharmacology and phenomenology of psychosis. Schizophr Res 79:59–68. doi:10.1016/j.schres.2005.01.003
Karsz FR, Vance A, Anderson VA et al (2008) Olfactory impairments in child attention-deficit/hyperactivity disorder. J Clin Psychiatry 69:1462–1468. doi:10.4088/JCP.v69n0914
Kashino M, Kondo HM (2012) Functional brain networks underlying perceptual switching: auditory streaming and verbal transformations on JSTOR. Philos Trans Biol Sci 367:977–987. doi:10.1098/rstb.2011.0370
Kessler RC, Adler L, Ames M et al (2005) The World Health Organization adult ADHD self-report scale (ASRS): a short screening scale for use in the general population. Psychol Med 35:245–256. doi:10.1017/S0033291704002892
Kessler RC, Lane M, Stang PE, van Brunt DL (2009) The prevalence and workplace costs of adult attention deficit hyperactivity disorder in a large manufacturing firm. Psychol Med 39:137–147. doi:10.1017/S0033291708003309
Kim S, Al-Haj M, Chen S et al (2014a) Colour vision in ADHD: part 1—Testing the retinal dopaminergic hypothesis. Behav Brain Funct 10:38. doi:10.1186/1744-9081-10-38
Kim S, Chen S, Tannock R (2014b) Visual function and color vision in adults with attention-deficit/hyperactivity disorder. J Optom 7:22–36. doi:10.1016/j.optom.2013.07.001
Kim S, Banaschewski T, Tannock R (2015) Color vision in attention-deficit/hyperactivity disorder: a pilot visual evoked potential study. J Optom 8:116–130. doi:10.1016/j.optom.2014.10.002
Lane SJ, Reynolds S, Thacker L (2010) Sensory over-responsivity and ADHD: differentiating using electrodermal responses, cortisol, and anxiety. Front Integr Neurosci 4:8. doi:10.3389/fnint.2010.00008
Lange KW, Hauser J, Lange KM et al (2014) Utility of cognitive neuropsychological assessment in attention deficit/hyperactivity disorder. Atten Def Hyp Disord 6:241–248. doi:10.1007/s12402-014-0132-3
Li S-C, Passow S, Nietfeld W et al (2013) Dopamine modulates attentional control of auditory perception: DARPP-32 (PPP1R1B) genotype effects on behavior and cortical evoked potentials. Neuropsychologia 51:1649–1661. doi:10.1016/j.neuropsychologia.2013.04.005
Lindenberger U, Baltes PB (1997) Intellectual functioning in old and very old age: cross-sectional results from the Berlin Aging Study. Psychol Aging 12:410–432. doi:10.1037/0882-7974.12.3.410
Lorenzen A, Scholz-Hehn D, Wiesner CD et al (2016) Chemosensory processing in children with attention-deficit/hyperactivity disorder. J Psychiatr Res 76:121–127. doi:10.1016/j.jpsychires.2016.02.007
Lucker JR, Geffner D, Koch W (1996) Perception of loudness in children with ADD and without ADD. Child Psychiatry Hum Dev 26:181–190
Lunner T (2003) Cognitive function in relation to hearing aid use. Int J Audiol 42:49–58. doi:10.3109/14992020309074624
Majic T, Rentzsch J, Gudlowski Y et al (2011) COMT Val108/158Met genotype modulates human sensory gating. Neuroimage 55:818–824. doi:10.1016/j.neuroimage.2010.12.031
Mangeot SD, Miller LJ, McIntosh DN et al (2001) Sensory modulation dysfunction in children with attention-deficit-hyperactivity disorder. Dev Med Child Neurol 43:399–406
Markovska-Simoska S, Pop-Jordanova N (2010) Face and emotion recognition by ADHD and normal adults. Acta Neuropsychol 8:99–122
McGrath PA, Seifert CE, Speechley KN et al (1996) A new analogue scale for assessing children’s pain: an initial validation study. Pain 64:435–443. doi:10.1016/0304-3959(95)00171-9
McIntosh DN, Miller LJ, Shyu V (1999) Development and validation of the short sensory profile. In: Dunn W (ed) Sensory profile manual. Psychological Corporation, San Diego, pp 59–73
Melun JP, Morin LM, Muise JG, DesRosiers M (2001) Color vision deficiencies in Gilles de la Tourette syndrome. J Neurol Sci 186:107–110
Micoulaud-Franchi J-A, Lopez R, Vaillant F et al (2015a) Perceptual abnormalities related to sensory gating deficit are core symptoms in adults with ADHD. Psychiatry Res 230:357–363. doi:10.1016/j.psychres.2015.09.016
Micoulaud-Franchi J-A, Vaillant F, Lopez R et al (2015b) Sensory gating in adult with attention-deficit/hyperactivity disorder: event-evoked potential and perceptual experience reports comparisons with schizophrenia. Biol Psychol 107:16–23. doi:10.1016/j.biopsycho.2015.03.002
Moberg PJ, Doty RL, Mahr RN et al (1997) Olfactory identification in elderly schizophrenia and alzheimer’s disease. Neurobiol Aging 18:163–167. doi:10.1016/S0197-4580(97)00015-8
Moberg PJ, Kamath V, Marchetto DM et al (2014) Meta-analysis of olfactory function in schizophrenia, first-degree family members, and youths at-risk for psychosis. Schizophr Bull 40:50–59. doi:10.1093/schbul/sbt049
Moore DJ, Keogh E, Eccleston C (2012) The interruptive effect of pain on attention. Q J Exp Psychol 65:565–586. doi:10.1080/17470218.2011.626865
Müller CP, Huston JP (2007) Dopamine activity in the occipital and temporal cortices of rats: dissociating effects of sensory but not pharmacological stimulation. Synapse 61:254–258. doi:10.1002/syn.20366
Murphy KR, Barkley RA, Bush T (2001) Executive functioning and olfactory identification in young adults with attention deficit-hyperactivity disorder. Neuropsychology 15:211–220. doi:10.1037/0894-4105.15.2.211
Owsley C (2003) Contrast sensitivity. Ophthalmol Clin North Am 16:171–177. doi:10.1016/S0896-1549(03)00003-8
Parush S, Sohmer H, Steinberg A, Kaitz M (1997) Somatosensory functioning in children with attention deficit hyperactivity disorder. Dev Med Child Neurol 39:464–468. doi:10.1111/j.1469-8749.1997.tb07466.x
Pelli D, Robson JG, Wilkins AJ (1988) The design of a new letter chart for measuring contrast sensitivity. Clin Vis Sci 2:187–199
Pieri V, Diederich NJ, Raman R, Goetz CG (2000) Decreased color discrimination and contrast sensitivity in Parkinson’s disease. J Neurol Sci 172:7–11. doi:10.1016/S0022-510X(99)00204-X
Polanczyk G, de Lima MS, Horta BL et al (2007) The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry 164:942–948. doi:10.1176/ajp.2007.164.6.942
Roessner V, Banaschewski T, Fillmer-Otte A et al (2008) Color perception deficits in co-existing attention-deficit/hyperactivity disorder and chronic tic disorders. J Neural Transm 115:235–239. doi:10.1007/s00702-007-0817-2
Romanos M, Renner TJ, Schecklmann M et al (2008) Improved odor sensitivity in attention-deficit/hyperactivity disorder. Biol Psychiatry 64:938–940. doi:10.1016/j.biopsych.2008.08.013
Rosenberg GG, Blake-Rahter P, Heavner J et al (1999) Improving classroom acoustics (ICA): a three-year FM sound field classroom amplification study. J Educ Audiol 7:8–28
Roy A, Roy M, Berman J, Gonzalez B (2003) Blue cone electroretinogram amplitudes are related to dopamine function in cocaine-dependent patients. Psychiatry Res 117:191–195. doi:10.1016/S0165-1781(02)00323-2
Royeen CB (1987) TIP—touch inventory for preschoolers: a pilot study. Phys Occup Ther Pediatr 7:29–40. doi:10.1300/J006v07n01_04
Royeen CB, Fortune JC (1990) Touch inventory for elementary-school-aged children. Am J Occup Ther 44:155–159. doi:10.5014/ajot.44.2.155
Sanderson-Leepa ME, Rintelmann WF (1976) Articulation functions and test-retest performance of normal-hearing children on three speech discrimination tests: WIPI, PBK-50, and NU Auditory Test No. 6. J Speech Hear Disord 41:503–519
Schecklmann M, Schaldecker M, Aucktor S et al (2011a) Effects of methylphenidate on olfaction and frontal and temporal brain oxygenation in children with ADHD. J Psychiatr Res 45:1463–1470. doi:10.1016/j.jpsychires.2011.05.011
Schecklmann M, Schenk E, Maisch A et al (2011b) Altered frontal and temporal brain function during olfactory stimulation in adult attention-deficit/hyperactivity disorder. Neuropsychobiology 63:66–76. doi:10.1159/000323448
Scherder EJA, Rommelse NNJ, Broring T et al (2008) Somatosensory functioning and experienced pain in ADHD-families: a pilot study. Eur J Paediatr Neurol 12:461–469. doi:10.1016/j.ejpn.2007.11.004
Sharma A, Couture J (2014) A review of the pathophysiology, etiology, and treatment of attention-deficit hyperactivity disorder (ADHD). Ann Pharmacother 48:209–225
Shaw P, Gogtay N, Rapoport J (2010) Childhood psychiatric disorders as anomalies in neurodevelopmental trajectories. Hum Brain Mapp 31:917–925. doi:10.1002/hbm.21028
Shimizu VT, Bueno OFA, Miranda MC (2014) Sensory processing abilities of children with ADHD. Braz J Phys Ther 18:343–352. doi:10.1590/bjpt-rbf.2014.0043
Shimoni M, Engel-Yeger B, Tirosh E (2010) Participation in leisure activities among boys with attention deficit hyperactivity disorder. Res Dev Disabil 31:1234–1239. doi:10.1016/j.ridd.2010.07.022
Silva AP, Frère AF (2011) Virtual environment to quantify the influence of colour stimuli on the performance of tasks requiring attention. Biomed Eng Online 10:74. doi:10.1186/1475-925X-10-74
Sloane ME, Ball K, Owsley C et al (1992) The visual activities questionnaire: developing an instrument for assessing problems in everyday visual tasks. Tech Dig Noninvasive Assess Vis Syst 1:26–29
Söderlund GBW, Jobs EN (2016) Differences in speech recognition between children with attention deficits and typically developed children disappear when exposed to 65 dB of auditory noise. Front Psych 7:34. doi:10.3389/fpsyg.2016.00034
Stevens AA, Maron L, Nigg JT et al (2012) Increased sensitivity to perceptual interference in adults with attention deficit hyperactivity disorder. J Int Neuropsychol Soc 18:511–520. doi:10.1017/S1355617712000033
Stray LL, Kristensen Ø, Lomeland M et al (2013) Motor regulation problems and pain in adults diagnosed with ADHD. Behav Brain Funct 9:1–10. doi:10.1186/1744-9081-9-18
Tacca MC (2011) Commonalities between perception and cognition. Front Psychol 2:358. doi:10.3389/fpsyg.2011.00358
Tallal P, Miller S, Fitch RH (1993) Neurobiological basis of speech: a case for the preeminence of temporal processing. Ann N Y Acad Sci 682:27–47. doi:10.1111/j.1749-6632.1993.tb22957.x
Tannock R, Martinussen R, Frijters J (2000) Naming speed performance and stimulant effects indicate effortful, semantic processing deficits in attention-deficit/hyperactivity disorder. J Abnorm Child Psychol 28:237–252. doi:10.1023/A:1005192220001
Thapar A, Cooper M, Eyre O, Langley K (2013) Practitioner review: what have we learnt about the causes of ADHD? J Child Psychol Psychiatry 54:3–16. doi:10.1111/j.1469-7610.2012.02611.x
Thome J, Reddy DP (2009) The current status of research into attention deficit hyperactivity disorder: proceedings of the 2nd international congress on ADHD: from childhood to adult disease. ADHD Atten Deficit Hyperact Disord 1:165–174. doi:10.1007/s12402-009-0016-0
Thome J, Ehlis A, Fallgatter AJ et al (2012) Biomarkers for attention-deficit/hyperactivity disorder (ADHD). A consensus report of the WFSBP task force on biological markers and the world federation of ADHD. World J Biol Psychiatry 13:379–400. doi:10.3109/15622975.2012.690535
Tillman TW, Carhart R (1966) An expanded test for speech discrimination utilizing CNC monosyllablic words: Northwestern University Auditory Test No. 6. USAF School of Aerospace Medicine, Brooks Air Force Base, TX
Treister R, Eisenberg E, Demeter N, Pud D (2015) Alterations in pain response are partially reversed by methylphenidate (Ritalin) in adults with attention deficit hyperactivity disorder (ADHD). Pain Pract 15:4–11. doi:10.1111/papr.12129
Tseng MH, Cheng TJ (2008) Sensory profile-Chinese version. Chinese Behavioral Science Corporation, Taipei
Tucha L, Tucha O, Laufkoetter R et al (2008) Neuropsychological assessment of attention in adults with different subtypes of attention-deficit/hyperactivity disorder. J Neural Transm 115:269–278. doi:10.1007/s00702-007-0836-z
Wasserstein J (2005) Diagnostic issues for adolescents and adults with ADHD. J Clin Psychol 61:535–547. doi:10.1002/jclp.20118
Weiland R, Macht M, Ellgring H et al (2011) Olfactory and gustatory sensitivity in adults with attention-deficit/hyperactivity disorder. Atten Defic Hyperact Disord 3:53–60. doi:10.1007/s12402-010-0052-9
Wood PB (2008) Role of central dopamine in pain and analgesia. Expert Rev Neurother 8:781–797. doi:10.1586/14737175.8.5.781
World Health Organization (1992) The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. World Health Organization, Geneva
Xie Z, Maddox WT, Knopik VS et al (2015) Dopamine receptor D4 (DRD4) gene modulates the influence of informational masking on speech recognition. Neuropsychologia 67:121–131. doi:10.1016/j.neuropsychologia.2014.12.013
Yochman A, Parush S, Ornoy A (2004) Responses of preschool children with and without ADHD to sensory events in daily life. Am J Occup Ther 58:294–302. doi:10.5014/ajot.58.3.294
Yochman A, Ornoy A, Parush S (2007) Co-occurrence of developmental delays among preschool children with attention-deficit-hyperactivity disorder. Dev Med Child Neurol 48(6):483–488. doi:10.1111/j.1469-8749.2006.tb01300.x
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was conducted in compliance with ethical standards as outlined in the current version of the Helsinki Declaration (2013).
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Fuermaier, A.B.M., Hüpen, P., De Vries, S.M. et al. Perception in attention deficit hyperactivity disorder. ADHD Atten Def Hyp Disord 10, 21–47 (2018). https://doi.org/10.1007/s12402-017-0230-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12402-017-0230-0