
Abstract
This systematic review aimed to evaluate the prognostic value of Iodine123 Metaiodobenzylguanidine (123I-mIBG) SPECT myocardial imaging in patients with heart failure (HF) and to assess whether semi-quantitative SPECT scores can be useful for accurate risk stratification concerning arrhythmic event (AE) and sudden cardiac death (SCD) in this cohort. A systematic literature search of studies published until November 2020 regarding the application of 123I-mIBG SPECT in HF patients was performed, in Pubmed, Scopus, Medline, Central (Cochrane Library) and Web Of Science databases, including the words “MIBG”, “metaiodobenzylguanidine”, “heart”, “spect”, and “tomographic”. The included studies had to correlate 123I-mIBG SPECT scores with endpoints such as overall survival and prevention of AE and SCD in HF patients. According to the sixteen studies included, the analysis showed that 123I-mIBG SPECT scores, such as summed defect score (SDS), regional wash-out (rWO), and regional myocardial tracer uptake, could have a reliable prognostic value in patients with HF. An increased SDS or rWO, as well as a reduced 123I-mIBG myocardial uptake, have proven to be effective in predicting AE- and SCD-specific risk in HF patients. Despite achieved results being promising, a more reproducible standardized method for semi-quantitative analysis and further studies with larger cohort are needed for 123I-mIBG SPECT myocardial imaging to be as reliable and, thus, accepted as the conventional 123I-mIBG planar myocardial imaging.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Heart failure (HF) is characterized by several abnormalities of sympathetic cardiac activity: an increased sympathetic response is initially favorable by serving as compensation for decreased cardiac output, but as HF progresses this response leads to deleterious neurohormonal and myocardial structural changes that worsen the condition and increase the likelihood of adverse cardiac events.1
Iodine123-Metaiodobenzylguanidine (123I-mIBG), an analog of norepinephrine, is a useful tool for detecting abnormalities in the myocardial adrenergic nervous system in HF patients and can be successfully used to assess their prognosis.2,3,–4123I-mIBG represents a tracer of sympathetic neuron integrity and function and the most widely used imaging agent for studying the causes and effects of cardiac sympathetic hyperactivity.5 Semi-quantitative myocardial 123I-mIBG parameters have proved to be of prognostic value in HF.6,7 Specifically, some trials were designed to assess the capability of the heart to mediastinum ratio (H/M) on 123I-mIBG planar scintigraphy for predicting prognosis for significant adverse cardiac events in subjects with HF.8 Currently, the H/M is the basis for the clinical decision-making diagnostic work-up, enabling the common application of a single standardized parameter beyond worldwide institutions.9,10 Several single and multicenter studies demonstrated and confirmed its potent prognostic role in the clinical evaluation and risk stratification in HF.11,12 HF patients with impaired myocardial 123I-mIBG parameters had a worse prognosis compared with those with relatively preserved parameters (i.e., reduced late H/M and increased myocardial wash-out rate (WR)).13 However, it has become progressively more common to include single-photon emission computerized tomography (SPECT) imaging in clinical and research protocol.14 Myocardial SPECT imaging allows evaluation of the regional sympathetic activity and polar maps of the myocardium could be obtained by SPECT images, providing an assessment of the defect extent and severity.15,16 Furthermore, the ability of 123I-mIBG SPECT to provide regional information not available on planar images remains a driver for efforts to incorporate this procedure into assessments of HF patients with arrhythmic events (AE) and sudden cardiac death (SCD) specific risk.17,18 Despite PET imaging holds higher spatial resolution and superior quantitative capabilities,19,20 for the forthcoming future 123I-mIBG SPECT accounts for the most widely available nuclear imaging technique for an accurate assessment of the regional myocardial sympathetic innervation.21 Nonetheless, a shared and established consent of these 123I-mIBG SPECT parameters is found to be hard to get according to the present knowledge. Therefore, to date, there is an urgent need for improved risk stratification for patients developing HF and growing evidence that 123I-mIBG SPECT imaging should gain greater clinical relevance. The aim of this systematic review is to evaluate the prognostic value of 123I-mIBG SPECT myocardial imaging in patients with HF and to assess whether semi-quantitative SPECT scores can be useful for accurate risk stratification with regard to AE and SCD.
Materials and Methods
Search Strategy and Study Selection
This systematic review was drawn up following PRISMA guidelines.22 An online literature search looking up articles that suited the inclusion criteria was conducted on Pubmed, Scopus, Medline, Central (Cochrane Library), and Web Of Science databases. Papers published from January 1950 to November 2020 concerning HF patients assessed by means of 123I-mIBG SPECT were searched. The applied search query was the following: ((MIBG* [WORD] OR metaiodobenzylguanidine [WORD]) AND (heart [WORD]) AND (spect [WORD] OR tomographic [WORD])). This string was then adapted for each database. Eligible studies had to take into consideration semi-quantitative scores expressly derived by myocardial SPECT imaging, like regional wash-out rate (rWO) and summed scores (SS) values. Studies were included when these scores were correlated with specific endpoints, such as overall survival (OS) and prevention of AE and SCD. Reviews, case reports, editorials, studies conducted on animals or phantoms, and studies concerning oncologic conditions were excluded. The English language was mandatory for inclusion in the analysis. References of the provided articles were also examined to find out any additional relevant studies.
Data Extraction and Methodological Quality Assessment
For each included study, general data about the article (authors, journal, year of publication, country, and study design) along with patient characteristics were retrieved.
The methodological quality of included studies was assessed using the Quality Assessment of Diagnostic accuracy Studies-2 (QUADAS2) tool. Since its publication in 2003,23 the QUADAS tool has been widely used24,25 and it is recommended for use in systematic reviews of diagnostic accuracy by the Agency for Healthcare Research and Quality, Cochrane Collaboration (Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy), and the U.K. National Institute for Health and Clinical Excellence. Data extraction and quality assessment were independently performed by two reviewers and eventual disagreements were resolved by unanimous approval after discussion.
Results
Search Results
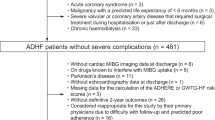
A total of 315 articles were found and thus the authors examined each abstract to identify potentially suitable studies. From the overall group of 315, 204 full-text articles concerning patients with neuroblastoma,14 pheochromocytoma (105), and Parkinson’s disease (62) were excluded. 23 articles were excluded because they did not satisfy the inclusion criteria. The 111 remaining papers were assessed for eligibility with the exclusion of 28 papers with no SPECT data. 16 articles were considered suitable and ultimately selected for this review. The detailed study selection flow chart, along with the search strategy and the selection criteria applied, is represented in Figure 1.

Study selection flow chart
Study Characteristics
Characteristics of the included studies and technical acquisition parameters used to obtain 123I-mIBG myocardial SPECT imaging are reported in Tables 1 and 2. The number of enrolled patients in the analyzed studies ranged from 16 to 985, the latter corresponding with the ADMIRE-HF multicenter trial cohort.26 The selected articles were published from 1995 to 2020 by researchers mostly from the USA and Europe, but also one from Japan and another study from Australia. Subjects enrolled were essentially patients with stable NYHA Class II or III HF (ischemic or non-ischemic) at risk for an adverse cardiac event (i.e., AE or SCD), including subjects referred for ICD implantation for primary prevention of SCD.
Methodological Quality
The overall methodological quality of the included studies resulted quite good: 12 of 16 studies satisfied at least three and 9 of 16 all of the four QUADAS2 domains for the bias risk assessment and 10 of 16 satisfied each of the three applicability assessment domains, with 12 satisfying at least two domains (Table 3). Considering independently the results within each bias assessment domain, at least 11 studies obtained a low concern of bias and no more than 2 studies showed high risk in some of those (Figure 2A, B). Conversely, taking into account all four bias assessment domains, only two studies reported more than two unclear results, in relation to an insufficient amount of details given to achieve an acceptable methodological protocol appraisal, and only one reported a high risk of bias in two of the four domains. Regarding the patient selection domain, three studies had an unclear risk of bias because there was a lack of detailed data and/or it was not reported whether patients were consecutively enrolled. Two studies reported a high risk of bias because some heterogeneity within the inclusion criteria was detected. Regarding the index test domain, two studies reported a high risk of bias due to some kind of different elaboration and interpretation of the 123I-mIBG myocardial SPECT imaging, bringing the risk to decrease the global homogeneity and power of the findings. It was found a high concern of applicability, both in patient selection and index test domains, in three studies. Cumulatively, given four high risks, and one unclear result obtained if considering both patient selection and index test domain, the concern for global applicability was mainly low (Figure 3A, B).

(A) Risk of bias assessment through Quadas2 for each study. (B) Results of risk of bias assessment through Quadas2 along with its graphic representation

(A) Applicability concerns assessment through Quadas2 for each study. (B) Results of applicability concerns assessment through Quadas2 along with its graphic representation
Statistical analysis
A random-effects meta-analysis was also carried out, but it had a very large heterogeneity as measured by the I2. In accordance with the recommendations of the Cochrane Oral Health Group, we therefore decided not to report on this analysis.
Discussion
In patients with chronic HF, sympathetic hyperactivity initially represents a compensatory mechanism for coping with impaired myocardial function. However, long-term elevated adrenergic stimulation generates a vicious circle which leads in the end to detrimental myocardial remodeling, decline in left ventricular function, and increased morbidity and mortality.27 Cardiac sympathetic activity could be non-invasively assessed with 123I-mIBG myocardial SPECT imaging since the internalization of this tracer in presynaptic endings of post-ganglionic neuronal cells.28,29 Several studies proved that parameters derived by myocardial planar scintigraphy with 123I-mIBG play a significant prognostic role in chronic HF, with particular regard to the H/M value.30,31,–32 However, in recent times, following the conversion from planar to SPECT tomographic techniques in clinical nuclear myocardial perfusion imaging (MPI), also 123I-mIBG SPECT imaging it has become progressively more common in clinical and research protocols.5,33 Early and late 123I-mIBG SPECT images were scored visually with 20- and 17-segment regional polar maps, also known as bull’s-eye maps. Additionally, segmental counts data were used to calculate regional wash-out rate (rWO) in some studies. In patients with HF, the reduced uptake of norepinephrine in presynaptic neurons determines a lower mIBG uptake (decreased H/M) and an increased WR, due to an increased release rate. Such patients are eligible for implantable cardioverter-defibrillator (ICD) implantation. The dominant observation was that the larger the extent of the 123I-mIBG SPECT abnormality, the higher the likelihood of ventricular tachyarrhythmia.34123I-mIBG scintigraphy was approved after the multicenter prospective study ADMIRE-HF showed a significant correlation between decreased late H/M and increased risk of HF progression, ventricular tachyarrhythmia, and death.26 Several studies investigated the prognostic value of 123I-mIBG scintigraphy in patients with chronic HF. A systematic review explored the prognostic significance of 123I-mIBG planar-imaging-derived parameters and indicated that patients with HF and decreased late H/M or increased WO, have a worse prognosis compared with patients with normal parameters.27
To date few studies, mainly evaluating relatively small samples of patients, focused on the prognostic significance of 123I-mIBG SPECT imaging derived parameters. Basically, data obtained by SPECT tomographic imaging have been applied in the same way as planar scintigraphic ones: to evaluate the potential correlation between 123I-mIBG semi-quantitative uptake scores and specific outcomes, like the occurrence of AE and SCD.35,36 Therefore, this systematic review aimed to collect sets of SPECT quantitative data from published studies to derive more accurate evidence of their prognostic value; a systematic process was adopted to avoid all possible selection bias. The methodological work-up in conducting a systematic review carries unavoidably with it some biases and limitations. First of all publication itself represents a primary source of bias as studies showing significant results are more likely to be published than studies reporting non-significant findings, therefore only complete studies taking into account the role of 123I-mIBG SPECT imaging in relation with planar imaging were considered. Therapy could represent another potential source of bias. In most of the studies included in this systematic review, the authors stated that the patient population was treated with either beta-blockers, Angiotensin-converting-enzyme inhibitors (ACE), or Angiotensin II Receptor Blockers (ARBs), but this was not homogeneous criteria. Only some authors specified that the patients were not undergoing treatment with tricyclic antidepressants or other medications that are known to interfere with mIBG uptake.37,38 The inclusion criteria were homogeneous for most but not all studies (NYHA class II or III, left ventricular ejection fraction LVEF ≤35%, indication for ICD implantation) hence the heterogeneity of the patient population can represent an additional source of bias. In particular, since most of the samples were extracted from patients affected by chronic HF, the absent discrimination between ischemic and non-ischemic events among such patients could be a source of error. 12 out of 16 studies assembling SPECT slices in polar maps of 17 segments were performed on patients with chronic HF, in order to predict AE or SCD in such patients. In these studies, the tracer uptake was graded on a scale of 0-4 (0=normal; 1=mildly reduced; 2=moderately reduced; 3=severely reduced; 4 = absent), and the SDS was calculated by summing the scores for each segment. All these studies stated that an increased summed score is suggestive of an increased risk for AE or SCD and associated with a worse prognosis in such patients. Most of the patients with an increased summed score also show a H/M ratio < 1.60, therefore demonstrating a good correlation between the tomographic and the planar imaging parameters. Another parameter, the regional 123I-mIBG rWO, calculated on SPECT imaging, was considered in one of these studies. It was calculated by subtracting the minimum rWO among 17 segments. The abnormal rWO was defined as both the rWO range and maximum rWO > mean value + 2SD obtained in 15 subjects.39 This SPECT parameter was significantly associated with SCD. An increased rWO, according to Doi et al.,,40 is associated with cardiac events in patients with chronic HF, suggesting a good prognostic value of this parameter.
Nevertheless, controversies remain on whether the best parameter to assess such risks remains the H/M on planar images. Indeed, most of the authors recognize as a major limitation to their studies the low sample size and the fact that additional studies are needed to establish the role of 123I-mIBG SPECT. Furthermore, the population of patients was heterogeneous since it doesn’t discriminate the etiology of chronic HF between ischemic and non-ischemic.13 A recent study41 assembling SPECT slices in polar maps of 20 instead of 17 segments was included in this review,42 having similar outcomes in terms of SPECT SDS in correlation with prognosis in patients with chronic HF.43 Several studies tried to apply 123I-mIBG SPECT in different ways. Somsen et al.44 described a new method to quantitative myocardial mIBG uptake, considering eighteen 123I-mIBG SPECT studies of patients with chronic HF. Myocardial uptake is calculated from the myocardial to left ventricular cavity count density ratio and the 123I activity in a blood sample. This was performed employing single-slice SPECT and multi-slice SPECT methods. The first compares different ROIs: mediastinum (M), right lung (L), left ventricular cavity (C), and the entire myocardium (MYO). The second analyzes semi-automatically drawn volumes of interest (VOIs). The single-slice SPECT method showed poor reproducibility than the multi-slice SPECT method that is a reproducible and accurate technique for the assessment of myocardial 123I-mIBG uptake but further evaluations of this method are needed.45,46,47,–48 Another study49 examined the association between left ventricular mechanical dyssynchrony and cardiac sympathetic denervation with potential SCD events in the ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) trial. The ADMIRE-HF subject had rest gated SPECT Technetium-99 metastable (99mTc)-Tetrofosmin and 123I-mIBG imaging. Thanks to SPECT myocardial perfusion imaging, it was possible to determine the phase standard deviation, an index of mechanical dyssynchrony, through which it was observed an association between left ventricular mechanical dyssynchrony and SCD events in symptomatic patients with HF and reduced EF.
Conclusions
Data from this systematic review suggest that patients affected by chronic HF, including those receiving an ICD, with a high SPECT SDS, an increased rWO, or, either way, reduced tracer uptake in specific segments of the myocardium, have an increased risk of developing AE or SCD, with a worse prognosis with respect to patients with a low SDS. In any case, it seems clear that additional studies must be performed and an automated quantitative analysis system must be adopted for 123I-mIBG SPECT since the lack of standardized methods makes the comparison difficult between different studies and the sharing of data between different centers, to reach the same reliable prognostic value as planar 123I-mIBG scintigraphy.
Abbreviations
- HF:
-
Heart failure
- 123I-mIBG:
-
Iodine123-metaiodobenzylguanidine
- H/M:
-
Heart to mediastinum ratio
- WR:
-
Wash-out rate
- SPECT:
-
Single-photon emission computerized tomography
- AE:
-
Arrhythmic events
- SCD:
-
Sudden cardiac death
- OS:
-
Overall survival
- MPI:
-
Myocardial perfusion imaging
- rWO:
-
Regional wash-out rate
References
Treglia G, Stefanelli A, Bruno I, Giordano A. Clinical usefulness of myocardial innervation imaging using Iodine-123-meta-iodobenzylguanidine scintigraphy in evaluating the effectiveness of pharmacological treatments in patients with heart failure: an overview. Eur Rev Med Pharmacol Sci. 2013;17:56–68.
Kasama S, Toyama T, Kurabayashi M. Usefulness of cardiac sympathetic nerve imaging using (123)Iodine-metaiodobenzylguanidine scintigraphy for predicting sudden cardiac death in patients with heart failure. Int Heart J. 2016;57:140–4.
Flotats A. Role of myocardial 123I-mIBG innervation imaging in the diagnosis of neurodegenerative diseases. Clin Transl Imaging. 2018;6:449–58.
Werner RA. Cardiac innervation imaging as a risk stratification tool for potential device therapy candidates. J Nucl Cardiol. 2020;27:1798–801.
Dimitriu-Leen AC, Scholte AJ, Jacobson AF. 123I-MIBG SPECT for evaluation of patients with heart failure. J Nucl Med. 2015;56:25s–30s.
Asghar O, Arumugam P, Armstrong I, Ray S, Schmitt M, Malik RA. Iodine-123 metaiodobenzylguanidine scintigraphy for the assessment of cardiac sympathetic innervation and the relationship with cardiac autonomic function in healthy adults using standardized methods. Nucl Med Commun. 2017;38:44–50.
Shibutani T, Nakajima K, Yoneyama H, Konishi T, Okuda K, Onoguchi M, et al. The utility of heart-to-mediastinum ratio using a planar image created from IQ-SPECT with Iodine-123 meta-iodobenzylguanidine. J Nucl Cardiol. 2020. https://doi.org/10.1007/s12350-020-02081-9.
Jacobson AF, Lombard J, Banerjee G, Camici PG. 123I-mIBG scintigraphy to predict risk for adverse cardiac outcomes in heart failure patients: design of two prospective multicenter international trials. J Nucl Cardiol. 2009;16:113–21.
Nakata T, Nakajima K, Yamashina S, Yamada T, Momose M, Kasama S, et al. A pooled analysis of multicenter cohort studies of (123)I-mIBG imaging of sympathetic innervation for assessment of long-term prognosis in heart failure. JACC Cardiovasc Imaging. 2013;6:772–84.
Bax JJ, Kraft O, Buxton AE, Fjeld JG, Parízek P, Agostini D, et al. 123 I-mIBG scintigraphy to predict inducibility of ventricular arrhythmias on cardiac electrophysiology testing: a prospective multicenter pilot study. Circ Cardiovasc Imaging. 2008;1:131–40.
Nakajima K, Nakata T. Cardiac 123I-MIBG imaging for clinical decision making: 22-year experience in Japan. J Nucl Med. 2015;56:11s–9s.
Iqbal B, Currie G, Kiat H. Regional cardiac sympathetic nervous system evaluation using 123I-mIBG SPECT in patients with heart failure. J Med Imaging Radiat Sci. 2018;49:397–405.
De Vincentis G, Frantellizzi V, Fedele F, Farcomeni A, Scarparo P, Salvi N, et al. Role of cardiac 123I-mIBG imaging in predicting arrhythmic events in stable chronic heart failure patients with an ICD. J Nucl Cardiol. 2018;26:1188–96.
Verberne HJ. Assessment of cardiac sympathetic innervation with (123)I-mIBG SPECT comes to life: need for standardization! Eur Heart J Cardiovasc Imaging. 2016;17:391–2.
Carrió I, Cowie MR, Yamazaki J, Udelson J, Camici PG. Cardiac sympathetic imaging with mIBG in heart failure. JACC Cardiovasc Imaging. 2010;3:92–100.
Verschure DO, Poel E, Nakajima K, Okuda K, van Eck-Smit BLF, Somsen GA, et al. A European myocardial (123)I-mIBG cross-calibration phantom study. J Nucl Cardiol. 2018;25:1191–7.
Al Badarin FJ, Wimmer AP, Kennedy KF, Jacobson AF, Bateman TM. The utility of ADMIRE-HF risk score in predicting serious arrhythmic events in heart failure patients: incremental prognostic benefit of cardiac 123I-mIBG scintigraphy. J Nucl Cardiol 2014;21:756-62; quiz 3-55, 63-5.
Siebermair J, Lehner S, Sattler SM, Rizas KD, Beckmann BM, Becker A, et al. Left-ventricular innervation assessed by (123)I-SPECT/CT is associated with cardiac events in inherited arrhythmia syndromes. Int J Cardiol. 2020;312:129–35.
Wan N, Travin MI. Cardiac imaging with (123)I-meta-iodobenzylguanidine and analogous PET tracers: current status and future perspectives. Semin Nucl Med. 2020;50:331–48.
Tokuda Y, Sakakibara M, Yoshinaga K, Yamada S, Kamiya K, Asakawa N, et al. Early therapeutic effects of adaptive servo-ventilation on cardiac sympathetic nervous function in patients with heart failure evaluated using a combination of (11)C-HED PET and (123)I-MIBG SPECT. J Nucl Cardiol. 2019;26:1079–89.
Kawai T, Yamada T, Tamaki S, Morita T, Furukawa Y, Iwasaki Y, et al. Usefulness of cardiac meta-iodobenzylguanidine imaging to identify patients with chronic heart failure and left ventricular ejection fraction <35% at low risk for sudden cardiac death. Am J Cardiol. 2015;115:1549–54.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6:e1000100.
Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol. 2003;3:25.
Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155:529–36.
Schueler S, Schuetz GM, Dewey M. The revised QUADAS-2 tool. Ann Intern Med 2012;156:323; author reply -4.
Jacobson AF, Senior R, Cerqueira MD, Wong ND, Thomas GS, Lopez VA, et al. Myocardial iodine-123 meta-iodobenzylguanidine imaging and cardiac events in heart failure. Results of the prospective ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) study. J Am Coll Cardiol. 2010;55:2212–21.
Verberne HJ, Brewster LM, Somsen GA, van Eck-Smit BL. Prognostic value of myocardial 123I-metaiodobenzylguanidine (MIBG) parameters in patients with heart failure: a systematic review. Eur Heart J. 2008;29:1147–59.
Travin MI, Henzlova MJ, van Eck-Smit BLF, Jain D, Carrió I, Folks RD, et al. Assessment of 123I-mIBG and 99mTc-tetrofosmin single-photon emission computed tomographic images for the prediction of arrhythmic events in patients with ischemic heart failure: Intermediate severity innervation defects are associated with higher arrhythmic risk. J Nucl Cardiol. 2016;24:377–91.
Christensen TE, Kjaer A, Hasbak P. The clinical value of cardiac sympathetic imaging in heart failure. Clin Physiol Funct Imaging. 2013;34:178–82.
van der Veen BJ, Al Younis I, de Roos A, Stokkel MP. Assessment of global cardiac I-123 MIBG uptake and washout using volumetric quantification of SPECT acquisitions. J Nucl Cardiol. 2012;19:752–62.
Verschure DO, de Groot JR, Mirzaei S, Gheysens O, Nakajima K, van Eck-Smit BLF, et al. Cardiac 123 I- m IBG scintigraphy is associated with freedom of appropriate ICD therapy in stable chronic heart failure patients. Int J Cardiol. 2017;248:403–8.
Dimitriu-Leen AC, Gimelli A, Al Younis I, Veltman CE, Verberne HJ, Wolterbeek R, et al. The impact of acquisition time of planar cardiac (123)I-MIBG imaging on the late heart to mediastinum ratio. Eur J Nucl Med Mol Imaging. 2016;43:326–32.
Teresińska A. Iodine-123-metaiodobenzylguanidine cardiac SPECT imaging in the qualification of heart failure patients for ICD implantation. J Nucl Cardiol. 2019;26:1182–7.
Boogers MJ, Borleffs CJ, Henneman MM, van Bommel RJ, van Ramshorst J, Boersma E, et al. Cardiac sympathetic denervation assessed with 123-iodine metaiodobenzylguanidine imaging predicts ventricular arrhythmias in implantable cardioverter-defibrillator patients. J Am Coll Cardiol. 2010;55:2769–77.
Marshall A, Cheetham A, George RS, Mason M, Kelion AD. Cardiac iodine-123 metaiodobenzylguanidine imaging predicts ventricular arrhythmia in heart failure patients receiving an implantable cardioverter-defibrillator for primary prevention. Heart. 2012;98:1359–65.
Clements IP, Kelkar AA, Garcia EV, Butler J, Chen J, Folks R, et al. Prognostic significance of123I-mIBG SPECT myocardial imaging in heart failure: differences between patients with ischaemic and non-ischaemic heart failure. Eur Heart J Cardiovasc Imaging. 2015;17:384–90.
Tinti E, Positano V, Giorgetti A, Marzullo P. Feasibility of [(123)I]-meta-iodobenzylguanidine dynamic 3-D kinetic analysis in vivo using a CZT ultrafast camera: preliminary results. Eur J Nucl Med Mol Imaging. 2014;41:167–73.
Kasama S, Toyama T, Sumino H, Nakazawa M, Matsumoto N, Sato Y, et al. Prognostic value of serial cardiac 123I-MIBG imaging in patients with stabilized chronic heart failure and reduced left ventricular ejection fraction. J Nucl Med. 2008;49:907–14.
Yamamoto H, Yamada T, Tamaki S, Morita T, Furukawa Y, Iwasaki Y, et al. Prediction of sudden cardiac death in patients with chronic heart failure by regional washout rate in cardiac MIBG SPECT imaging. J Nucl Cardiol. 2019;26:109–17.
Doi T, Nakata T, Hashimoto A, Yuda S, Wakabayashi T, Kouzu H, et al. Cardiac mortality assessment improved by evaluation of cardiac sympathetic nerve activity in combination with hemoglobin and kidney function in chronic heart failure patients. J Nucl Med. 2012;53:731–40.
Sazonova SI, Atabekov TA, Batalov RE, Mishkina AI, Varlamova JV, Zavadovsky KV, et al. Prediction of appropriate ICD therapy in patients with ischemic heart failure. J Nucl Cardiol. 2020. https://doi.org/10.1007/s12350-020-02321-y.
Slomka PJ, Nishina H, Berman DS, Kang X, Friedman JD, Hayes SW, et al. Automatic quantification of myocardial perfusion stress-rest change: a new measure of ischemia. J Nucl Med. 2004;45:183–91.
Mangieri E, Tanzilli G, De Vincentis G, Barillà F, Remediani S, Acconcia MC, et al. Slow coronary flow and stress myocardial perfusion imaging. Different patterns in acute patients. J Cardiovasc Med (Hagerstown). 2006;7:322–7.
Somsen GA, Borm JJ, de Milliano PA, van Vlies B, Dubois EA, van Royen EA. Quantitation of myocardial iodine-123 MIBG uptake in SPET studies: a new approach using the left ventricular cavity and a blood sample as a reference. Eur J Nucl Med. 1995;22:1149–54.
Nakajima K, Okuda K, Yokoyama K, Yoneyama T, Tsuji S, Oda H, et al. Cross calibration of (123)I-meta-iodobenzylguanidine heart-to-mediastinum ratio with D-SPECT planogram and Anger camera. Ann Nucl Med. 2017;31:605–15.
Nakajima K, Verschure DO, Okuda K, Verberne HJ. Standardization of (123)I-meta-iodobenzylguanidine myocardial sympathetic activity imaging: phantom calibration and clinical applications. Clin Transl Imaging. 2017;5:255–63.
Verberne HJ, Feenstra C, de Jong WM, Somsen GA, van Eck-Smit BLF, Busemann Sokole E. Influence of collimator choice and simulated clinical conditions on 123I-MIBG heart/mediastinum ratios: a phantom study. European journal of nuclear medicine and molecular imaging. 2005;32:1100–7.
Flotats A, Carrio I, Agostini D, Le Guludec D, Marcassa C, Schafers M, et al. Proposal for standardization of 123I-metaiodobenzylguanidine (MIBG) cardiac sympathetic imaging by the EANM Cardiovascular Committee and the European Council of Nuclear Cardiology. Eur J Nucl Med Mol Imaging. 2010;37:1802–12.
Hage FG, Aggarwal H, Patel K, Chen J, Jacobson AF, Heo J, et al. The relationship of left ventricular mechanical dyssynchrony and cardiac sympathetic denervation to potential sudden cardiac death events in systolic heart failure. J Nucl Cardiol. 2014;21:78–85.
Disclosures
Mariano Pontico, Gabriele Brunotti, Miriam Conte, Ferdinando Corica, Laura Cosma, Cristina De Angelis, Maria Silvia De Feo, Julia Lazri, Antonio Matto, Melissa Montebello, Arianna Di Rocco, Viviana Frantellizzi, Alessio Farcomeni, and Giuseppe De Vincentis have no conflicts of interest to declare.
Funding
Open Access funding provided by Università degli Studi di Roma La Sapienza. No funding has been received for this paper.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The authors of this article have provided a PowerPoint file, available for download at SpringerLink, which summarises the contents of the paper and is free for re-use at meetings and presentations. Search for the article DOI on SpringerLink.com.
The authors have also provided an audio summary of the article, which is available to download as ESM, or to listen to via the JNC/ASNC Podcast.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pontico, M., Brunotti, G., Conte, M. et al. The prognostic value of 123I-mIBG SPECT cardiac imaging in heart failure patients: a systematic review. J. Nucl. Cardiol. 29, 1799–1809 (2022). https://doi.org/10.1007/s12350-020-02501-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-020-02501-w