
Abstract
Background
Despite therapeutic improvement, the prognosis of chronic heart failure (CHF) remains unfavorable partly due to arrhythmia and sudden cardiac death (SCD). This prospective study evaluated myocardial 123I-meta-iodobenzylguanidine (123I-mIBG) scintigraphy as a predictor of arrhythmic events (AE) in CHF patients.
Methods
170 CHF patients referred for implantable cardioverter-defibrillator (ICD) implantation for both primary and secondary prevention were enrolled. All patients underwent planar and SPECT imaging. Early and late heart-to-mediastinum (H/M) ratio, 123I-mIBG washout (WO), early and late summed SPECT scores were calculated The primary endpoint was an AE: sustained ventricular tachycardia, resuscitated cardiac arrest, appropriate ICD therapy or SCD. The secondary endpoint was appropriate ICD therapy.
Results
During a median follow-up of 23.3 months, 69 patients experienced an AE. Early summed score (ESS) was the only independent predictor of AE [HR 1.023 (1.003-1.043)]. Focussing on only patients with an ICD for primary prevention, ESS was the only independent predictor of AE [HR 1.028 (1.007-1.050)]. 123I-mIBG-derived parameters failed to be independent predictors of appropriate ICD therapy. However there was a “bell-shaped” relation between 123I-mIBG scintigraphy-derived parameters and AE and appropriate ICD therapy, i.e., those with intermediate 123I-mIBG abnormalities tended to be at higher risk of events.
Conclusion
Although SPECT 123I-mIBG scintigraphy was associated with AE in CHF patients with ICD implantation for primary and secondary prevention, no association was found between 123I-mIBG scintigraphy-derived parameters and appropriate ICD therapy.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Chronic heart failure (CHF) is a life-threatening syndrome with a growing incidence and prevalence over the last decades, with consequently high hospitalization and re-hospitalization rates. CHF is associated with high morbidity and mortality rates and approximately 50% of deaths are related to sudden cardiac death (SCD). In addition, mortality rates increase with increased disease duration, i.e., 20% during the first year and rising to approximately 50% within 5 years.1
In order to prevent SCD in CHF patients, current guidelines recommend an implantable cardioverter-defibrillator (ICD) in those patients with a left ventricular ejection fraction (LVEF) < 35%, NYHA class II or III and treated with optimal medical therapy. Initial trials showed that ICD’s are effective in reducing SCD in CHF patients.2 However, recent studies suggest that several ICD recipients experience inappropriate shocks and ICD-associated infectious complications.3,4,5 Furthermore, some arrhythmic deaths happen in patients who were classified as low risk for arrhythmic cardiac death and had no ICD indication. In addition, for example, in the SCD-HeFT (Sudden Cardiac Death in Heart Failure Trial) study three years after ICD implantation for primary prevention, a remarkably high percentage (65%) of patients had never received appropriate ICD therapy.6 Taken together, these issues suggest that the current ICD selection criteria in CHF patients, now largely driven by LVEF, are suboptimal.
The cardiac sympathetic activity is one of the neurohormonal compensation mechanisms that plays an important role in the pathogenesis and prognosis of CHF with impaired LVEF. Initially, beta-adrenergic receptor stimulation by increased synaptic norepinephrine (NE) levels helps to compensate for impaired myocardial function, but long-term NE excess has detrimental effects on myocardial structure and gives rise to a downregulation and decrease in the sensitivity of post-synaptic β-adrenergic receptor and consequently, poor outcome.7
Cardiac sympathetic activity can non-invasively be assessed with meta-iodobenzylguanidine (123I-mIBG) using both planar and SPECT techniques.8123I-mIBG is a radiolabeled NE analogue and accumulates in the presynaptic myocardial sympathetic nerve endings. Quantified myocardial 123I-mIBG parameters have proved to be of prognostic value in CHF.9,10,11,12 Those patients with impaired myocardial 123I-mIBG parameters had a worse prognosis compared with those with relatively preserved parameters (i.e., reduced late heart-to-mediastinum (H/M) ratio and increased 123I-mIBG myocardial washout (WO)).
More specifically, Boogers et al. demonstrated that high values of the SPECT-derived summed myocardial denervation score, (i.e., extensively reduced activity of the norepinephrine transporter was associated with an increased risk of ventricular arrhythmia related to appropriate ICD therapy and SCD.10 However, the study population consisted of a heterogeneous failure population with an ICD for both primary and secondary prevention.
The primary goal of our study was to evaluate the efficacy of both planar and SPECT 123I-mIBG imaging to predict AE, defined as an episode of sustained ventricular tachycardia, resuscitated cardiac arrest, appropriate ICD discharge (anti-tachycardial pacing or defibrillation), or SCD. In addition, we studied whether 123I-mIBG scintigraphy could predict appropriate ICD therapy specifically (i.e., secondary endpoint).
Materials and Methods
We performed a prospective, single-center observational study of CHF patients with an indication for ICD implantation as for both primary and secondary prevention. From October 2011 to January 2016, consecutive CHF patients, fulfilling the inclusion criteria, were prospectively enrolled.
Inclusion criteria were NYHA class II or III; LVEF < 35%; indication for an ICD implantation (primary or secondary prevention); expected survival > 1 years; age > 18 years old; signed informed consent. All patients received optimal medical therapy according to current guidelines.13 Exclusion criteria were previous ICD implantation; cardiac resynchronisation therapy (CRT) indication; cancer history; severe valvulopathy; recent acute coronary syndrome (< 3 months); contraindication to ICD implantation.
Enrolled patients underwent 123I-mIBG scintigraphy 7-15 days before ICD implantation. Settings for detection of ventricular tachycardia’s or fibrillation were at the discretion of the implanting physician.
Clinical follow-up with ICD interrogation was performed at 6, 12, and 18 months. AE were defined as episodes of sustained ventricular tachycardia (> 30 seconds), resuscitated cardiac arrest, appropriate ICD intervention (anti-tachycardial pacing or defibrillation), or SCD.
Written informed consent was obtained from all patients. The study protocol was approved by the institutional committee on human research and conducted in accordance with the ethical guidelines of the 1975 Helsinki Declaration.
Image Acquisition of Planar and SPECT 123I-mIBG Scintigraphy
A 5% Lugol solution was administered to block the thyroid before the administration of 150-185 MBq of 123I-mIBG (AdreView, GE Healthcare), resulting in an effective dose of 2.5 to 3.3 mSv.
Fifteen (i.e., early) and 240 (i.e., late) minutes after tracer injection, planar anterior thoracic images were acquired for 10 minutes with a zoom factor of 1 and stored in a 128 × 128 matrix. The images were acquired in supine position, with a dual-head gamma camera (Infinia, GE Healthcare, Milwaukee, USA) using a low energy parallel-hole high-resolution collimator (LEHR).
Immediately after the planar images, at 25 minutes and 250 minutes after injection, SPECT cardiac images were acquired with the dual-headed gamma camera over 180° using a 90°-rotation, starting at 45° right-anterior oblique projection and proceeding to the 45° left-posterior oblique projection. A 64 × 64 matrix was used for the SPECT studies (zoom factor 1). We applied a step-and-shot technique (64 projections, 30 seconds of duration per frame in non-gated mode). For both planar and SPECT, the energy window was symmetrically centered to ± 10% of the 159-KeV 123I photopeak.
Planar 123I-mIBG Scintigraphy Analysis
Planar 123I-mIBG images were analyzed to obtain semi-quantitative parameters of tracer distribution. On the planar images, a manually polygonal region of interest (ROI) was drawn over the heart, around the epicardial border and the valve plane, including the left ventricular cavity (H), being careful to exclude lung and liver from the myocardial ROI.14 A second 7 × 7 pixel square ROI was placed on the upper half of the mediastinum (M), below the thyroid gland. H/M ratio’s, at 15 minutes (early H/M ratio) and 240 minutes (late H/M ratio), were calculated as mean counts per pixel in the myocardial ROI divided by the mean counts per pixel in the mediastinal ROI.14
The myocardial washout rate (WO) from early to late images was calculated using background correction according to the following formula and expressed as a percentage:14
where 1.21 is the correction for 123I decay at 3 hours and 45 minutes; e the early images; l the late images; H the heart counts per pixel; and M is the mediastinal counts per pixel.
SPECT 123I-mIBG Scintigraphy Analysis
Using Myovaton software implemented on a Xeleris Duo platform (GE Healthcare), SPECT images were reoriented in short, vertical long, and horizontal long heart axes after filtered-back-projection (FBP) reconstruction. A low-pass filter, Butterworth (order: 10, cut-off frequency: 0.3 cycles/cm for early SPECT and order: 20, cut-off frequency: 0.3 cycles/cm for late SPECT) was used as a preprocessing filter; no scatter or attenuation correction was applied (Figure 1). After reorientation of myocardial axes, heart images were analyzed with a standard 17-segments model similarly to the conventional methods used for myocardial perfusion imaging (MPI).15,16 All 17 segments were visually scored by each reader using a 5-point scale where myocardial 123I-mIBG uptake was expressed as a percentage of the maximum myocardial uptake17: segments with a value greater than 70% were defined as normal and scored as 0. Segments with mildly reduced uptake, ranging from 69 to 60%, were scored as 1. A score of 2 was assigned to segments with moderately reduced uptake, 59-50%. Segments with severely reduced uptake, 49-40%, were scored as 3. Finally, segments with absent uptake (i.e., lower than 39%) were scored as 4. The defect scores were calculated as the sum of the segmental scores and the early and late summed scores (ESS and LSS, respectively) were obtained. The difference summed score (DSS) was obtained as the subtraction between ESS and LSS.

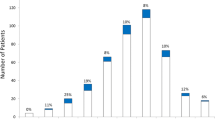
(A) Relation between late H/M ratio categories and arrhythmic events (AE). (B) Relation between late H/M ratio categories and appropriate ICD therapy. Due to a relatively low number of patients with late H/M ratio < 1.2 (n = 8) compared to those with late H/M ratio > 1.6 (n = 51) and intermediate late H/M ratio (n = 111), no adequate statistical analysis was feasible to compare the three groups. Therefore, we combined the groups with late H/M ratio < 1.2 and > 1.6 and compared this combined group with those with an intermediate late H/M ratio (1.2–1.6): P = .014 for AE and P < .001 for ICD therapy
Observer Variability of SPECT 123I-mIBG Images
For the inter-observer analysis, three observers with different degrees of expertise in nuclear cardiology techniques, independently reviewed all SPECT 123I-mIBG images.
Statistical Analysis
Data are expressed as means ± standard deviation, differences between groups (those with AE and those without AE) were evaluated with the independent samples T-test, the Mann-Whitney U test, or χ2 when appropriate. Incidence of events was estimated by means of Kaplan-Meier curves, and univariate or multivariable Cox regression models were used to assess (adjusted) hazard ratios. Proportionality of hazards was checked by means of residual analysis. Time-dependent ROC curves from censored data were computed using the Kaplan-Meier method.18,19 In order to assess reproducibility among three operators, the intra-class correlation coefficient (ICC) was used. For clinically relevant agreement, the following criteria were used: ICC values < .40, .40-.59, .60-.74, .75-1.00 were considered poor, fair, good, excellent, respectively.
A P value < .05 was considered to indicate a statistical significance. All analyses were conducted with R software version 3.0.2 (R Development Core Team, 2013).
Results
Subjects
A total of 170 consecutive patients (139 male, mean age 64.2 ± 12.6 years) were enrolled. The baseline characteristics are shown in Table 1. Almost 60% of the patients had ischemic heart disease. Eighty-six patients (50.6%) were classified as NYHA class II and 84 (49.4%) as NYHA class III. The mean LVEF was 31.1 ± 9.4%. Approximately 25% of the patients had a left bundle branch block (LBBB). The majority of patients (n = 156) received an ICD for primary prevention. The mean early H/M ratio was 1.62 ± .21, the late H/M ratio was 1.53 ± .23, and 123I-mIBG WO was 30.9 ± 18.4%. The mean early SPECT summed score (ESS) was 31.4 ± 11.9, the mean late SPECT score (LSS) was 36.2 ± 12.3, and the SPECT difference score (DSS) (i.e., ESS - LSS) was − 4.7 ± 8.6.
Arrhythmic Events
Follow-up was complete in all patients with a median follow-up of 23.3 (1-51) months. In total, 69 patients experienced an AE. Of these 25 had sustained ventricular tachycardia (> 30 seconds), 3 of whom had a spontaneous reconversion to sinus rhythm, 22 experienced an appropriate ICD therapy (anti-tachycardial pacing or defibrillation), 8 had a resuscitated cardiac arrest, and 14 died of SCD. Patients with AE tended to have a lower, but not significant late H/M ratio (P = .074), higher myocardial 123I-mIBG washout (P = .020) , and higher ESS and LSS (respectively, P = .012 and P= .040).
In the overall population (i.e., primary and secondary prevention), the late H/M ratio showed in relation to AE a “bell-shaped” curve (Figure 1A). A similar curve was found for late H/M ratio in relation to appropriate ICD therapy (Figure 1B). Patients with intermediate late H/M ratios (range 1.2-1.6) were more likely to have an AE and appropriate ICD therapy compared to patients with low and high late H/M ratios. A similar pattern was observed for the primary prevention group only (data not shown)
SPECT 123I-mIBG Observer Variability
The ICC for inter-observer variability of the summed 123I-mIBG SPECT scores showed an excellent agreement for both ESS and LSS (.846, 95% CI: .801-.884, P < .001 and .829, 95% CI: .786-.866, P < .001, respectively).
Independent Predictors of Arrhythmic Events
The results of the multivariate Cox regression analysis are shown in Table 2. ESS was the only independent predictor of AE in both primary and secondary prevention [HR 1.023 (1.003-1.043), P = .023]. Focussing on only patients with an ICD for primary prevention, the ESS was the only independent predictor of the combined AE [HR 1.028 (1.007-1.050), P = .009]. Due to the relative low number of patients with a secondary ICD indication, no subgroup analysis was performed for this subgroup.
When we analyzed the separate AE classifications in the combined group of primary and secondary ICD indication, age was the only independent predictor appropriate ICD therapy [HR .971 (.944-.999), P = .040]. For combined primary and secondary prevention, late H/M ratio failed to be an independent predictor of appropriate ICD therapy [HR .153 (.020-1.172), P = .071]. In addition, the late H/M ratio also failed as an independent predictor of appropriate ICD therapy in the primary prevention group only. Both the ESS and the LVEF were independent predictors of SCD [respectively, HR 1.048 (1.000-1.098), P = .050 and HR .924 (.855-.998), P = .045].
Discussion
CHF is associated with high morbidity and mortality rates. Despite optimal medical therapy, arrhythmia and SCD occur frequently in this population. In the past decades, ICD implantation has become an integral component of CHF management.13 Although the efficacy of ICD implantation has been proven in many multicenter studies, questions have been raised if patients selection is adequate. Even though LVEF < 35% is most commonly used for risk stratification for ventricular arrhythmias, it does not adequately identify patients at risk for SCD. In the MADIT II population, only 35% of the patients received appropriate ICD therapy during 3-year follow-up.6
The present study demonstrates that in stable CHF patients with ICD implantation for both primary and secondary prevention, ESS was the only SPECT 123I-mIBG scintigraphy-derived parameter associated with AE. The planar-derived parameters (i.e., early and late H/M ratios and 123I-mIBG WO) were not able to predict AE. Furthermore, both planar- and SPECT-derived parameters were not able to predict appropriate ICD therapy. These findings are line with a recent multicenter study including 135 CHF patients with ICD implantation for primary prevention.20
Previous large multicentre study and meta-analysis have suggested linear correlations between overall prognosis (i.e., progression CHF, cardiac death) and increased cardiac sympathetic activity, expect for AE and appropriated ICD therapy.9,21 However, there are some small studies suggesting an association between increase cardiac sympathetic activity and AE of appropriate ICD therapy. In a prospective study in 116 CHF patients, eligible for ICD implantation for both primary and secondary prevention of SCD, 123I-mIBG SPECT was shown to be an independent predictor of appropriate ICD therapy and cardiac death.10 The cumulative incidence of appropriate ICD therapy during 3-year follow-up was significantly higher when a relatively large 123I-mIBG SPECT defect (median summed score ≥26) was present. In a small study by Marshall et al22 including 27 CHF patients referred for ICD implantation with or without CRT, patients with AE, SCD had lower H/M ratios and higher 123I-mIBG SPECT defect score compared to those without an event.
A possible explanation for the difference in 123I-mIBG scintigraphy outcome in relation to appropriate ICD therapy between present study and previous studies10,22 could be related to differences in patient selection (i.e., ICD implantation for combined primary and secondary prevention), aetiology of CHF (i.e., ischemic vs. non-ischemic), differences in ICD settings, CRT, and number of patients with optimal medical therapy. More specifically the percentage of patients in the present study receiving ACE-inhibition (ACE-I) or angiotensin receptor blocker (ARB) was relatively low compared to other study cohorts.
The “bell-shaped” relation between 123I-mIBG and events is not new. For example, the results of the recent study by Verschure et al20 showed a “bell-shaped” curve for the early and late H/M ratio in relation to appropriated ICD therapy, suggesting that patients with intermediate late H/M ratio are more likely to have appropriate ICD therapy compared to patients with low and high late H/M ratios. Our findings are also in line with previous findings of Agostini et al showing that AE occurred in patients with an intermediate standardized late H/M ratio (1.46-2.17). In addition, Travin et al demonstrated similar results for 123I-mIBG SPECT defects in a population with 471 ischemic CHF patients, showing that, those with intermediate defects on 123I-mIBG SPECT summed score appeared to be at the highest risk for cardiac events.23 They concluded that the presumption of a monotonic increase in risk of an AE with increasing 123I-mIBG SPECT defects may not be correct. In line with these previous studies, the present study showed the same “bell-shaped” curve for late H/M ratio (Figure 1). For the SPECT-derived parameters similar curves were seen (data not shown). This underlines the notion that most likely there is no linear association between risk of an AE and 123I-mIBG myocardial uptake.
Although the exact pathophysiology of arrhythmias is still a matter of debate, it has been recognized that scar tissue and ischemia may serve as substrate for arrhythmias. Areas with slow conduction may facilitate the development of reentrant tachycardia.24 Especially the border zone of infarct tissue with viable myocardial tissue is predisposed to develop reentrant circuits. Sympathetic nerve fibers are more susceptible to ischemia than myocytes, thereby causing a disbalance between still viable but partly denervated and normal myocardium.25 This disbalance in myocardial sympathetic innervation may create a myocardial substrate particularly vulnerable to arrhythmia and arrhythmic death. The results of the present study with the “bell-shaped” curve for the late H/M ratio in relation to appropriated ICD therapy underline this hypothesis.
Recently the DANISH trail, reported that the ICD implantation for primary prevention of SCD in non-ischemic heart failure was not associated with improved survival compared with usual clinical care.26 However, SCD occurred less often in the ICD group compared to the control group [HR .50 (.31-.82), P = .005]. This suggests that some non-ischemic CHF patients remain at an increased risk for SCD. Future studies will be needed to confirm whether myocardial 123I-mIBG scintigraphy is helpful in specifically identifying non-ischemic CHF patients with an increased SCD risk.
123I-mIBG scintigraphy is a highly reproducible technique to assess cardiac sympathetic activity and has a small inter- and intra-observer variation.27 The analysis of 123I-mIBG SPECT can be challenging in patients with impaired myocardial 123I-mIBG uptake, i.e., discrimination between myocardium (low/no uptake) and lung (higher uptake) might be difficult. Although this difficulty might possibly interfere with the reading of the images, the present study showed a low variability in SPECT score between the 3 observers. This indicates that with visual scoring, observers are able to adequately overcome possible variation in a uniform way. In addition, the results of the present study are in line with previous studies showing a relatively small inter-observer variability.27,28
Despite the fact that 123I-mIBG scintigraphy is highly reproducible, there are many inter-institutional differences in image acquisition and post-processing. Therefore, international efforts have been made to harmonize and standardize cardiac 123I-mIBG scintigraphy.14 These recommendations include proposals for patient preparation, administered dose of 123I-mIBG activity (MBq), scanning parameters, and analysis of the acquired data to obtain the most used semi-quantitative parameters (i.e., early and late H/M ratio and 123I-mIBG washout (WO)). In addition, it has been suggested to correct for different collimator use and use standardized planar-derived parameters.29 This will further the clinical role of myocardial 123I-mIBG scintigraphy.
Study Limitations
Although the included patients were treated with optimal medical therapy, the percentage of subject receiving ACE-inhibition/angiotensin receptor blocker was relatively low compared to other studies. This could have influenced the cardiac sympathetic activity in these patients and consequently the outcome of this study. Furthermore, the CHF aetiology of the enrolled patients was heterogeneous including both ischemic and non-ischemic HF. Therefore, additional studies are needed to establish the specific role of 123I-mIBG imaging in these specific subpopulations.
Although we did not perform myocardial perfusion imaging, this could have generated additional information on regional innervation/perfusion mismatch areas that might predispose to ventricular arrhythmias.22,30 Finally, although a ME collimator is recommended, in the present study a LEHR collimator was used. To overcome the difference in collimator use and to extrapolate these results to other institutions, standardized planar-derived parameters should be used.29
Conclusion
In conclusion, SPECT 123I-mIBG scintigraphy-derived ESS was associated with AE in patients with ICD implantation for primary and secondary prevention. Although no linear association was found between 123I-mIBG scintigraphy-derived parameters and appropriate ICD therapy, there was a “bell-shaped” relation between 123I-mIBG scintigraphy-derived parameters and AE and appropriate ICD therapy. This seemingly counterintuitive finding implies that not those with the largest 123I-mIBG abnormalities tend to be at the highest risk for events but those with intermediate 123I-mIBG abnormalities.
New Knowledge Gained
The present study showed a “bell-shaped” relation between cardiac sympathetic activity and AE and appropriated ICD therapy. These findings are in line with previous studies and underline the change in paradigm that not those with the largest 123I-mIBG abnormalities tend to be at the highest risk for events but those with intermediate 123I-mIBG abnormalities.
Abbreviations
- 123I-mIBG:
-
123I-meta-iodobenzylguanidine
- AE:
-
Arrhythmic events
- CHF:
-
Chronic heart failure
- DSS:
-
Difference summed score
- ESS:
-
Early summed score
- H/M ratio:
-
Heart-to-mediastinum ratio
- LSS:
-
Late summed score
- LVEF:
-
Left ventricular ejection fraction
- SCD:
-
Sudden cardiac death
- WO:
-
Washout
References
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:e147–239.
Borne RT, Peterson PN, Greenlee R, Heidenreich PA, Wang Y, Curtis JP, et al. Temporal trends in patient characteristics and outcomes among Medicare beneficiaries undergoing primary prevention implantable cardioverter-defibrillator placement in the United States, 2006-2010. Results from the National Cardiovascular Data Registry’s Implantable Cardioverter-Defibrillator Registry. Circulation. 2014;130:845–53.
Bhavnani SP, Giedrimiene D, Coleman CI, Guertin D, Azeem M, Kluger J. The healthcare utilization and cost of treating patients experiencing inappropriate implantable cardioverter defibrillator shocks: a propensity score study. Pacing Clin Electrophysiol. 2014;37:1315–23.
Bhavnani SP, Kluger J, Coleman CI, White CM, Guertin D, Shafi NA, et al. The prognostic impact of shocks for clinical and induced arrhythmias on morbidity and mortality among patients with implantable cardioverter-defibrillators. Heart rhythm. 2010;7:755–60.
Daubert JP, Zareba W, Cannom DS, McNitt S, Rosero SZ, Wang P, et al. Inappropriate implantable cardioverter-defibrillator shocks in MADIT II: frequency, mechanisms, predictors, and survival impact. J Am Col Cardiol. 2008;51:1357–65.
Moss AJ, Greenberg H, Case RB, Zareba W, Hall WJ, Brown MW, et al. Long-term clinical course of patients after termination of ventricular tachyarrhythmia by an implanted defibrillator. Circulation. 2004;110:3760–5.
Hattori N, Schwaiger M. Metaiodobenzylguanidine scintigraphy of the heart: what have we learnt clinically? Eur J Nucl Med. 2000;27:1–6.
Wieland DM. Wu J-l, Brown LE, Mangner TJ, Swanson DP, Beierwaltes WH. Radiolabeled Adrenergic Neuron-Blocking Agents: Adrenomedullary Imaging with [131I] Iodobenzylguanidine. J Nucl Med. 1980;21:349–53.
Jacobson AF, Senior R, Cerqueira MD, Wong ND, Thomas GS, Lopez VA, et al. Myocardial iodine-123 meta-iodobenzylguanidine imaging and cardiac events in heart failure. Results of the prospective ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Jacobson AF, Senior R, Cerqueira MD, Wong ND, Thomas GS, Lopez VA, et al. Myocardial iodine-123 meta-iodobenzylguanidine imaging and cardiac events in heart failure. Results of the prospective ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) study. J Am Coll Cardiol. 2010;55:2212–21.
Boogers MJ, Borleffs CJW, Henneman MM, van Bommel RJ, van Ramshorst J, Boersma E, et al. Cardiac Sympathetic Denervation Assessed With 123-Iodine Metaiodobenzylguanidine Imaging Predicts Ventricular Arrhythmias in Implantable Cardioverter-Defibrillator Patients. J Amn Coll Cardiol. 2010;55:2769–77.
Verberne HJ, Brewster LM, Somsen GA, van Eck-Smit BL. Prognostic value of myocardial 123I-metaiodobenzylguanidine (MIBG) parameters in patients with heart failure: a systematic review. Eur Heart J. 2008;29:1147–59.
Kuwabara Y, Tamaki N, Nakata T, Yamashina S, Yamazaki J. Determination of the survival rate in patients with congestive heart failure stratified by (1)(2)(3)I-MIBG imaging: a meta-analysis from the studies performed in Japan. Ann Nucl Med. 2011;25:101–7.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–200.
Flotats A, Carrió I, Agostini D, Le Guludec D, Marcassa C, Schaffers M, et al. Proposal for standardization of 123I-metaiodobenzylguanidine (MIBG) cardiac sympathetic imaging by the EANM Cardiovascular Committee and the European Council of Nuclear Cardiology. Eur Nucl Med Mol Imaging. 2010;37:1802–12.
Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation. 2002;105:539–42.
Travin MI. Cardiac autonomic imaging with SPECT tracers. J Nucl Cardiol. 2013;20:128-43; quiz 46.
Holly TA, Abbott BG, Al-Mallah M, Calnon DA, Cohen MC, DiFilippo FP, et al. Single photon-emission computed tomography. J Nucl Cardiol. 2010;17:941–73.
Hajian-Tilaki KO, Hanley JA. Comparison of three methods for estimating the standard error of the area under the curve in ROC analysis of quantitative data. Acad Radiol. 2002;9:1278–85.
Heagerty PJ, Lumley T, Pepe MS. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics. 2000;56:337–44.
Verschure DO, de Groot JR, Mirzaei S, Gheysens O, Nakajima K, van Eck-Smit BLF, et al. Cardiac 123I-mIBG scintigraphy is associated with freedom of appropriate ICD therapy in stable chronic heart failure patients. Int J Cardiol. 2017;248:403–8.
Verschure DO, Veltman CE, Manrique A, Somsen GA, Koutelou M, Katsikis A, et al. For what endpoint does myocardial 123I-MIBG scintigraphy have the greatest prognostic value in patients with chronic heart failure? Results of a pooled individual patient data meta-analysis. Eur Heart J Cardiovasc Imaging. 2014;15:996–1003.
Marshall A, Cheetham A, George RS, Mason M, Kelion AD. Cardiac iodine-123 metaiodobenzylguanidine imaging predicts ventricular arrhythmia in heart failure patients receiving an implantable cardioverter-defibrillator for primary prevention. Heart. 2012;98:1359–65.
Travin MI, Henzlova MJ, van Eck-Smit BLF, Jain D, Carrio I, Folks RD, et al. Assessment of (123)I-mIBG and (99m)Tc-tetrofosmin single-photon emission computed tomographic images for the prediction of arrhythmic events in patients with ischemic heart failure: Intermediate severity innervation defects are associated with higher arrhythmic risk. J Nucl Cardiol. 2017;24:377–91.
de Bakker JM, van Capelle FJ, Janse MJ, Tasseron S, Vermeulen JT, de Jonge N, et al. Slow conduction in the infarcted human heart. ‘Zigzag’ course of activation. Circulation. 1993;88:915–26.
Matsunari I, Schricke U, Bengel FM, Haase HU, Barthel P, Schmidt G, et al. Extent of cardiac sympathetic neuronal damage is determined by the area of ischemia in patients with acute coronary syndromes. Circulation. 2000;101:2579–85.
Kober L, Thune JJ, Nielsen JC, Haarbo J, Videbaek L, Korup E, et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N Engl J Med. 2016;375:1221–30.
Verschure DO, Bongers V, Hagen P, Somsen GA, van Eck-Smit BF, Verberne H. Impact of a predefined mediastinal ROI on inter-observer variability of planar 123I-MIBG heart-to-mediastinum ratio. J Nucl Cardiol. 2014;21:605–13.
Veltman C, Boogers M, Meinardi J, Al Younis I, Dibbets-Schneider P, Van der Wall E, et al. Reproducibility of planar 123I-meta-iodobenzylguanidine (MIBG) myocardial scintigraphy in patients with heart failure. Eur J Nucl Med Mol Imaging. 2012;39:1599–608.
Verschure DO, Poel E, Nakajima K, Okuda K, van Eck-Smit BL, Somsen GA, et al. A European myocardial 123I-mIBG cross-calibration phantom study. J Nucl Cardiol 2017. https://doi.org/10.1007/s12350-017-0782-6. Epub.
Sasano T, Abraham MR, Chang KC, Ashikaga H, Mills KJ, Holt DP, et al. Abnormal sympathetic innervation of viable myocardium and the substrate of ventricular tachycardia after myocardial infarction. J Am Coll Cardiol. 2008;51:2266–75.
Disclosure
The authors have no conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors of this article have provided a PowerPoint file, available for download at SpringerLink, which summarizes the contents of the paper and is free for re-use at meetings and presentations. Search for the article DOI on SpringerLink.com
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
De Vincentis, G., Frantellizzi, V., Fedele, F. et al. Role of cardiac 123I-mIBG imaging in predicting arrhythmic events in stable chronic heart failure patients with an ICD. J. Nucl. Cardiol. 26, 1188–1196 (2019). https://doi.org/10.1007/s12350-018-1258-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-018-1258-z