
Abstract
Background
Triple negative (TN) breast cancer is defined as a subtype that is negative for estrogen receptor (ER), progesterone receptor (PgR), and human epidermal growth factor receptor 2 (HER2). To clarify the characteristics of TN breast cancer, surveillance data of the Registration Committee of the Japanese Breast Cancer Society were analyzed.
Method
Of 14,748 cases registered in 2004, 11,705 (79.4%) were examined for ER, PgR, and HER2. Of these, the most prevalent (53.8%) was a hormone-responsive subtype with ER positive/PgR positive/HER2 negative, followed by TN subtype (15.5%).
Results
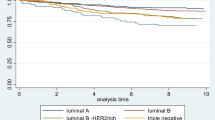
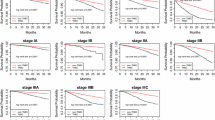
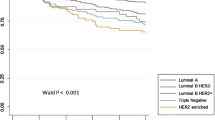
The proportion of postmenopausal patients was relatively high in the TN subtype. This cancer was diagnosed at a slightly advanced stage and with more cases positive for lymph node metastases than other subtypes. Morphologically, the TN subtype was more frequently classified as solid-tubular carcinoma. Mucinous, tubular, or secretary carcinomas were frequently found in the hormone receptor positive/HER2 negative subtype, while squamous cell carcinoma, spindle cell carcinoma, and metaplastic carcinoma with bone/cartilage metaplasia were very frequently found in the TN group. Apocrine carcinoma was also found very frequently in the TN group. Selection of chemotherapy was not based on receptor subtypes, but was determined by the degree of tumor progression.
Conclusions
Although TN types are similar to basal-like breast tumor, as determined by gene profiling, their diagnosis needs verification by determination of the level of epidermal growth factor receptor or cytokeratin 5/6 expression. TN type should be examined further for immunohistochemical features and analyzed for prognostic details in this cohort.




Similar content being viewed by others
References
Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer Registry. Cancer. 2007;109:1721–8.
Carey LA, Dees EC, Sawyer L, Gatti L, Moore DT, Collichio F, et al. The triple negative paradox: primary tumor chemosensitivity of breast cancer subtypes. Clin Cancer Res. 2007;13:2329–34.
Nishimura R, Arima N. Is triple negative a prognostic factor in breast cancer? Breast Cancer. 2008;15:303–8.
Sorlie T, Perou CM, Tibshirani R, Aas T, Geisler S, Johnsen H, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci USA. 2001;98:10869–74.
Sorlie T, Tibshirani R, Parker J, Hastie T, Marron JS, Nobel A, et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc Natl Acad Sci USA. 2003;100:8418–23.
Kobayashi S. Basal-like subtype of breast cancer: a review of its unique characteristics and their clinical significance. Breast Cancer. 2008;15:153–8.
Carey LA, Perou CM, Livasy CA, Dressler LG, Cowan D, Conway K, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006;295:2492–502.
Kurebayashi J, Moriya T, Ishida T, Hirakawa H, Kurosumi M, Akiyama F, et al. The prevalence of intrinsic subtypes and prognosis in breast cancer patients of different races. Breast. 2007;16(Suppl 2):S72–7.
Harvey JM, Clark GM, Osborne CK, Allred DC. Estrogen receptor status by immunohistochemistry is superior to the ligand-binding assay for predicting response to adjuvant endocrine therapy in breast cancer. J Clin Oncol. 1999;17:1474–81.
Umemura S, Kurosumi M, Moriya T, Oyama T, Arihiro K, Yamashita H, et al. Immunohistochemical Evaluation for hormone receptors in breast cancer: a practically useful evaluation system and handling protocol. Breast cancer. 2006;13:232–5.
Millikan RC, Newman B, Tse CK, Moorman PG, Conway K, Dressler LG, et al. Epidemiology of basal-like breast cancer. Breast Cancer Res Treat. 2008;109:123–39.
Reis-Filho JS, Milanezi F, Steele D, Savage K, Simpson PT, Nesland JM, et al. Metaplastic breast carcinomas are basal-like tumours. Histopathology. 2006;49:10–21.
Acknowledgment
We wish to thank Mr. Naohito Fukui, NPO Japan Clinical Research Support Unit. This work was supported by the research fund from the Japanese Breast Cancer Society.
Conflicts of interest statement.
The author and his immediate family members open their conflicts of interest as follows: Employment: none; leadership: none; consultant: none; stock: none; honoraria: H. Iwase, AstraZeneca, Novartis; J. Kurebayashi, AstraZeneca, Takeda; research fund: H. Iwase, AstraZeneca, Taiho, Chugai, Takeda; testimony: none; other: none.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Iwase, H., Kurebayashi, J., Tsuda, H. et al. Clinicopathological analyses of triple negative breast cancer using surveillance data from the Registration Committee of the Japanese Breast Cancer Society. Breast Cancer 17, 118–124 (2010). https://doi.org/10.1007/s12282-009-0113-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12282-009-0113-0