
Abstract
Background
Reasoned action approach (RAA) includes subcomponents of attitude (experiential/instrumental), perceived norm (injunctive/descriptive), and perceived behavioral control (capacity/autonomy) to predict intention and behavior.
Purpose
To provide a meta-analysis of the RAA for health behaviors focusing on comparing the pairs of RAA subcomponents and differences between health protection and health-risk behaviors.
Methods
The present research reports a meta-analysis of correlational tests of RAA subcomponents, examination of moderators, and combined effects of subcomponents on intention and behavior. Regressions were used to predict intention and behavior based on data from studies measuring all variables.
Results
Capacity and experiential attitude had large, and other constructs had small-medium-sized correlations with intention; all constructs except autonomy were significant independent predictors of intention in regressions. Intention, capacity, and experiential attitude had medium-large, and other constructs had small-medium-sized correlations with behavior; intention, capacity, experiential attitude, and descriptive norm were significant independent predictors of behavior in regressions.
Conclusions
The RAA subcomponents have utility in predicting and understanding health behaviors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Identifying the factors predicting engagement in health behaviors has been the focus of considerable research in health psychology. A variety of social cognition models purporting to delineate the key determinants of behavior [1] have been applied to health behaviors. These prominently include the theory of planned behavior (TPB; [2]), an extension of the theory of reasoned action (TRA; [3]). The TPB is a parsimonious model applied to a wide range of health behaviors (for reviews, see [4–10]). In recent years, researchers have sought to develop the TPB by differentiating subcomponents of the model [11, 12]. Despite including very similar constructs, this expanded model (Fig. 1) has been given a variety of names (e.g., two-factor model; [12]). We here refer to this model as the reasoned action approach (RAA; [13]). The present paper provides a meta-analytic review of the RAA subcomponents to health behaviors, test of health behavior type (protection vs. risk) as a moderator, and test of the power of the subcomponents to independently predict intention and behavior.

The subcomponent RAA (dashed lines indicate additional paths suggested by the meta-analysis)
Overview of the TPB and RAA
The TPB states that behavior is determined by an individual’s behavioral intention and that perceived behavioral control (PBC) also determines behavior [2] or moderates the impact of intention on behavior [13]. Intention is held to be the motivational component that spurs an individual to engage in a particular behavior. PBC captures the extent to which people have control over engaging in the behavior or confidence that they can perform the behavior. Intention, in turn, is determined by an individual’s attitude toward the behavior (e.g., whether engaging in the behavior is evaluated to be positive or negative), subjective norms (e.g., perceptions of whether others think one should engage in a behavior), and PBC. Overall, the TPB has been shown to explain 40–49 % of the variance in intention and 26–36 % of the variance in behavior [2, 5, 7, 8, 14, 15]. The most comprehensive meta-analysis of prospective health behavior TPB studies to date [10] reported that intention and PBC explained 19.3 % variance in behavior, while attitude, subjective norm, and PBC explained 44.3 % variance in intention. This meta-analysis also reported that the predictive ability of the TPB varied across different health behaviors.
In the RAA (Fig. 1), the three determinants of intentions are labeled attitude toward the behavior, perceived norm, and PBC [13], with each represented by pairs of distinct, but related, subcomponents [11–13, 16]. In particular, attitude toward the behavior is assumed to consist of experiential and instrumental attitudes; perceived norm is assumed to consist of injunctive and descriptive norms, while PBC is assumed to consist of capacity and autonomy ([13]; see below for definitions). Ajzen and Fishbein [11] have suggested that the subcomponents reflect the more general construct (e.g., experiential and instrumental attitudes reflect overall attitude toward the behavior) and that the more general constructs be used in analyses (i.e., a second-order factor analysis model). Although this has the advantage of parsimony, it has the disadvantage of requiring further theorizing about the relationship between the more general construct and the subcomponents [12]. Considering each of the subcomponents as independent predictors of intention and behavior is the approach taken in the growing number of studies reviewed here. This approach has the advantage of allowing us to examine which subcomponent is the more important predictor and also to test novel pathways (e.g., experiential attitude to behavior). This, in turn, allows us to more precisely specify targets of intervention to change health behaviors. Previous meta-analyses of the TPB have explored subcomponents of the RAA in isolation (e.g., experiential vs. instrumental attitudes [17]; injunctive vs. descriptive norms [18]; capacity vs. autonomy [19]) and pointed to the discriminant validity of the subcomponents. However, there is no meta-analysis of the power of all six subcomponents as zero-order and as independent predictors of intention and behavior. The present meta-analysis addresses this gap in relation to health behaviors and explores type of behavior (i.e., health protection and health-risk behaviors) as a moderator.
The semantic differential measures of attitude toward behavior used in TPB studies often focus more on instrumental or cognitive (e.g., healthy–unhealthy, valuable–worthless) compared to experiential or affective (e.g., pleasant–unpleasant, interesting–boring) aspects of attitude [20, 21]. Studies have found experiential measures of attitude to be more closely linked to intentions [20, 22–25] and behavior [25, 26]. In the RAA, separate measures tap experiential/affective and instrumental/cognitive components of attitude. The two components have medium-sized correlations with one-another [17] but can be discriminated based on their underlying belief systems [27], different functions [28], experimental manipulations [29], and empirical differences [30]. It is suggested that instrumental attitude may impact behavior through a “reflective” path via intention, while experiential attitude operates both via intention and through an “impulsive” direct path to behavior ([25, 31]; Fig. 1).
The perceived norm component of the TPB has also been a focus of research, with the unexpectedly weak predictive power of subjective norm being noted by some authors [5, 32, 33]. One explanation for this weak predictive power is the focus on injunctive norm [34]. Cialdini et al. [34] label the norms in the TPB injunctive norm as they concern the perceived social approval of others which motivates behavior through social reward/punishment, and distinguish them from descriptive norm which are perceptions of what others do [35]. Although some authors argue that injunctive and descriptive norms be considered indicators of the same underlying concept [3, 13, 36], recent research has pointed to their discriminant validity. In a meta-analysis, Rivis and Sheeren [37] found that descriptive norm explained an additional 5 % of variance in intention after taking account of attitude, injunctive norm, and PBC. Similarly, Manning [18] reported that in a meta-analysis of TPB studies measuring injunctive and descriptive norms, injunctive norm was a stronger correlate of intention compared to descriptive norm (r + = 0.51, k = 160; r + = 0.40, k = 17), although the pattern was reversed for predictions of behavior (r + = 0.28, k = 156; r + = 0.34, k = 17). The two constructs show medium-large-sized correlations with one another ([37], r + = 0.38; [18], r + = 0.59) [38]. In distinguishing injunctive and descriptive norms, the RAA allows testing of their independent effects on intention and behavior. In so doing, it helps identify distinct pathways of effect on behavior (e.g., injunctive norm may influence behavior only indirectly through intention as hypothesized in the TPB, while descriptive norm might indirectly influence behavior through intentions and also directly influence behavior reflecting modeling or other processes; Fig. 1).
The difference between the TPB and the earlier TRA lies in the addition of PBC. Meta-analytic reviews support the power of PBC to explain additional variance in intention and behavior after controlling for the components of the TRA [5]. However, overlaps between PBC and self-efficacy [39] have long been noted (see also [13]). Some researchers have advocated the use of measures of self-efficacy in place of PBC alongside components of the TRA [40]. Opinion appears to have coalesced around the idea of PBC tapping two separate but related constructs [13, 15, 19, 41], although the preferred terminology varies. We follow Fishbein and Ajzen [13] in labeling these constructs as capacity and autonomy. Capacity “…deals with the ease or difficulty of performing a behavior, with people’s confidence that they can perform it if they want to do so” [42]. Capacity shows considerable overlap with many definitions of self-efficacy (sometimes also labeled capability). Autonomy “… involves people’s beliefs that they have control over the behavior, that performance or non-performance of the behavior is up to them” [42]. Armitage and Conner [5] reported that capacity (that they labeled self-efficacy) compared to autonomy (labeled perceived control) were stronger correlates of intention (r + = 0.44 vs. 0.23) and behavior (r + = 0.35 vs. 0.18). The RAA, in distinguishing these two components, allows tests of their independent effects on intention and behavior and highlights different pathways of effect on behavior (e.g., capacity influencing behavior both directly and indirectly through intention, while autonomy only directly influencing behavior independent of intention).
The TRA/TPB explicitly states that the power of different components to predict different behaviors might vary [13]. Indeed, one meta-analysis [10] reported type of behavior to be a key moderator of model relationships. Consistent differences between clusters of health behaviors could be expected on theoretical grounds and if confirmed might help guide intervention efforts. For example, the prototype-willingness model (PWM; [43]) is an adaption of the TRA/TPB specifically for risk behaviors in adolescent groups that particularly emphasizes the role of normative influences. Similarly, Conner et al. [17] emphasized the role of experiential/affective influences in applications of the TPB to risk behaviors. The present research reports a meta-analysis of published RAA studies focusing on comparing the pairs of subcomponents, testing differences between health protection versus health-risk behaviors (e.g., previous research suggests that experiential attitudes [17] or descriptive norms [43] may be stronger predictors of behavior for risk compared to protection behaviors), and testing differences in the power of the subcomponents of the RAA to predict intention and behavior in regressions based on those studies measuring all variables.
Method
Searches
Relevant databases (PsycINFO, MEDLINE, Web of Science, CINAHL, Embase) were searched on two occasions (10 May 2010 and 6 November 2012), using the following search strings: (1) attitud* and norm* and control and intention*; OR (2) theory of planned behavi*; OR (3) planned behavi* and Ajzen. Citation searches were performed on three key papers [2, 5, 7], and content pages of key journals were searched (British Journal of Health Psychology, Health Education Research, Health Psychology, Journal of Applied Social Psychology, Psychology and Health). Key authors were contacted to identify additional eligible articles not otherwise identified.
Selection Criteria
The inclusion/exclusion criteria for studies were based on those of McEachan et al. [10], with the addition of one criterion related to measurement of the RAA:
-
1.
Prospective study providing measure of behavior at follow-up.
-
2.
Measuring health behavior. Health behaviors were defined as behaviors which impact or have the potential to impact on the health of an individual in a positive or negative way and included behaviors such as physical activity, safer sex, drug use, and screening.
-
3.
Explicitly testing the TPB and providing overall measures of attitude toward behavior, perceived behavioral control, intention, and either overall perceived norm (k = 35) or a belief-based measure of norm (k = 7).
-
4.
Reporting a minimum sample size of N = 30, reporting zero-order correlations between at least one pair of subcomponent variables and intention or behavior.
-
5.
Measuring at least instrumental and experiential attitude, or injunctive and descriptive norm, or capacity and autonomy.
Following McEachan et al. [10], we excluded studies if they reported cross-sectional or retrospective assessment of behavior; if they described interventions different from “normal care” where no control analyses were reported; and if they reported studies involving professional athletes, descriptions of physician behavior, patient “help-seeking” behavior, or dieting/weight control among general population samples. Studies providing only a “stage of change” algorithm measure of behavior were also excluded. Papers from meeting abstracts, theses, or other unpublished research were not included.
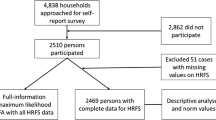
A total of 7619 citations were identified. The first author performed an initial screen and excluded 6684 on the basis of their abstract or title. The full text of the remaining 935 articles were downloaded and then reviewed in a two-stage process. First, articles were screened according to inclusion criteria 1 to 4: 561 were excluded. The full text of the remaining 374 were scrutinized to ascertain whether the paper reported instrumental and experiential attitude, or injunctive and descriptive norm, or capacity and autonomy. A further 292 were excluded. A randomly selected 10 % of articles were independently screened by a second reviewer for inclusion and exclusion, agreement was 96 %; disagreements were discussed and resolved. A total of 82 papers were found to be eligible (Fig. 2), of these 74 papers (including 86 tests) provided sufficient information to be included in the review. A total of 62 (76 %) of the 82 papers were included in the McEachan et al.’s [10] meta-analysis.

Flow of studies for meta-analysis
Data Abstraction
In order to identify which subcomponent RAA variables studies assessed, all items used to measure RAA constructs were extracted from included studies. A code book was developed and piloted (using [12, 42]) to assign measures as assessing general, subcomponent, or belief-based measures of TPB variables (Table 1). One reviewer coded all measures while a second blind coded approximately 50 % (average kappa = 0.97). Disagreements were resolved by discussion.
Moderator Coding
Studies that assessed at least one pair of RAA subcomponents were blind double coded for further characteristics by two reviewers. All disagreements were discussed and resolved. In line with previous reviews [10], we coded the type of health behavior in the study, the type of sample, and time delay from measurement of RAA variables to measurement of behavior (Table 1). It was not possible to include coding of other moderators used in previous meta-analyses of the TPB (e.g., objective vs. self-report measures of behavior) because of limited numbers of studies in at least one category.
Type of health behavior
Following Rothman and Salovey [115], we coded studies into protection (approach), risk (avoidance), or other (e.g., detection, curative) health behaviors. Fifty-nine tests were coded within the protection category. This category included physical activity behaviors (k = 41), behaviors related to a healthy diet (k = 14), using condoms (k = 4) or sunscreen (k = 1), and safe driving (k = 1). Risk behaviors included drinking alcohol, smoking, using drugs, or exceeding the posted speed limit (k = 15). Other behaviors (k = 12) included detection behaviors (general health screening, k = 2; breast self-examination, k = 1; checking blood glucose levels among type 1 diabetic patients, k = 1), quitting smoking (k = 3), breastfeeding (k = 3), and blood donation (k = 2). Due to their heterogeneity, other behaviors were not included in the moderator analyses of behavior type. One paper [25] reported both risk and protection behaviors assessed from one sample. The appropriate correlations from this study were included in estimates for both types of behavior but the sample size halved. Agreement for coding of behavior was 97 %, and disagreements were resolved through discussion.
Type of sample
Type of sample was coded into adolescent or school age (e.g., those recruited directly from schools or youth clubs and who were 17 years or younger, k = 10), student (e.g., undergraduate or postgraduate student samples recruited from university settings, k = 41), or adult samples (e.g., excluding latter two groups and recruited from community settings, k = 30) (cp. [10]). One study contained a mixture of age groups, and four could not be coded (e.g., recruited military trainees; [109]) and so excluded from analyses on type of sample. Agreement for coding was 89 % with disagreements resolved by discussion.
Time interval between measures
This was coded in weeks but was highly skewed (median 3.5 weeks; range = 1–130 weeks). Studies were therefore split into two groups labeled shorter follow-up (≤4 weeks, k = 54) or longer follow-up (>4 weeks, k = 32). Coding agreement was 99 % with disagreements resolved by discussion.
Analysis
Analyses were conducted using Comprehensive Meta-Analysis software, version 2.2.064 [116], and SPSS, version 20, using correlation coefficients extracted from papers. A random effects meta-analysis was performed, with effect size estimates weighted by sample size. Mean effect sizes (r + ), standard deviations, heterogeneity estimates (Q statistic; [117]), percentage of variation accounted for by statistical artifacts (I 2), and fail-safe numbers (FSN) were computed. Significant Q values were indicative of significant heterogeneity. The I 2 statistic was used to quantify the degree of heterogeneity (I 2 values of 25, 50, and 75 % indicate low, moderate, and high levels of heterogeneity, respectively; [118]). FSNs were compared against tolerance levels to assess potential file drawer problems [119]. We also used Egger’s regression test [120] and the Duval and Tweedie’s [121] trim and fill procedure to identify potential publication bias. Moderator analyses of our categorical moderators were undertaken using random effects subgroup analyses. Moderator analyses were only conducted where every category contained at least three studies. Variance between studies was expected to be consistent across subgroups, and thus, the heterogeneity variance within each subgroup (τ 2) was estimated by a single value collapsing across subgroups [116]. Statistical significance of each moderator was assessed using Q tests analogous to analysis of variance, such that a significant between-group Q indicates that the effect size differs significantly as a function of the moderator. Proportion of heterogeneity accounted for by each moderator was computed using adjusted R 2 (ratio of variance explained by the moderator relative to the amount of variance in total), calculated using 1 − (τ 2 within / τ 2 total) [116].
In order to explore the simultaneous impact of predictor variables in explaining intention and in explaining behavior, we used multiple regression based on the frequency-weighted mean correlations. However, given the fact that the number of tests contributing to estimates of individual correlations varied so much, leading to potential problems of nonpositive definite matrices, we decided to base these analyses only on those studies (k = 14, N = 3990) that included all components of the RAA. We report the correlation matrix that regressions were based on. For regressions predicting intention, instrumental and experiential attitudes, injunctive and descriptive norms, capacity and autonomy were entered simultaneously. For regressions predicting behavior, at a first step, we entered intention, capacity and autonomy (to parallel the TPB), followed by all remaining variables at step 2. For each step of each regression, we report the percentage additional variance explained (ΔR 2) and the independent contribution of each construct in the form of unstandardized beta weights (B), standard errors (SE), and standardized beta weights (β).
Results
Overview of Tests
Table 1 shows that of the total pool of 86 tests, 49 tests compared instrumental and experiential attitudes (of these, k = 39 were coded as preventive, k = 3 as risk, k = 7 as other), 42 tests compared injunctive and descriptive norms (k = 23 preventive, k = 9 risk, k = 10 as other), and 36 tests compared autonomy and capacity (k = 20 preventive, k = 10 risk, k = 6 as other). There were only 14 full tests of the full subcomponent model from eight papers. Table 1 also shows the coding of each study by type of sample and time interval between measures.
Overall Effect Sizes
Table 2 shows the meta-analysis correlations for each of the six constructs with intention and behavior; intercorrelations between the pairs of constructs are also reported. Z tests were used to compare the relative magnitude of subcomponent constructs correlations with intention and behavior. Capacity and experiential attitude showed large-sized correlations with intention, while instrumental attitude, injunctive norm, descriptive norm, and autonomy showed medium-large-sized correlations with intention. The intercorrelations between instrumental and experiential attitudes, injunctive and descriptive norms, and capacity and autonomy were of medium-large magnitude (Table 2; [38]). Intention, capacity, and experiential attitude all showed medium-large-sized correlations with behavior. Instrumental attitude, descriptive norm, autonomy, and injunctive norm showed small-medium-sized correlations with behavior. Compared to instrumental attitude, experiential attitude showed significantly stronger associations with both intention (experiential: r + = 0.546; instrumental: r + = 0.384) and behavior (experiential: r + = 0.299; instrumental: r + = 0.195). The same pattern was apparent for capacity versus autonomy (intention: capacity: r + = 0.598; autonomy: r + = 0.268; behavior: capacity: r + = 0.388; autonomy: r + = 0.189). There were also significant but more modest differences in the magnitude of correlations between injunctive or descriptive norms with intention (injunctive norm: r + = 0.389; descriptive norm: r + = 0.351) or behavior (injunctive norm: r + = 0.220; descriptive norm: r + = 0.265).
Egger’s regression test revealed significant asymmetry (ts > 1.86, ps < 0.05) for six correlations (four correlations with behavior and two with intention). For each correlation, we then used the Trim and Fill method [121] to examine effects sizes after studies were trimmed compared to those reported in Table 2. In one case, the values reduced by 0.003 (capacity–behavior: one study trimmed; r + = 0.385, 95 % CI 0.335–0.432), while in the other cases, the values increased by between 0.006 and 0.048 (instrumental attitude–behavior: eight studies trimmed; r + = 0.232, 95 % CI 0.185–0.278; injunctive norm–behavior: nine studies trimmed; r + = 0.266, 95 % CI 0.227–0.305; autonomy–behavior: nine studies trimmed; r + = 0.232, 95 % CI 0.187–0.277; instrumental attitude–intention: nine studies trimmed; r + = 0.414, 95 % CI 0.355–0.470; autonomy–intention: eight studies trimmed; r + = 0.331, 95 % CI 0.266–0.393). The fail safe number (FSN) for effects reported in Table 2 ranged from a low of 1848 (for autonomy–behavior) to a high of 106,267 (for intention–behavior). These findings suggest the influence of publication bias in the meta-analysis can be designated as modest rather than severe.
The above results appear unlikely to be unduly influenced by the reliability of the measures of each construct. The majority of studies used multiple items to measure each construct (ranging from 71 % of studies for autonomy to 100 % of studies for experiential attitude) and the reliability of these multi-item scales was generally good (mean Cronbach’s alphas ranging from 0.72 for descriptive norms to 0.82 for experiential attitudes). Excluding studies with low reliabilities (alpha < 0.60) did not substantively alter the Table 2 correlations.
Moderator Analyses
In relation to the correlations reported in Table 2, all Q values were significant (ps < 0.001) and the I 2 statistic ranged between 74.75 and 94.54 %, indicating moderate to high levels of heterogeneity for all correlations. We assessed the impact of type of behavior and sample as moderators of all correlations and time interval between measures as a moderator of relationships with prospective measures of behavior (Table 3). In relation to type of behavior, there were significant moderation effects for eight relationships. Intention, experiential attitude, instrumental attitude, injunctive norm, and descriptive norm were each significantly stronger correlates of behavior in risk compared to protection behaviors. In addition, experiential attitude and instrumental attitude were significantly stronger correlates of intention in risk compared to protection behaviors. Finally, the autonomy–capacity correlation was significantly stronger in protection compared to risk behaviors (Table 3).
In relation to type of sample, only the relationship between descriptive norm and behavior was significantly moderated (Table 3). Subgroup analysis indicated that the strongest correlation was for school samples, then students and finally older samples. In each case, the comparisons between each pair were significant (Qs > 8.27, ps < 0.001). Finally, in relation to time interval between measures, only the relationship between intention and behavior was significantly moderated (Table 3). Intention was a significantly stronger predictor of behavior in studies with shorter compared to longer time intervals between measurement of cognitions and behavior.
Predicting Intention and Behavior
Given the considerable variation in the number of studies contributing to the estimate of each bivariate correlation we decided to base our regression analyses on the subset of studies estimating all relationships. This has the advantage of being more likely to produce a positive definite correlation matrix but the disadvantage of limiting the number of studies included. Table 4 reports the correlation matrix used in these regressions. Examination of the relevant correlations in Tables 2 and 4 indicate generally higher values in Table 4 although the relative magnitude of correlations was similar.
Multiple regression analyses of the correlation matrix of average effect sizes for the studies that estimated all relationships in the RAA (k = 14; N = 3990) indicated experiential attitude, capacity, instrumental attitude, injunctive norm, and descriptive norm were each significant independent predictors of intention explaining 58.7 % of the variance, F(6,3983) = 942.4, p < 0.001. Autonomy was not a significant predictor of intention. Experiential attitude and capacity were the strongest predictors of intention (Table 5).
In relation to behavior, multiple regression analyses using the same correlation matrix indicated that intention and capacity, but not autonomy, were significant independent predictors (Table 5, step 1) explaining 30.9 % of the variance, F(3,3986) = 595.1, p < 0.001. Adding experiential attitude, instrumental attitude, injunctive norm, and descriptive norm explained a further 1.4 % of the variance in behavior (F(4,3982) = 21.2, p < 0.001), with intention, capacity, experiential attitude, and descriptive norm significant at this step (Table 5, step 2). Autonomy, instrumental attitude, and injunctive norm were not significant predictors of behavior. Intention was the dominant predictor of behavior (Table 5), indeed entering intention alone explained 30.4 % of the variance in behavior, B = 0.551, SE = 0.013, F(1,3988) = 1738.6, p < 0.001.
Discussion
This meta-analysis assessed the power of the RAA in relation to prospective tests on health behaviors. The RAA with subcomponents extends the TPB by splitting each of attitude toward behavior, perceived norm, and PBC into two subcomponents [13, 122]. The meta-analysis provided support for the discriminant validity of the subcomponent conceptualization of experiential versus instrumental attitudes, injunctive versus descriptive norms, and capacity versus autonomy (i.e., correlations between pairs of constructs was only of medium-large magnitude and did not approach 1.0; Table 2). Capacity and experiential attitudes showed large-sized correlations with intention, while instrumental attitude, injunctive norm, descriptive norm and autonomy showed medium-large-sized correlations with intention. Intention, capacity, and experiential attitude all showed medium-large-sized correlations with behavior, while instrumental attitude, descriptive norm, autonomy, and injunctive norm showed small-medium-sized correlations. Compared to instrumental attitude, experiential attitude showed significantly stronger associations with both intention and behavior. The same pattern was apparent for capacity versus autonomy, with the former being a significantly stronger correlate of both intention and behavior. The differences in magnitude of correlations between injunctive or descriptive norms with intention or behavior were more modest but still significant, with injunctive norm being the stronger predictor of intention and descriptive norm being the stronger predictor of behavior (Table 2).
Significant heterogeneity in the correlations was only partly explained by our moderators, suggesting the need to treat these findings with some caution. Our key moderating variable of type of behavior significantly influenced the relationship between intention and behavior, between experiential or instrumental attitudes and intention or behavior, between injunctive or descriptive norm and behavior, and between autonomy and capacity. This suggests interesting directions for future research. Given that experiential attitude, instrumental attitude, and descriptive norm were significant stronger predictors of risk compared to protection behaviors, this might suggest the particular importance of these variables in relation to risk behaviors and the potential value of differentially targeting variables when attempting to change risk versus protection behaviors.
There were also significant moderating effects for our other two moderators. Time delay between measurement of intention and behavior significantly moderated this relationship, supporting previous meta-analyses of the TPB [10] in showing stronger correlations over shorter intervals. This is a limiting condition of the TRA/TPB, although intention can still predict over prolonged time intervals [123]. That the descriptive norm–behavior relationship was significantly stronger in adolescent/school aged compared to adult samples is a noteworthy finding (cp. [10]), particularly given the direct effects of descriptive norm on behavior independent of intention and other constructs (see below). In practical terms, interventionists targeting younger age groups might usefully focus on targeting descriptive norm with strategies such as modeling or group performance.
Regression analyses indicated experiential attitudes and capacity to be the strongest predictors of intention, although instrumental attitude, injunctive norm, and descriptive norm were also significant independent predictors of intention explaining a total of 58.7 % of the variance. Only autonomy was not a significant predictor. This is a higher percentage of variance than reported in previous meta-analyses of the TPB [10], although direct comparisons are difficult given differences in the number of predictors. Nevertheless, this is an impressive amount of explained variance and approaches the limits that may be possible given measurement error in measuring each construct. Regression analyses also indicated that intention was the strongest predictors of behavior, but that capacity, experiential attitude, and descriptive norm were also significant, explaining 32.3 % of the variance. Autonomy, instrumental attitude, and injunctive norm were not significant predictors of behavior. Key differences between the TPB and RAA with subcomponents here are the direct effects that experiential attitude and descriptive norm have on behavior in the RAA and the lack of direct effect on intention or behavior for autonomy in the RAA. Nevertheless, in general, the findings broadly support the RAA with intention being the dominant predictor of behavior [13].
A number of important differences emerge between the RAA and TPB. First, although both experiential and instrumental attitudes are significant correlates of intention and behavior, and both are significant simultaneous predictors of intention in regressions, only experiential attitude is a significant predictor of behavior in regressions controlling for RAA variables. Second, injunctive and descriptive norms are significant correlates of intention and behavior, and both are significant simultaneous predictors of intention in regression. However, only descriptive norm is a significant predictor of behavior in regressions controlling for other RAA variables. Third, of the two constructs making up PBC, a differentiated pattern emerges for capacity and autonomy. Both constructs are significant positive correlates of intention and behavior, although capacity has a significantly stronger correlation in each case (Table 2). Capacity was a significant positive predictor of intention when controlling for other RAA constructs, while autonomy was a nonsignificant negative predictor of intention. Capacity was a significant positive predictor of behavior when controlling for intention and autonomy. Capacity remained a significant predictor of behavior controlling for all RAA constructs. Autonomy was not a significant predictor of behavior in the regressions across behaviors. Fourth, protection-risk behavior comparisons indicated significant moderation effects for correlations. These four key findings are now discussed in more detail.
In relation to the first point, the support for the important role of experiential compared to instrumental attitudes as a predictor of both intention and behavior supports a growing body of research in this area including intervention studies [29]. Experiential attitude appears to be a key determinant of intention and behavior [17]. Independent effects for both attitudes on intention suggest the value of targeting both in relation to changing intention as a means to change behavior (i.e., an indirect effect). Also, the additional significant direct effect of experiential attitude on behavior independent of intention suggests that changing experiential attitude compared to instrumental attitude could have stronger impacts on behavior change given the direct and indirect paths. Further research attempting to independently manipulate experiential and instrumental attitudes and observing effects on intention and behavior (and the relative size of direct and indirect paths to behavior) is required. The direct path by which experiential attitude influences behavior may be particularly important as it suggests a nonreasoned path to behavior (i.e., not mediated by intention; Fig. 1). It might be that experiential attitude better reflects impulsive influences on behavior. Some support for this hypothesis comes from the relative strength of experiential attitude compared with instrumental attitude in predicting the more hedonic and impulsive “risk” behaviors. Interventionists should take into account these patterns of prediction when designing interventions to change protection versus risk behaviors. Nevertheless, the relatively small amount of variance explained by experiential attitude over and above intention indicates the importance of targeting intentions.
In relation to the second point, support for both injunctive and descriptive norms as correlates of intention and behavior is a further important finding. Given that the TPB has previously only focused on injunctive norm, this might help explain why norms appeared to have only a relatively modest impact on intention compared to other constructs. Both injunctive and descriptive norms emerge as independent predictors of intention. Direct effects of descriptive norm on behavior independent of intention may reflect modeling processes (Fig. 1). Further research independently manipulating injunctive and descriptive norms and observing effects on intention and behavior (and the relative size of direct/indirect paths to behavior) is required. Although it is again worth noting that intention is the dominant predictor of behavior.
In relation to the third point, the current findings for capacity and autonomy partially support the idea of research focusing on the former [19, 40]. In the context of health behaviors, capacity was a significantly stronger correlate of both intention and behavior and a more consistent independent predictor of intention and behavior when controlling for other RAA constructs. There were no significant effects for autonomy in regressions. A recent review of drinking alcohol noted that autonomy was negatively related to intention and behavior [124]. Further research exploring effects for autonomy on intention and behavior in risk versus protection health behaviors is warranted. However, the current research provides little support for a focus on autonomy. In contrast, the observed effects of capacity support the emphasis on this construct (labeled as self-efficacy) in other research perspectives such as social cognitive theory [125] and protection motivation theory [126]. However, further research that independently manipulates autonomy and capacity and observes effects on intention and behavior might be useful before focusing attention solely on capacity to the exclusion of autonomy. Indeed, recent research [127, 128] has called for more focus on measures of autonomy rather than capacity because the former is a purer measure of perceived capability. Williams and colleagues [128] suggest that capacity measures (labeled self-efficacy) may reflect motivation rather than perceived capability. The strong predictive power of capacity in relation to intention and behavior could be seen as consistent with the latter point. However, the weak effects for autonomy observed here might suggest a limited predictive power for purer measures of perceived capability such as autonomy (see [129] for a useful discussion of the two aspects of perceived behavioral control that the RAA distinguishes).
In relation to the fourth point, a number of significant differences emerged for the application of the RAA to protection versus risk behaviors. The two consistent findings were the significantly stronger effects for experiential attitudes and descriptive norms on behavior for risk compared to protection behaviors, although both constructs were significant predictors of behavior for both types of behaviors. The meta-analysis indicated significant differences in simple correlations. These findings suggest that it might be valuable to target changes in experiential attitude and descriptive norm in order to directly (independent of intention) change health behaviors, and that this may be a particularly potent approach for risk behaviors. Further research that independently manipulates experiential attitude and descriptive norm and observes effects on behavior for protection versus risk behaviors would be valuable in testing these predictions. In identifying differences between protection and risk behaviors, the present research adds further support for the idea that a “one size fits all” approach to developing interventions is undesirable [10]. Future research could usefully test whether interventions that change the key predictors identified here produces different effects for protection versus risk behaviors. The added value of distinguishing between individual protection or risk behaviors in terms of predictors is also an issue for further research.
The present research has a number of strengths including examining a range of health behaviors. There are also a number of weaknesses including a reliance on self-reported behavior measures and failure to examine the effects of controlling for past behavior (see [130] for useful discussion of this issue). An important further weakness is the lack of a direct comparison of the TPB and RAA. In the present data, the RAA explained 58.7 and 32.3 % of the variance in intention and behavior, respectively, considerably higher than the values previously reported for intention (44.3 %) and behavior (19.3 %) [10]. However, simple direct comparisons of the two in terms of amount of variance explained in intention or behavior are difficult to interpret given the larger number of predictors in the RAA compared to the TPB. Nevertheless, the new pathways to behavior identified here for the RAA (Fig. 1), particularly if supported in subsequent research, may be considered an important advantage that offsets the loss in parsimony for the subcomponent version of the RAA over the TPB. Nevertheless, further studies testing the discriminant validity of pairs of constructs (e.g., instrumental vs. experiential attitude) or novel studies showing that the constructs can be independently manipulated would be particularly valuable in more clearly demonstrating the value of the subcomponents of the RAA over the TPB.
In summary, the present paper indicates the potential value of the subcomponents of the RAA in helping us understand the determinants of health behaviors. Although less parsimonious than the TPB, the RAA with subcomponents offers unique insights into the determinants of health behaviors. Experiential attitude, instrumental attitude, injunctive norm, descriptive norm, and capacity emerge as consistent predictors of intention, while intention, capacity, experiential attitude, and descriptive norm emerge as predictors of behavior. Novel direct effects of experiential attitude and descriptive norm on behavior, independent of intention, suggest important unplanned influences on behavior that might form additional targets for interventions designed to change health behaviors (Fig. 1, dashed lines). An important future test of the RAA subcomponents will be the extent to which the unique insights it provides into the determinants of health behaviors are supported in direct experimental tests of manipulations that test specific pathways in the model.
References
Conner M, Norman P, eds. Predicting and changing health behaviour: Research and practice with social cognition models. 3rd ed. Maidenhead: Open University Press; 2015.
Ajzen I. The theory of planned behavior. Organ Behav Hum Decis. 1991; 50: 179-211.
Ajzen I, Fishbein M. Understanding attitudes and predicting social behavior. Englewood-Cliff, NJ: Prentice-Hall; 1980.
Albarracin D, Johnson BT, Fishbein M, et al. Theories of reasoned action and planned behavior as models of condom use: A meta-analysis. Psychol Bull. 2001; 127: 142-161.
Armitage CJ, Conner M. Efficacy of the theory of planned behaviour: A meta-analytic review. Brit J Soc Psychol. 2001; 40: 471-499.
Cooke R, French DP. How well do the theory of reasoned action and theory of planned behaviour predict intentions and attendance at screening programmes? A meta-analysis. Psychol Health. 2008; 23: 745-765.
Godin G, Kok G. The theory of planned behavior: A review of its applications to health-related behaviors. Am J Health Promot. 1996; 11: 87-98.
Hagger M, Chatzisarantis N, Biddle S. A meta-analytic review of the theories of reasoned action and planned behavior in physical activity: predictive validity and the contribution of additional variables. J Sport Exerc Psychol. 2002; 24: 3-32.
Hausenblas HA, Carron AV, Mack DE. Application of the theories of reasoned action and planned behavior to exercise behavior: A meta-analysis. J Sport Exerc Psychol. 1997; 19: 36-51.
McEachan RRC, Conner M, Taylor NJ, et al. Prospective prediction of health-related behaviors with the Theory of Planned Behavior: A meta-analysis. Health Psychol Rev. 2011; 5: 97-144.
Ajzen I, Fishbein M. The influence of attitudes on behavior. In: Albarracin D, Johnson BT, Zanna MP, eds. Handbook of attitudes and attitude change: Basic principles. Mahwah, NJ: Erlbaum; 2005: 173-221.
Conner M, Sparks P. The theory of planned behaviour and health behaviours. In: Conner M, Norman P, eds. Predicting health behaviour: Research and practice with social cognition models. 2nd ed. Maidenhead: Open University Press; 2005: 170-222.
Fishbein M, Ajzen I. Predicting and changing behavior: The reasoned action approach. New York, NY: Psychology Press; 2010.
Schulze R, Whittmann WW. A meta-analysis of the Theory of Reasoned Action and the Theory of Planned Behavior: The principle of compatibility and multidimensionality of beliefs as moderators. In: Schulze R et al., eds. Meta-analysis: New Developments and Applications in Medical and Social Sciences. Ashland, OH: Hogrefe & Huber Publishers; 2003: 219-250.
Trafimow D, Sheeran P, Conner M, et al. Evidence that perceived behavioral control is a multidimensional construct: Perceived control and perceived difficulty. Brit J Soc Psychol. 2002; 41: 101-121.
Head KJ, Noar SM. Facilitating progress in health behaviour theory development and modification: The reasoned action approach as a case study. Health Psychol Rev. 2014; 8: 34-52.
Conner M, McEachan R, Taylor N, et al. Role of affective attitudes and anticipated affective reactions in predicting health behaviors. Health Psychol. 2015; 34: 642-652.
Manning M. The effects of subjective norms on behaviour in the theory of planned behaviour: A meta analysis. Brit J Soc Psychol. 2009; 48: 649-705.
Rodgers WM, Conner M, Murray TC. Distinguishing among perceived control, perceived difficulty, and self-efficacy as determinants of intentions and behaviours. Brit J Soc Psychol. 2008; 47: 607-630.
Ajzen I, Driver BL. Application of the theory of planned behavior to leisure choice. J Leis Res. 1992; 24: 207-224.
Crites SL, Fabrigar LR, Petty RE. Measuring the affective and cognitive properties of attitudes: conceptual and methodological issues. Personal Soc Psychol Bull. 1994; 20: 619-34.
Ajzen A, Timko C. Correspondence between health attitudes and behavior. Basic Appl Soc Psychol. 1986; 7: 259-276.
Chan DK, Fishbein M. Determinants of college women’s intentions to tell their partners to use condoms. Basic Appl Soc Psychol. 1993; 23: 1455-70.
Manstead ASR, Parker D. Evaluating and extending the Theory of Planned Behaviour. Eur Rev Soc Psychol. 1995; 6: 69-95.
Lawton R, Conner M, McEachan R. Desire or reason: Predicting health behaviors from affective and cognitive attitudes. Health Psychol. 2009; 28: 56-65.
Lawton R, Conner M, Parker D. Beyond cognition: Predicting health risk behaviors from instrumental and affective beliefs. Health Psychol. 2007; 26: 259-267.
Trafimow D, Sheeran P. Some tests of the distinction between cognitive and affective beliefs. J Exp Soc Psychol. 1998; 34: 378-97.
Breckler SJ, Wiggins EC. Affect versus evaluation in the structure of attitudes. J Exp Soc Psychol. 1989; 25: 253-271.
Conner M, Rhodes R, Morris B, et al. Changing exercise through targeting affective or cognitive attitudes. Psychol Health. 2011; 26: 133-149.
Eagly AH, Chaiken S. The psychology of attitudes. Harcourt Brace Jovanovich: Fort Worth, TX; 1993.
Strack F, Deutsch R. Reflective and impulsive determinants of social behavior. Personal Soc Psychol Rev. 2004; 8: 220-47.
Sheppard BH, Hartwick J, Warshaw PR. The theory of reasoned action: A meta-analysis of past research with recommendations for modifications and future research. J Consum Res. 1988; 15: 325-339.
Van den Putte B. On the theory of reasoned action. Unpublished doctoral dissertation. Amsterdam, the Netherlands: University of Amsterdam; 1991.
Cialdini RB, Kallgren CA, Reno RR. A focus theory of normative conduct: A theoretical refinement and re-evaluation of the role of norms in human behavior. Adv Exp Soc Psychol. 1991; 24: 201-234.
Deutsch M, Gerard HB. A study of normative and informational social influences upon individual judgment. J Abnorm Soc Psychol. 1955; 51: 629-636.
Fishbein M. Introduction. In: Terry DJ, Gallois C, McCamish M, eds. The Theory of Reasoned Action: Its Application to AIDS-preventive Behaviour. Oxford: Pergamon; 1993: 15-25.
Rivis A, Sheeran P. Descriptive norms as an additional predictor in the theory of planned behaviour: A meta-analysis. Curr Psychol. 2003; 22: 218-33.
Cohen J. A power primer. Psychol Bull. 1992; 112: 155-159.
Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol Rev. 1977; 84: 191-215.
de Vries H, Backbier E, Kok G, et al. The impact of social influences in the context of attitude, self-efficacy, intention and previous behavior as predictors of smoking onset. J Appl Soc Psychol. 1995; 25: 237-257.
Ajzen I. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. J Appl Soc Psychol. 2002; 32: 1-20.
Ajzen, I. Constructing a TpB questionnaire: Conceptual and methodological considerations. Available at http://www.people.umass.edu/aizen/pdf/tpb.measurement.pdf. Accessibility verified July 12 2006.
Gibbons FX, Gerrard M. Predicting young adults’ health risk behavior. J Pers Soc Psychol. 1995; 69: 505-517.
Abraham C, Henderson M, Der G. Cognitive impact of a research-based school sex education programme. Psychol Health. 2004; 19: 689-703.
Armitage CJ, Conner M. Distinguishing perceptions of control from self-efficacy: Predicting consumption of a low-fat diet using the theory of planned behavior. J Appl Soc Psychol. 1999; 29: 72-90.
Armitage CJ, Conner M. The theory of planned behaviour: Assessment of predictive validity and ‘perceived control’. Brit J Soc Psychol. 1999; 38: 35-54.
Armitage CJ, Conner M, Loach J, et al. Different perceptions of control: Applying an extended theory of planned behavior to legal and illegal drug use. Basic Appl Soc Psychol. 1999; 21: 301-316.
Berg C, Jonsson I, Conner M. Understanding choice of milk and bread for breakfast among Swedish children aged 11–15 years: an application of the Theory of Planned Behaviour. Appetite. 2000; 34: 5-19.
Bish A, Sutton S, Golombok S. Predicting uptake of a routine cervical smear test: A comparison of the health belief model and the theory of planned behaviour. Psychol Health. 2000; 15: 35-50.
Blanchard CM, Fisher J, Sparling PB, et al. Understanding adherence to 5 servings of fruits and vegetables per day: A Theory of Planned Behavior perspective. J Nutr Educ Behav. 2009; 41: 3-10.
Blanchard CM, Kupperman J, Sparling PB, et al. Do ethnicity and gender matter when using the theory of planned behavior to understand fruit and vegetable consumption? Appetite. 2009; 52: 15-20.
Blanchard C, Fisher J, Sparling P, et al. Understanding physical activity behavior in African American and Caucasian college students: An application of the theory of planned behavior. J Am Coll Health. 2008; 56: 341-346.
Blanchard CM, Kupperman J, Sparling P, et al. Ethnicity and the theory of planned behavior in an exercise context: A mediation and moderation perspective. Psychol Sport Exerc. 2008; 9: 527-545.
Boudreau F, Godin G, Pineau R, et al. Health risk appraisal in an occupational setting and its impact on exercise behaviour. J Occup Environ Med. 1995; 37: 1145-1150.
Bryan AD, Rocheleau CA. Predicting aerobic versus resistance exercise using the theory of planned behavior. Am J Health Behav. 2002; 26: 83-94.
Chatzisarantis NLD, Hagger MS, Wang CKJ, et al. The effects of social identity and perceived autonomy support on health behaviour within the Theory of Planned Behaviour. Curr Psychol. 2009; 28: 55-68.
Conner M, Godin G, Sheeran P, et al. Some feelings are more important: Cognitive attitudes, affective attitudes, anticipated affect, and blood donation. Health Psychol. 2013; 32: 264-272.
Conner M, McMillan B. Interaction effects in the theory of planned behaviour: Studying cannabis use. Brit J Soc Psychol. 1999; 38: 195-222.
Conner M, Rodgers W, Murray T. Conscientiousness and the intention-behavior relationship: Predicting exercise behavior. J Sport Exerc Psycol. 2007; 29: 518-533.
Conner M, Sherlock K, Orbell S. Psychosocial determinants of ecstasy use in young people in the UK. Brit J Health Psychol. 1998; 3: 295-317.
de Bruijn GJ, Keer M, van den Putte B, et al. Need for affect, need for cognition, and the intention-fruit consumption relationship: An action-control perspective. Health Educ J. 2012; 71: 617-628.
de Bruijn GJ, Rhodes RE, van Osch L. Does action planning moderate the intention-habit interaction in the exercise domain? A three-way interaction analysis investigation. J Behav Med. 2012; 35: 509-519.
de Bruijn GJ, Verkooijen K, de Vries NK, et al. Antecedents of self-identity and consequences for action control: An application of the theory of planned behaviour in the exercise domain. Psychol Sport Exerc. 2012; 13: 771-778.
Dunn KI, Mohr P, Wilson CJ, et al. Determinants of fast-food consumption. An application of the Theory of Planned Behaviour. Appetite. 2011; 57: 349-357.
Elliott MA, Ainsworth K. Predicting university undergraduates’ binge-drinking behavior: A comparative test of the one- and two-component theories of planned behavior. Addict Behav. 2012; 37: 92-101.
Elliott MA, Thomson JA. The social cognitive determinants of offending drivers’ speeding behaviour. Accid Anal Prev. 2010; 42: 1595-1605.
Gardner ER, Hausenblas HA. Understanding exercise and diet motivation in overweight women enrolled in a weight-loss program: A prospective study using the theory of planned behavior. J Appl Soc Psychol. 2004; 34: 1353-1370.
Eves F, Hoppe R, McLaren U. Prediction of specific types of physical activity using the theory of planned behavior. J Appl Biobehav Res. 2003; 8: 77-95.
Giles M, Liddell C, Bydawell M. Condom use in African adolescents: The role of individual and group factors. AIDS Care. 2005; 17: 729-739.
Giles M, McClenahan C, Cairns E, et al. An application of the Theory of Planned Behaviour to blood donation: The importance of self-efficacy. Health Educ Res. 2004; 19: 380-391.
Godin G, Anderson D, Lambert LD, et al. Identifying factors associated with regular physical activity in leisure time among Canadia adolescents. Am J Health Promot. 2005; 20: 20-27.
Hagger MS, Chatzisarantis NLD. First- and higher-order models of attitudes, normative influence, and perceived behavioural control in the theory of planned behaviour. Brit J Soc Psychol. 2005; 44: 513-535.
Hoie M, Moan IS, Rise J, et al. Using an extended version of the theory of planned behaviour to predict smoking cessation in two age groups. Addict Res Theory. 2012; 20: 42-54.
Jackson C, Smith RA, Conner M. Applying an extended version of the Theory of Planned Behaviour to physical activity. J Sports Sci. 2003; 21: 119-133.
Karvinen KH, Courneya KS, Plotnikoff RC, et al. A prospective study of the determinants of exercise in bladder cancer survivors using the Theory of Planned Behavior. Support Care Cancer. 2009; 17: 171-179.
Kellar I, Abraham C. Randomized controlled trial of a brief research-based intervention promoting fruit and vegetable consumption. Brit J Health Psychol. 2005; 10: 543-558.
Kraft P, Rise J, Sutton S, et al. Perceived difficulty in the theory of planned behaviour: Perceived behavioural control or affective attitude? Brit J Soc Psychol. 2005; 44: 479-496.
Lawton R, Ashley L, Dawson S, et al. Employing an extended Theory of Planned Behaviour to predict breastfeeding intention, initiation, and maintenance in White British and South-Asian mothers living in Bradford. Brit J Health Psychol. 2012; 17: 854-871.
Lowe R, Eves F, Carroll D. The influence of affective and instrumental beliefs on exercise intentions and behavior: A longitudinal analysis. J Appl Soc Psychol. 2002; 32: 1241-1252.
McEachan RRC, Sutton S, Myers L. Mediation of personality influences on physical activity within the Theory of Planned Behaviour. J Health Psychol. 2010; 15: 1170-1180.
McMillan B, Conner M. Applying an extended version of the theory of planned behavior to illicit drug use among Students. J Appl Soc Psychol. 2003; 33: 1662-1683.
McMillan B, Conner M, Woolridge M, et al. Predicting breastfeeding in women living in areas of economic hardship: Explanatory role of the theory of planned behaviour. Psychol Health. 2008; 23: 767-788.
McMillan B, Higgins AR, Conner M. Using an extended theory of planned behaviour to understand smoking amongst schoolchildren. Addict Res Theory. 2005; 13: 293-306.
Molla M, Astrom AN, Brehane Y. Applicability of the theory of planned behavior to intended and self-reported condom use in a rural Ethiopian population. AIDS Care. 2007; 19: 425-431.
Myers LB, Horswill MS. Social cognitive predictors of sun protection intention and behavior. Behav Med. 2006; 32: 57-63.
Norman P. The theory of planned behavior and binge drinking among undergraduate Students: Assessing the impact of habit strength. Addict Behav. 2011; 36: 502-507.
Norman P, Armitage CJ, Quigley C. The theory of planned behavior and binge drinking: Assessing the impact of binge drinker prototypes. Addict Behav. 2007; 32: 1753-1768.
Norman P, Conner M. The theory of planned behaviour and binge drinking: Assessing the moderating role of past behaviour within the theory of planned behaviour. Brit J Health Psychol. 2006; 11: 55-70.
Norman P, Hoyle S. The theory of planned behavior and breast self-examination: Distinguishing between perceived control and self-efficacy. J Appl Soc Psychol. 2004; 34: 694-708.
Payne N, Jones F, Harris P. The impact of working life on health behavior: The effect of job strain on the cognitive predictors of exercise. J Occup Health Psychol. 2002; 7: 342-353.
Payne N, Jones F, Harris PR. The role of perceived need within the theory of planned behaviour: A comparison of exercise and healthy eating. Brit J Health Psychol. 2004; 9: 489-504.
Plotnikoff RC, Courneya KS, Trinh L, et al. Aerobic physical activity and resistance training: an application of the theory of planned behavior among adults with type 2 diabetes in a random, national sample of Canadians. Int J Behav Nutr Phys. 2008; 5: 61.
Povey R, Conner M, Sparks P, et al. The theory of planned behaviour and healthy eating: Examining additive and moderating effects of social influence variables. Psychol Health. 2000; 14: 991-1006.
Povey R, Conner M, Sparks P, et al. Application of the theory of planned behaviour to two dietary behaviours: Roles of perceived control and self-efficacy. Brit J Health Psychol. 2000; 5: 121-139.
Raudsepp L, Viira R, Hannus A. Prediction of physical activity intention and behavior in a longitudinal sample of adolescent girls. Percept Mot Skills. 2010; 110: 3-18.
Rhodes RE, Blanchard CM. Do sedentary motives adversely affect physical activity? Adding cross-behavioural cognitions to the theory of planned behaviour. Psychol Health. 2008; 23: 789-805.
Rhodes RE, Blanchard CM, Matheson DH, et al. Disentangling motivation, intention, and planning in the physical activity domain. Psychol Sport Exerc. 2006; 7: 15-27.
Rhodes RE, Courneya K. Modelling the theory of planned behaviour and past behaviour. Psychol Health Med. 2003; 8: 57-69.
Rhodes RE, Courneya KS. Threshold assessment of attitude, subjective norm, and perceived behavioral control for predicting exercise intention and behavior. Psychol Sport Exerc. 2005; 6: 349-361.
Rhodes RE, Courneya KS, Blanchard CM, et al. Prediction of leisure-time walking: an integration of social cognitive, perceived environmental, and personality factors. Int J Behav Nutr Phys. 2007; 4: 51.
Rhodes R, de Bruijn GJ, Matheson DH. Habit in the physical activity domain: Integration with intention temporal stability and action control. J Sport Exercise Psychol. 2010; 32: 84-98.
Rhodes RE, Jones LW, Courneya KS. Extending the theory of planned behavior in the exercise domain: A comparison of social support and subjective norm. Res Q Exerc Sport. 2002; 73: 193-199.
Rhodes RE, Matheson DH. Discrepancies in exercise intention and expectation: Theoretical and applied issues. Psychol Health. 2005; 20: 63-78.
Rhodes RE, Matheson DH, Mark R. Evaluation of social cognitive scaling response options in the physical activity domain. Meas Phys Educ Exerc Sci. 2010; 14: 137-150.
Rise J, Kovac V, Kraft P, et al. Predicting the intention to quit smoking and quitting behaviour: Extending the theory of planned behaviour. Brit J Health Psychol. 2008; 13: 291-310.
Rivis A, Sheeran P. Social influences and the theory of planned behaviour: Evidence for a direct relationship between prototypes and young people’s exercise behaviour. Psychol Health. 2003; 18: 567-583.
Schutz M, Godin G, Vezina-Im L-A, et al. Determinants of condom use among HIV-positive men who have sex with men. Int J STD AIDS. 2011; 22: 391-397.
Scott EJ, Eves FF, French DP, et al. The theory of planned behaviour predicts self-reports of walking, but does not predict step count. Brit J Health Psychol. 2007; 12: 601-620.
Scott EJ, Eves FF, Hoppe R, et al. Dancing to a different tune: The predictive utility of the theory of planned behaviour when the behaviour is constrained. Psychol Sport Exerc. 2010; 11: 250-257.
Shankar A, Conner M, Bodansky HJ. Can the theory of planned behaviour predict maintenance of a frequently repeated behaviour? Psychol Health Med. 2007; 12: 213-224.
Sieverding M, Matterne U, Ciccarello L. What role do social norms play in the context of men’s cancer screening intention and behavior? Application of an extended theory of planned behavior. Health Psychol. 2010; 29: 72-81.
Victoir A, Eertmans A, Van den Bergh O, et al. Learning to drive safely: Social-cognitive responses are predictive of performance rated by novice drivers and their instructors. Transp Res F: Traffic Psychol Behav. 2005; 8: 59-74.
Wilkinson D, Abraham C. Constructing an integrated model of the antecedents of adolescent smoking. Brit J Health Psychol. 2004; 9: 315-333.
Woolfson LM, Maguire L. Binge drinking in a sample of Scottish undergraduate Students. J Youth Stud. 2010; 13: 647-659.
Rothman AJ, Salovey P. Shaping perceptions to motivate healthy behaviour: The role of message framing. Psychol Bull. 1997; 121: 3-19.
Borenstein M, Hedges LV, Higgins J, et al. Comprehensive meta-analysis version 2. Englewood, N.J.: Biostat; 2005.
Cochran WG. The χ2 test of goodness of fit. Ann Math Stat. 1952; 23: 315-345.
Higgins J, Thompson S, Deeks J, et al. Measuring inconsistency in meta-analysis. Brit Med J. 2003; 327: 557-560.
Rosenthal R. Meta-analytic procedures for social research. Beverly Hills, CA: Sage; 1984.
Egger M, Jüni P, Bartlett C, et al. How important are comprehensive literature searches and assessment of trial quality in systematic reviews? Empirical study. Health Technol Assess. 2003; 7(1): 1-76.
Duval S, Tweedie R. A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. J Am Stat Assoc. 2000; 95(449): 89-98.
Ajzen I. Martin Fishbein’s legacy: The reasoned action approach. Ann Am Acad Polit Soc Sci. 2012; 640(March): 11-27.
Conner M, Norman P, Bell R. The Theory of Planned Behavior and healthy eating. Health Psychol. 2002; 21: 194-201.
Cooke, R., Dahdah, M., Norman, P. How well does the theory of planned behaviour predict alcohol consumption? A systematic review and meta-analysis. Health Psychol Rev. http://dx.doi.org/10.1080/17437199.2014.947547
Bandura A. Self-efficacy: The exercise of control. New York: Freeman; 1997.
Maddux JE, Rogers RW. Protection motivation and self-efficacy: A revised theory of fear appeals and attitude change. J Exp Soc Psychol. 1983; 19: 469-479.
Williams DM. Outcome expectancy and self-efficacy: Theoretical implications of an unresolved contradiction. Personal Soc Psychol Rev. 2010; 14: 417-425.
Williams, D.M., Rhodes, R.E. The confounded self- efficacy construct: Conceptual analysis, and recommendations for future research. Health Psychol Rev. doi: 10.1080/17437199.2014.941998
Yzer M. Perceived behavioral control in reasoned action theory: A dual aspect interpretation. Ann Am Acad Polit Soc Sci. 2012; 640(March): 101-117.
Weinstein ND. Misleading tests of health behavior theories. Ann Behav Med. 2007; 33: 1-10.
Acknowledgments
The authors would like to thank Chandani Nekitsing for assistance in collating included studies and to the authors who provided additional information to allow their studies to be included.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
As a meta-analysis, no ethical approval was sought for this work.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
McEachan, R., Taylor, N., Harrison, R. et al. Meta-Analysis of the Reasoned Action Approach (RAA) to Understanding Health Behaviors. ann. behav. med. 50, 592–612 (2016). https://doi.org/10.1007/s12160-016-9798-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-016-9798-4