
Abstract
Purpose
The need of prophylactic central neck dissection (PCND) in patients with papillary thyroid carcinoma (PTC) is still controversial. The major restriction of PCND is the potential complications. We undertook a retrospective study to discuss its necessity in PTC patients.
Methods
A total of 188 patients with PTC who underwent total thyroidectomy and PCND were involved. In all of these, central lymph nodes were pathologic examined. Univariate and multivariate analyses were performed based on tumor location and size, etc.
Results
Overall, node metastases were found in 44.1 % (83/188) of patients. Tumor size was the independent positive predictor for lymph node metastasis, while gender, age, tumor multifocality, tumor location, and capsular infiltration were not independent predictors of central lymph node metastases. Postoperative complications happened in 5.3 % (10/188) of patients, which 4.8 % (9/188) had temporary hypocalcemia and 0 % (0/188) had permanent hypocalcemia. Rates of temporary and permanent recurrent laryngeal nerve injury were 0.5 % (1/188) and 0 % (0/188), respectively.
Conclusions
PCND is recommended in all patients with PTC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Thyroid carcinoma is the most common endocrine malignancy, which incidence increased in the last several decades. Papillary thyroid carcinoma (PTC) is the most common histological subtype, accounting for more than 85 % of all cases. The prognosis of PTC is general good, with 10-year survival rate exceeds 95 % and 20-year survival rate exceeds 93 % [1–5]. Despite its excellent outcomes, studies have showed that recurrence is an important factor increasing in morbidity and mortality, and cervical lymph node metastasis is most important variable known to increase the risk of local recurrence [6, 7].
It has been shown that cervical lymph node metastasis was found in 20–90 % of patients who undertook cervical lymph node dissection [8, 9]. Of theses, central lymph node metastasis is most common [10, 11]. For now, routinely performing a neck dissection in patients with clinically positive neck lymph nodes (cN+) has been a consensus. However, there is a controversy concerning the need and indications for a neck dissection in PTC patients showing clinically negative neck lymph nodes (cN0), which means prophylactic central neck dissection (PCND) [12–16].
The present study was a retrospective analysis of patients with cN0 PTC from the General Surgery department of Xinhua Hospital and from the Renji Hospital affiliated to Shanghai Jiaotong University School of Medicine in the past 3 years. Univariate and multivariate analyses were performed to assess the factors predicting for central lymph nodes metastases. Results may provide clues on the necessity of PCND and contribute to the improvement of PTC treatment.
Patients and methods
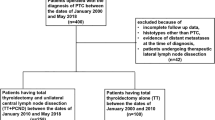
Subjects were selected according to the following criteria: (1) patients admitted for thyroid carcinoma in the General Surgery Department of Xinhua Hospital or in the Renji Hospital affiliated to Shanghai Jiao Tong University School of Medicine; (2) previously untreated patients; (3) surgical treatment was required for the primary tumor; (4) PTC diagnosed based on frozen paraffin sections; (5) PCND undertook in the same operating time after thyroidectomy; (6) lymph node metastases was not found clinically or radiologically prior to surgery (clinical N0/cN0); and (7) complete medical records were available for data extraction.
Following data were extracted from the medical records: gender, age at diagnosis, tumor size, tumor location, presence of local invasion, TNM classification, presence of central lymph node metastases, and postoperative complications.
TNM was assessed according to the 7th edition (2010) of the thyroid cancer TNM staging system from AJCC (American Joint Committee on Cancer)/UICC (International Federation of Cancer). The surgical procedure was followed according to NCCN practice guidelines. To the patients underwent total thyroidectomy we performed bilateral PCND, and to the patients underwent lobectomy the ipsilateral PCND was received.
Data collection was performed using Microsoft Excel (Redmond, WA, USA). Statistical analyses were performed using SAS 8.0 software (Cary, NC, USA). Student’s t test was used to compare normally distributed variables between groups. Non-normally distributed variables were analyzed using Wilcoxon’s rank test. Categorical variables were analyzed using the χ2 test or Fisher exact test. Multivariate analyses were conducted using unconditional logistic regression. Statistical significance was assumed when P < 0.05.
Results
A total of 188 patients were involved in the present study. All cases were confirmed as PTC using frozen paraffin sections. Table 1 shows patient demographics. For each patient, an average of three lymph nodes were obtained (range, 1–16, median = 3). Pathological examination showed that central lymph node metastases were found in 83 patients (83/188, 44.1 %).
Postoperative complications happened in 10 patients (10/188, 5.3 %), in which 9 (9/188, 4.8 %) had temporary hypocalcemia and 0 (0/188, 0 %) had permanent hypocalcemia. Rates of temporary and permanent recurrent laryngeal nerve injury were 0.5 % (1/188) and 0 % (0/188), respectively.
Table 2 shows the results of univariate analyses based on central lymph node metastasis. Results revealed that large tumor size (P = 0.04), disease affecting both lobes (P = 0.04), and multifocality (P = 0.02) were significantly positively associated to central lymph node metastasis.
Meanwhile, gender, age at diagnosis, tumor size, multifocality, tumor location, and capsular invasion were put in the logistic regression model. Results show that tumor size was independent predictive factor for central lymph node metastasis (Table 3).
Discussion
There is controversy in the application of PCND to the patients with PTC, which mainly focus on the balance of the potential benefits and the postoperative complications.
The benefits of PCND have become more and more clear. In our study, the positive nodes were found in 44.1 % of patients of PTC. Statistic analysis showed that the larger the tumor was, the more likely to find central lymph node metastasis, with the incidence of 35.1, 53.9, 47.1, and 100.0 % in tumor size of less than 1, 1–2, 2–4 cm, and lager than 4 cm, respectively. At the same time, tumor size was also an independent predictive factor for central lymph node metastases in cN0 PTC patients, with a positive correlation (correlation coefficient β = 1.2031, P = 0.004, OR = 3.330, 95 % CI = 1.474–7.525). These results consist with most reports. Ito et al. [14] also showed a positive correlation between tumor size and the incidence of central lymph node metastases, with the incidence of 38.3, 59.2, 73.7, and 79.0 % in tumor size of less than 1, 1–2, 2–4 cm, and lager than 4 cm, respectively. Roh et al. [12] using multivariate analyses reported that tumor size ≥1 cm was an independent factor for ipsilateral central lymph node metastases. Koo et al. [13] obtained the same results: either ipsilateral or contralateral lymph node metastases were more likely to occur in tumors >1 cm. However, a study by Kutler et al. [17] showed that tumor size had no significant impact on the presence of central lymph node metastases (P = 0.18). Generally, most researchers have had the consensus that the larger the tumor is, the more metastases may occurred.
This study also showed that both thyroid lobes had carcinoma would cause more nodal metastasis than one lobe, and multifocality of tumor would lead to higher incidence of metastasis than single tumor either.
As for the other factors such as patients’ age and gender, our results showed no significant difference in nodal metastasis. This consists with previously reported results [13, 17]. It means the application of PCND should not limited by patients age or gender.
Although not shown in this study, recent studies have shown that lymph node metastasis is related to increasing local recurrence and reducing survival rate. A large study have reported that mortality of PTC patients with nodal metastases was much greater than the patients without metastases. Thus to the patients with PTC, the benefits from PCND are obvious, the dissection can decrease local recurrence and increase the patient survival [6].
Another important reason to have PCND is that there is no other reliable method to verify central lymph node metastasis, whether preoperative or intraoperative ultrasound or other methods are far from sufficient sensitivity to verify the central lymph node metastasis [18]. Stulak et al. [19] showed in their study that in total of 511 patients with PTC, the clinical nodal negative patients were 476, in which preoperative ultrasound detected positive central lymph nodes in 10 patients (2.1 %) and positive cervical lymph nodes in 70 patients (14.4 %). But the truth was, the positive central lymph nodes were confirmed in 179 cases (32.5 %) and positive cervical lymph node was found in 86 cases (15.6 %). Kouvaraki et al. [9] showed that in 161 patients with preoperative ultrasonography, the positive central nodal incidence was 39.1 % (63/161), while the final pathological examination was proved to be 73.3 %, which implied false positive results in 2 (2/63) patients and 57 false negative results(57/98) of ultrasound examination. Therefore, before other reliable authentication methods arise, there is no better way to assess central lymph node metastasis other than PCND.
Furthermore, the results of PCND can help patients get clear staging after surgery, and subsequently take much more precise treatment. Explicit postoperative staging of patients with PTC can have following benefits of treatment: (1) to assess the prognosis; (2) to guide postoperative adjuvant therapy for individual programs, including 131I therapy and TSH suppressive therapy, which can reduce recurrence and mortality; (3) to determine the time and frequency of follow-up, which high-risk patients require intensive follow-up; (4) contribute to communication between physicians of patient information; and (5) staging system for clinical research can be used to assess the different groups of patients to different treatment [20, 21].
The main reason preventing us from taking PCND is the potential postoperative complications. As the increase in application of PCND, postoperative complications such as hypocalcemia, recurrent laryngeal nerve injury may increase [11, 22, 23] but as we have more experience, the incidence has been dropped obviously in the resent years [24–26]. Our study showed that the incidence of postoperative complications was 5.3 % (10/188); all of these were transient and no permanent complications, which included nine cases of hypocalcemia and one case of recurrent laryngeal nerve injury. But to the PTC patients who underwent recurrence, the reoperation for the treatment could be a total disaster. The disorders of structure would lead to much more severe complications and result in poor prognosis [27, 28].
In conclusion, the main reason stoping us taking PCND is the potential complications, but the data mentioned above have shown that after enough exercises, the incidence could be reduced to just like without PCND. Besides the high incidence of central lymph nodes metastasis in patients with PTC, the application of PCND will reduce tumor recurrence and patient’s mortality, and the pathological results of PCND will promote the follow-up treatment, we recommend PCND to all patients with PTC. But considering the good outcome of PTC and with the purpose to reduce complications as much as possible, we suggest that the prevention of complications should always be put to top priority in operation, which means during the surgery preference should be given to the removal of parts not leading to complications. After all, our purpose is to give patient better prognosis. In general, we recommend a compromised PCND to all patients with PTC, which means the PCND should compromise with the priority of low complication.
References
Brassard M, Borget I, Edet-Sanson A, Giraudet AL, Mundler O, Toubeau M, et al. Long-term follow-up of patients with papillary and follicular thyroid cancer: a prospective study on 715 patients. J Clin Endocrinol Metab. 2011;96:1352–9.
Nascimento C, Borget I, Al GA, Deandreis D, Chami L, Travagli JP, et al. Persistent disease and recurrence in differentiated thyroid cancer patients with undetectable postoperative stimulated thyroglobulin level. Endocr Relat Cancer. 2011;18:R29–40.
Sciuto R, Romano L, Rea S, Marandino F, Sperduti I, Maini CL. Natural history and clinical outcome of differentiated thyroid carcinoma: a retrospective analysis of 1503 patients treated at a single institution. Ann Oncol. 2009;20:1728–35.
Toniato A, Boschin I, Casara D, Mazzarotto R, Rubello D, Pelizzo M. Papillary thyroid carcinoma: factors influencing recurrence and survival. Ann Surg Oncol. 2008;15:1518–22.
Chow SM, Law SC, Chan JK, Au SK, Yau S, Lau WH. Papillary microcarcinoma of the thyroid-Prognostic significance of lymph node metastasis and multifocality. Cancer. 2003;98:31–40.
Podnos YD, Smith D, Wagman LD, Ellenhorn JD. The implication of lymph node metastasis on survival in patients with well-differentiated thyroid cancer. Am Surg. 2005;71:731–4.
Burns WR, Zeiger MA. Differentiated thyroid cancer. Semin Oncol. 2010;37:557–66.
Grebe SK, Hay ID. Thyroid cancer nodal metastases: biologic significance and therapeutic considerations. Surg Oncol Clin N Am. 1996;5:43–63.
Kouvaraki MA, Shapiro SE, Fornage BD, Edeiken-Monro BS, Sherman SI, Vassilopoulou-Sellin R, et al. Role of preoperative ultrasonography in the surgical management of patients with thyroid cancer. Surgery. 2003;134:946–54 discussion 954–5.
Robbins KT, Shaha AR, Medina JE, Califano JA, Wolf GT, Ferlito A, et al. Consensus statement on the classification and terminology of neck dissection. Arch Otolaryngol Head Neck Surg. 2008;134:536–8.
Roh JL, Kim JM, Park CI. Central compartment reoperation for recurrent/persistent differentiated thyroid cancer: patterns of recurrence, morbidity, and prediction of postoperative hypocalcemia. Ann Surg Oncol. 2011;18:1312–8.
Roh JL, Kim JM, Park CI. Central lymph node metastasis of unilateral papillary thyroid carcinoma: patterns and factors predictive of nodal metastasis, morbidity, and recurrence. Ann Surg Oncol. 2011;18:2245–50.
Koo BS, Choi EC, Yoon YH, Kim DH, Kim EH, Lim YC. Predictive factors for ipsilateral or contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma. Ann Surg. 2009;249:840–4.
Ito Y, Jikuzono T, Higashiyama T, Asahi S, Tomoda C, Takamura Y, et al. Clinical significance of lymph node metastasis of thyroid papillary carcinoma located in one lobe. World J Surg. 2006;30:1821–8.
Son YI, Jeong HS, Baek CH, Chung MK, Ryu J, Chung JH, et al. Extent of prophylactic lymph node dissection in the central neck area of the patients with papillary thyroid carcinoma: comparison of limited versus comprehensive lymph node dissection in a 2-year safety study. Ann Surg Oncol. 2008;15:2020–6.
Takami H, Ito Y, Okamoto T, Yoshida A. Therapeutic strategy for differentiated thyroid carcinoma in Japan based on a newly established guideline managed by Japanese Society of Thyroid Surgeons and Japanese Association of Endocrine Surgeons. World J Surg. 2011;35:111–21.
Kutler DI, Crummey AD, Kuhel WI. Routine central compartment lymph node dissection for patients with papillary thyroid carcinoma. Head Neck. 2012;34:260–3.
Marshall CL, Lee JE, Xing Y, Perrier ND, Edeiken BS, Evans DB, et al. Routine pre-operative ultrasonography for papillary thyroid cancer: effects on cervical recurrence. Surgery. 2009;146:1063–72.
Stulak JM, Grant CS, Farley DR, Thompson GB, van Heerden JA, Hay ID, et al. Value of preoperative ultrasonography in the surgical management of initial and reoperative papillary thyroid cancer. Arch Surg. 2006;141:489–94 discussion 494–6.
Bonnet S, Hartl D, Leboulleux S, Baudin E, Lumbroso JD, Al GA, et al. Prophylactic lymph node dissection for papillary thyroid cancer less than 2 cm: implications for radioiodine treatment. J Clin Endocrinol Metab. 2009;94:1162–7.
Hughes DT, White ML, Miller BS, Gauger PG, Burney RE, Doherty GM. Influence of prophylactic central lymph node dissection on postoperative thyroglobulin levels and radioiodine treatment in papillary thyroid cancer. Surgery. 2010;148:1100–6 discussion 1006–7.
Roh JL, Park JY, Park CI. Total thyroidectomy plus neck dissection in differentiated papillary thyroid carcinoma patients: pattern of nodal metastasis, morbidity, recurrence, and postoperative levels of serum parathyroid hormone. Ann Surg. 2007;245:604–10.
Shen WT, Ogawa L, Ruan D, Suh I, Duh QY, Clark OH. Central neck lymph node dissection for papillary thyroid cancer: the reliability of surgeon judgment in predicting which patients will benefit. Surgery. 2010;148:398–403.
Moo TA, Umunna B, Kato M, Butriago D, Kundel A, Lee JA, et al. Ipsilateral versus bilateral central neck lymph node dissection in papillary thyroid carcinoma. Ann Surg. 2009;250:403–8.
Sadowski BM, Snyder SK, Lairmore TC. Routine bilateral central lymph node clearance for papillary thyroid cancer. Surgery. 2009;146:696–703 discussion 703–5.
Palestini N, Borasi A, Cestino L, Freddi M, Odasso C, Robecchi A. Is central neck dissection a safe procedure in the treatment of papillary thyroid cancer? Our experience. Langenbecks Arch Surg. 2008;393:693–8.
Moley JF, Lairmore TC, Doherty GM, Brunt LM, DeBenedetti MK. Preservation of the recurrent laryngeal nerves in thyroid and parathyroid reoperations. Surgery. 1999;126:673–7 discussion 677–9.
Kim MK, Mandel SH, Baloch Z, Livolsi VA, Langer JE, Didonato L, et al. Morbidity following central compartment reoperation for recurrent or persistent thyroid cancer. Arch Otolaryngol Head Neck Surg. 2004;130:1214–6.
Conflict of interest
The authors have no conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Additional information
Q. Wang and B. Chu contributed equally to this work.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Wang, Q., Chu, B., Zhu, J. et al. Clinical analysis of prophylactic central neck dissection for papillary thyroid carcinoma. Clin Transl Oncol 16, 44–48 (2014). https://doi.org/10.1007/s12094-013-1038-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-013-1038-9