
Abstract
Background
Optimal resuscitation after traumatic brain injury (TBI) remains uncertain. We hypothesize that cerebral metabolic crisis is frequent despite adequate resuscitation of the TBI patient and that metabolic crisis negatively influences outcome.
Methods
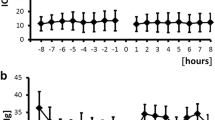
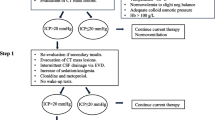
We assessed the effectiveness of a standardized trauma resuscitation protocol in 89 patients with moderate to severe TBI, and determined the frequency of adequate resuscitation. Prospective hourly values of heart rate, blood pressure, pulse oximetry, intracranial pressure (ICP), respiratory rate, jugular venous oximetry, and brain extracellular values of glucose, lactate, pyruvate, glycerol, and glutamate were obtained. The incidence during the initial 72 h after injury of low brain glucose <0.8 mmol/L, elevated lactate/pyruvate ratio (LPR) >25, and metabolic crisis, defined as the simultaneous occurrence of both low glucose and high LPR, were determined for the group.
Results
5 patients were inadequately resuscitated and eight patients had intractable ICP. In patients with successful resuscitation and controlled ICP (n = 76), within 72 h of trauma, 76 % had low glucose, 93 % had elevated LPR, and 74 % were in metabolic crisis. The duration of metabolic crisis was longer in those patients with unfavorable (GOSe ≤ 6) versus favorable (GOSe ≥ 7) outcome at 6 months (P = 0.011). In four multivariate models the burden of metabolic crisis was a powerful independent predictor of poor outcome.
Conclusions
Metabolic crisis occurs frequently after TBI despite adequate resuscitation and controlled ICP, and is a strong independent predictor of poor outcome at 6 months.

Similar content being viewed by others

References
Bhardwaj A, Mirski MA, editors. Handbook of Neurocritical Care: Second Edition. doi:10.1007/978-1-4419-6842-5_18, © Springer Science+Business Media, LLC 2011.
Hesdorffer DC, Ghajar J. Marked improvement in adherence to traumatic brain injury guidelines in United States trauma centers. J Trauma. 2007;63:841–8.
Chesnut RM, Marshall LF, Klauber MR, et al. The role of secondary brain injury in determining outcome from severe head injury. J Trauma. 1993;34:216–22.
McHugh GS, Engel DC, Butcher I, Steyerberg EW, Lu J, Mushkudiani N, et al. Prognostic value of secondary insults in traumatic brain injury: results from the IMPACT study. J Neurotrauma. 2007;24:287–93.
Stiefel MF, Udouteuk JD, Spiotta AM, Gracias VH, Golberg A, Maloney-Wilensky E, Bloom S, Le Roux PD. Conventional neurocritical care and cerebral oxygenation after traumatic brain injury. J Neurosurg. 2006;105:568–75.
Fletcher JJ, Bergman K, Bolstein PA, Kramer AH. Fluid balance, complications, and brain tissue oxygen tension monitoring following severe traumatic brain injury. Neurocrit Care. 2010;13(1):47–56.
Xu Y, McArthur D, Alger J, Etchepare M, Hovda D, Glenn T, Huang S, Dinov I, Vespa P. Early nonischemic oxidative metabolic dysfunction leads to chronic brain atrophy in traumatic brain injury. J Cereb Blood Flow Metab. 2010;30:883–94.
Vespa PM, Lakshmanan R, Loo JA, Drake T, Leblanc J, Ytternerg AJ, McArthur DL, Etchepare M. Metabolic crisis after traumatic brain injury is associated with a novel microdialysis proteome. Neurocrit Care. 2010;12:324–36.
Reinstrup P, Stahl N, Mellergard P, Uski T, Ungerstedt U, Nordstrom CH. Intracerebral microdialysis in clinical practice: baseline values for chemical markers during wakefulness, anesthesia, and neurosurgery. Neurosurgery. 2000;47:701–9.
Vespa PM, Bergsneider M, Hattori N, Wu HM, Huang SC, Martin NA, et al. Metabolic crisis without brain ischemia is common after traumatic brain injury: a combined microdialysis and positron emission tomography study. J Cereb Blood Flow Metab. 2005;25:763–74.
Marcoux J, McArthur D, Miller C, Glenn T, Villablanca P, Martin N, Hovda D, Alger J. Vespa Persistent metabolic crisis as measured by elevated cerebral microdialysis lactate-pyruvate ratio predicts chronic frontal love brain atrophy after traumatic brain injury. Crit Care Med. 2008;36:2871–7.
Hutchinson PJ, Timofeev I, Carpenter KL, Nortje J, Al-Rawi PG, O’Connell MT, Czosnyka M, Smielewski P, Pickard JD, Menon DK, Kirkpatrick PJ, Gupta AK. Cerebral extracellular chemistry and outcome following traumatic brain injury: a microdialysis study of 223 patients. Brain. 2011;134:484–94.
Vespa PM, O’Phelan K, McArthur D, Miller C, Eliseo M, Hirt D, et al. Pericontusional brain tissue exhibits persistent elevation of lactate/pyruvate ratio independent of cerebral perfusion pressure. Crit Care Med. 2007;35:1153–60.
Vespa PM, McArthur DL, O’Phelan K, Glenn T, Etchepare M, Kelly D, Bergsneider M, Martin N, Hovda D. Persistently low extracellular glucose correlates with poor outcome 6 months after human traumatic brain injury despite a lack of increased lactate: a microdialysis study. J Cereb Blood Flow Metab. 2003;23:865–77.
David J Dries, MD, MSE, FACS, FCCP, FCCM. Initial evaluation of the trauma patient. 2011. http://emedicine.medscape.com/article/434707-overview. Accessed 1 Sep 2011.
Brain Trauma Foundation. Guidelines for the management of severe traumatic brain injury, 3rd ed. J Neurotrauma. 2007;24(Suppl 1):S7–13.
Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators. Canadian Critical Care Trials Group. N Engl J Med. 1999;340(6):409–17.
Clifton GL, Miller ER, Choi SC, Levin HS. Fluid thresholds and outcome from severe brain injury. Crit Care Med. 2002;30(4):739–45.
Lam TS, Mak PSK, Siu WS, Lam MY, Cheung TF, Rainer TH. Validation of a Modified Early Warning Score (MEWS) in emergency department observation ward patients. Hong Kong J Emerg Med. 2006;13:24–30.
Wilcox R, Schoendbrodt F. Robust Statistics. 2012. http://dornsife.usc.edu/labs/rwilcox/software/index.cfm. Accessed 6 Mar 2012.
Wilcox R. Introduction to robust estimatino and hypothesis testing. 2nd ed. New York: Elsevier Inc; 2005.
Agostinelli C. wle: Weighted Likelihood Estimation. R package version 0.9-4. 2010. http://CRAN.R-project.org/package=wle. Accessed 6 Mar 2012.
Saatman KE, Duhaime A, Bullock R, Maas A, Valadka A, Manley GT. Classification of traumatic brain injury for targeted therapies. J Neurotrauma. 2008;25:719–38.
Sander A. The Extended Glasgow Outcome Scale. The Center for Outcome Measurement in Brain Injury. 2002. http://www.tbims.org/combi/gose. Accessed 30 Mar 2012.
Vespa PM, Nuwer MR, Nenov V, Ronne-Engstrom E, Hovda DA, Bergsneider M, Kelly DF, Martin NA, Becker DP. Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring. J Neurosurg. 1999;91:750–60.
Vespa PM, McArthur DL, Xu Y, Eliseo M, Etchepare M, Dinov I, Alger J, Glenn TP, Hovda D. Nonconvulsive seizures after traumatic brain injury are associated with hippocampal atrophy. Neurology. 2010;75:792–8.
Menon DK, Coles JP, Gupta AK, Fryer TD, Smielewski P, Chatfield DA, Aigbirhio F, Skepper JN, Minhas PS, Hutchinson PJ, Carpenter TA, Clark JC, Pickard JD. Diffusion limited oxygen delivery following head injury. Crit Care Med. 2004;32:1384–90.
Acknowledgments
UCLA Brain Injury Research Center, supported by NS-058489.
Conflict of interest
No commercial company conflicts of interest to report.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Stein, N.R., McArthur, D.L., Etchepare, M. et al. Early Cerebral Metabolic Crisis After TBI Influences Outcome Despite Adequate Hemodynamic Resuscitation. Neurocrit Care 17, 49–57 (2012). https://doi.org/10.1007/s12028-012-9708-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-012-9708-y