
Abstract
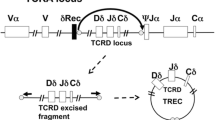
Newborn screening (NBS) programs for severe combined immunodeficiency (SCID), using the TREC-based assay, have enabled early diagnosis, prompt treatment, and eventually changed the natural history of affected infants. Nevertheless, it was believed that some affected infants with residual T cell, such as patients with MHC II deficiency, will be misdiagnosed by this assay. A full immune workup and genetic analysis using direct Sanger sequencing and whole exome sequencing have been performed to a patient that was identified by the Israeli NBS program for SCID. The patient was found to have severe CD4 lymphopenia with an inverted CD4/CD8 ratio, low TREC levels in peripheral blood, abnormal response to mitogen stimulation, and a skewed T cell receptor repertoire. HLA-DR expression on peripheral blood lymphocytes was undetectable suggesting a diagnosis of MHC II deficiency. Direct sequencing of the RFX5 gene revealed a stop codon change (p. R239X, c. C715T), which could cause the patient’s immune phenotype. His parents were found to be heterozygote carriers for the mutation. Whole exome sequencing could not identify other potential mutations to explain his immunodeficiency. The patient underwent successful conditioned hematopoietic stem cell transplantation from healthy matched unrelated donor and is currently well and alive with full chimerism. Infants with MHC class II deficiency can potentially be identified by the TREC-based assay NBS for SCID. Therefore, MHC II molecules (e.g., HLA-DR) measurement should be part of the confirmatory immune-phenotyping for patients with positive screening results. This will make the diagnosis of such patients straightforward.


Similar content being viewed by others

Abbreviations
- HSCT:
-
Hematopoietic stem cell transplantation
- MHC:
-
Major histocompatibility complex
- NBS:
-
Newborn screening
- SCID:
-
Severe combined immunodeficiency
- TCR:
-
T cell receptor
- TRECs:
-
T cell receptor excision circles
References
Dorsey MJ, Dvorak CC, Cowan MJ, Puck JM. Treatment of infants identified as having severe combined immunodeficiency by means of newborn screening. J Allergy Clin Immunol. 2017;139(3):733–42.
Rechavi E, Lev A, Simon AJ, Stauber T, Daas S, Saraf-Levy T, et al. First year of israeli newborn screening for severe combined immunodeficiency-clinical achievements and insights. Front Immunol. 2017;8:1448. https://doi.org/10.3389/fimmu.2017.
King JR, Hammarström L. Newborn screening for primary immunodeficiency diseases: history, current and future practice. J Clin Immunol. 2018 Jan;38(1):56–66.
Amariglio N, Lev A, Simon A, Rosenthal E, Spirer Z, Efrati O, et al. Molecular assessment of thymus capabilities in the evaluation of T-cell immunodeficiency. Pediatr Res. 2010;67(2):211–6.
Dar N, Gothelf D, Korn D, Frisch A, Weizman A, Michaelovsky E, et al. Thymic and bone marrow output in individuals with 22q11.2 deletion syndrome. Pediatr Res. 2015;77(4):579–85.
Kraus M, Lev A, Simon AJ, Levran I, Nissenkorn A, Levi YB, et al. Disturbed B and T cell homeostasis and neogenesis in patients with ataxia telangiectasia. J Clin Immunol. 2014;34(5):561–72.
Lev A, Simon AJ, Bareket M, Bielorai B, Hutt D, Amariglio N, et al. The kinetics of early T and B cell immune recovery after bone marrow transplantation in RAG-2-deficient SCID patients. PLoS One. 2012;7(1):e30494.
Albin-Leeds S, Ochoa J, Mehta H, Vogel BH, Caggana M, Bonagura V, et al. Idiopathic T cell lymphopenia identified in New York State newborn screening. Clin Immunol. 2017;183:36–40.
Kwan A, Abraham RS, Currier R, Brower A, Andruszewski K, Abbott JK, et al. Newborn screening for severe combined immunodeficiency in 11 screening programs in the United States. JAMA. 2014;312(7):729–38.
Jyonouchi S, Jongco AM, Puck J, Sullivan KE. Immunodeficiencies associated with abnormal newborn screening for T cell and B cell lymphopenia. J Clin Immunol. 2017;37(4):363–74.
Kwan A, Church JA, Cowan MJ, Agarwal R, Kapoor N, Kohn DB, et al. Newborn screening for severe combined immunodeficiency and T-cell lymphopenia in California: results of the first 2 years. J Allergy Clin Immunol. 2013;132(1):140–50.
Somech R. T-cell receptor excision circles in primary immunodeficiencies and other T-cell immune disorders. Curr Opin Allergy Clin Immunol. 2011;11(6):517–24.
Roifman CM, Somech R, Kavadas F, Pires L, Nahum A, Dalal I, et al. Defining combined immunodeficiency. J Allergy Clin Immunol. 2012;130(1):177–83.
Lev A, Simon AJ, Broides A, Levi J, Garty BZ, Rosenthal E, et al. Thymic function in MHC class II-deficient patients. J Allergy Clin Immunol. 2013;131(3):831–9.
Kuo CY, Chase J, Garcia Lloret M, Stiehm ER, Moore T, Aguilera MJ, et al. Newborn screening for severe combined immunodeficiency does not identify bare lymphocyte syndrome. J Allergy Clin Immunol. 2013;131(6):1693–5.
Lyttle A, Roifman CM, Dadi H, Wright N, Kavadas F. MHC class II deficiency in the Dene native population: a case report highlighting pitfalls in diagnosis and treatment. Allergy Asthma Clin Immunol. 2014;10(Suppl 1):A1.
Picard C, Fischer A. Hematopoietic stem cell transplantation and other management strategies for MHC class II deficiency. Immunol Allergy Clin North Am. 2010;30(2):173–8.
Hanna S, Etzioni A. MHC class I and II deficiencies. J Allergy Clin Immunol. 2014;134(2):269–75.
Aluri J, Gupta M, Dalvi A, Mhatre S, Kulkarni M, Hule G, et al. Clinical, immunological, and molecular findings in five patients with major histocompatibility complex class II deficiency from India. Front Immunol. 2018;9:188.
Klein C, Cavazzana-Calvo M, Le Deist F, Jabado N, Benkerrou M, Blanche S, et al. Bone marrow transplantation in major histocompatibility complex class II deficiency: a single-center study of 19 patients. Blood. 1995;85(2):580–7.
Al-Mousa H, Al-Shammari Z, Al-Ghonaium A, Al-Dhekri H, Al-Muhsen S, Al-Saud B, et al. Allogeneic stem cell transplantation using myeloablative and reduced-intensity conditioning in patients with major histocompatibility complex class II deficiency. Biol Blood Marrow Transplant. 2010;16(6):818–23.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Marcus, N., Stauber, T., Lev, A. et al. MHC II deficient infant identified by newborn screening program for SCID. Immunol Res 66, 537–542 (2018). https://doi.org/10.1007/s12026-018-9019-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12026-018-9019-2