
Abstract
Background
Although knee osteoarthritis (OA) is common, its etiology is poorly understood. Specifically, it is not known whether knee OA is associated with abnormal anthropometric and musculoskeletal characteristics known to be associated with OA in general. We recently studied this topic for patients with hip arthritis; however, it is important to evaluate it for knee OA separately, because there are reports indicating that patients with primary OA in different joints may have a different phenotype.
Questions/purposes
Do patients with primary knee OA have a phenotype with higher bone mineral density (BMD), higher body mass index (BMI), larger skeletal size, lower lean body mass, and higher fat content?
Methods
We included 38 women and 74 men (mean age, 61 years; range, 34–85 years) with primary knee OA and 122 women and 121 men as control subjects. We used dual-energy x-ray absorptiometry to measure total body BMD (g/cm2), femoral neck width (cm), fat and lean mass (%), and BMI (kg/m2). Z scores were calculated for each individual. Data are presented as means with 95% confidence intervals.
Results
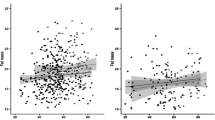
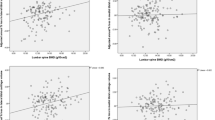
Women with knee OA had the following Z scores: total body BMD 0.8 (0.5–1.0); BMI 1.6 (1.1–2.0); femoral neck width 0.1 (–0.3 to 0.4); proportion of lean mass –1.0 (–1.5 to –0.6); and proportion of fat mass 1.0 (0.6–1.4). Men with knee OA had the following Z scores: total body BMD 0.5 (0.3–0.7); BMI 0.9 (0.6–1.1); femoral neck width 0.3 (0.1–0.7); proportion of lean mass –0.9 (–1.1 to –0.8); and proportion of fat mass 0.7 (0.5–0.9).
Conclusions
Women and men with idiopathic knee OA have a phenotype with higher BMD, higher BMI, proportionally higher fat mass, and proportionally lower lean body mass. Men also have a larger skeletal size.
Clinical Relevance
A higher BMD may lead to stiffer bone, a higher BMI to a greater joint load, and a proportionally lower lean body (muscle) mass to lower joint-protective ability, and all trait deviations probably predispose for knee OA.
Similar content being viewed by others

References
Alwis G, Karlsson C, Stenevi-Lundgren S, Rosengren BE, Karlsson MK. Femoral neck bone strength estimated by hip structural analysis (HSA) in Swedish Caucasians aged 6-90 years. Calcif Tissue Int. 2012;90:174–185.
Beck TJ, Ruff CB, Warden KE, Scott WW Jr, Rao GU. Predicting femoral neck strength from bone mineral data. A structural approach. Invest Radiol. 1990;25:6–18.
Bergink AP, Uitterlinden AG, Van Leeuwen JP, Hofman A, Verhaar JA, Pols HA. Bone mineral density and vertebral fracture history are associated with incident and progressive radiographic knee osteoarthritis in elderly men and women: the Rotterdam Study. Bone. 2005;37:446–456.
Blagojevic M, Jinks C, Jeffery A, Jordan KP. Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and meta-analysis. Osteoarthritis Cartilage. 2010;18:24–33.
Buckwalter JA, Saltzman C, Brown T. The impact of osteoarthritis: implications for research. Clin Orthop Relat Res. 2004;427(Suppl):S6–15.
Chaganti RK, Parimi N, Lang T, Orwoll E, Stefanick ML, Nevitt M, Lane NE. Bone mineral density and prevalent osteoarthritis of the hip in older men for the Osteoporotic Fractures in Men (MrOS) Study Group. Osteoporos Int. 2010;21:1307–1316.
Cicuttini FM, Baker JR, Spector TD. The association of obesity with osteoarthritis of the hand and knee in women: a twin study. J Rheumatol. 1996;23:1221–1226.
Cöster M, Rosengren EB, Magnusson H, Brudin L, M. KK. Bone mass and anthropometry in patients with osteoarthritis of the foot and ankle Foot Ankle Surg. 2014;20 52–56.
Dequeker J, Johnell O. Osteoarthritis protects against femoral neck fracture: the MEDOS study experience. Bone. 1993;14(Suppl 1):S51–56.
Dieppe PA, Lohmander LS. Pathogenesis and management of pain in osteoarthritis. Lancet. 2005;365:965–973.
Felson DT, Lawrence RC, Dieppe PA, Hirsch R, Helmick CG, Jordan JM, Kington RS, Lane NE, Nevitt MC, Zhang Y, Sowers M, McAlindon T, Spector TD, Poole AR, Yanovski SZ, Ateshian G, Sharma L, Buckwalter JA, Brandt KD, Fries JF. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann Intern Med. 2000;133:635–646.
Gupta KB, Duryea J, Weissman BN. Radiographic evaluation of osteoarthritis. Radiol Clin North Am. 2004;42:11–41, v.
Haugen IK, Slatkowsky-Christensen B, Orstavik R, Kvien TK. Bone mineral density in patients with hand osteoarthritis compared to population controls and patients with rheumatoid arthritis. Ann Rheum Dis. 2007;66:1594–1598.
Hilding M, Aspenberg P. Local peroperative treatment with a bisphosphonate improves the fixation of total knee prostheses: a randomized, double-blind radiostereometric study of 50 patients. Acta Orthop. 2007;78:795–799.
Jarvholm B, Lewold S, Malchau H, Vingard E. Age, bodyweight, smoking habits and the risk of severe osteoarthritis in the hip and knee in men. Eur J Epidemiol. 2005;20:537–542.
Karlsson MK, Gardsell P, Johnell O, Nilsson BE, Akesson K, Obrant KJ. Bone mineral normative data in Malmo, Sweden. Comparison with reference data and hip fracture incidence in other ethnic groups. Acta Orthop Scand. 1993;64:168–172.
Karlsson MK, Magnusson H, Coster MC, Vonschewelov T, Karlsson C, Rosengren BE. Patients With hip osteoarthritis have a phenotype with high bone mass and low lean body mass. Clin Orthop Relat Res. 2014;472:1224–1229.
Lang TF. The bone-muscle relationship in men and women. J Osteoporos. 2011;2011:702735.
Lee JH, Park JW, Shin YH. The insertional torque of a pedicle screw has a positive correlation with bone mineral density in posterior lumbar pedicle screw fixation. J Bone Joint Surg Br. 2012;94:93–97.
Lingard EA, Mitchell SY, Francis RM, Rawlings D, Peaston R, Birrell FN, McCaskie AW. The prevalence of osteoporosis in patients with severe hip and knee osteoarthritis awaiting joint arthroplasty. Age Ageing. 2010;39:234–239.
Lohmander LS, Gerhardsson de Verdier M, Rollof J, Nilsson PM, Engstrom G. Incidence of severe knee and hip osteoarthritis in relation to different measures of body mass: a population-based prospective cohort study. Ann Rheum Dis. 2009;68:490–496.
Montgomery MM, Shultz SJ, Schmitz RJ, Wideman L, Henson RA. Influence of lean body mass and strength on landing energetics. Med Sci Sports Exerc. 2012;44:2376–2383.
Nevitt MC, Zhang Y, Javaid MK, Neogi T, Curtis JR, Niu J, McCulloch CE, Segal NA, Felson DT. High systemic bone mineral density increases the risk of incident knee OA and joint space narrowing, but not radiographic progression of existing knee OA: the MOST study. Ann Rheum Dis. 2010;69:163–168.
Pereira D, Peleteiro B, Araujo J, Branco J, Santos RA, Ramos E. The effect of osteoarthritis definition on prevalence and incidence estimates: a systematic review. Osteoarthritis Cartilage. 2011;19:1270–1285.
Radin EL, Rose RM. Role of subchondral bone in the initiation and progression of cartilage damage. Clin Orthop Relat Res. 1986;213:34–40.
Reijman M, Pols HA, Bergink AP, Hazes JM, Belo JN, Lievense AM, Bierma-Zeinstra SM. Body mass index associated with onset and progression of osteoarthritis of the knee but not of the hip: the Rotterdam Study. Ann Rheum Dis. 2007;66:158–162.
Sowers M. Epidemiology of risk factors for osteoarthritis: systemic factors. Curr Opin Rheumatol. 2001;13:447–451.
Sridhar MS, Jarrett CD, Xerogeanes JW, Labib SA. Obesity and symptomatic osteoarthritis of the knee. J Bone Joint Surg Br. 2012;94:433–440.
Thorlund JB, Aagaard P, Roos EM. Muscle strength and functional performance in patients at high risk of knee osteoarthritis: a follow-up study. Knee Surg Sports Traumatol Arthrosc. 2012;20:1110–1117.
van Saase JL, van Romunde LK, Cats A, Vandenbroucke JP, Valkenburg HA. Epidemiology of osteoarthritis: Zoetermeer survey. Comparison of radiological osteoarthritis in a Dutch population with that in 10 other populations. Ann Rheum Dis. 1989;48:271–280.
van Saase JL, Vandenbroucke JP, van Romunde LK, Valkenburg HA. Osteoarthritis and obesity in the general population. A relationship calling for an explanation. J Rheumatol. 1988;15:1152–1158.
Wilder FV, Barrett JP, Farina EJ. The association of radiographic foot osteoarthritis and radiographic osteoarthritis at other sites. Osteoarthritis Cartilage. 2005;13:211–215.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article

Cite this article
Karlsson, M.K., Magnusson, H., Cöster, M. et al. Patients With Knee Osteoarthritis Have a Phenotype With Higher Bone Mass, Higher Fat Mass, and Lower Lean Body Mass. Clin Orthop Relat Res 473, 258–264 (2015). https://doi.org/10.1007/s11999-014-3973-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-014-3973-3