
Abstract
Background
While it is accepted accurate identification of infecting organisms is crucial in guiding treatment of periprosthetic joint infection (PJI), there remains no consensus regarding the best method for obtaining cultures.
Questions/purposes
We compared the yield of intraoperative tissue samples versus swab cultures in diagnosing PJI.
Methods
Tissue and swab cultures (three each) were collected prospectively during a consecutive series of 156 aseptic and septic revision arthroplasties from October 2011 to April 2012. The tissues and swabs were taken from standardized regions of the joint. After excluding 39 reimplantation procedures, we included 117 cases (74 hip, 43 knee; 30 septic, 87 aseptic) for analysis. We used a modified version of the Musculoskeletal Infection Society criteria for defining PJI, requiring three of five rather than four of six criteria. Tissue and swab cultures from septic and aseptic cases were used to calculate their sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for identifying PJI.
Results
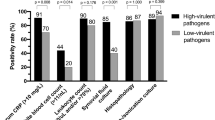
Tissue cultures were positive in a higher percentage of septic cases than swab cultures: 28 of 30 (93%) versus 21 of 30 (70%). Tissue cultures were positive in two of 87 aseptic cases (2%), while swab cultures were positive in 10 of 87 (12%). The sensitivity, specificity, PPV, and NPV were 93%, 98%, 93%, and 98%, respectively, for tissue cultures and 70%, 89%, 68%, and 90%, respectively, for swab cultures.
Conclusions
Tissue cultures demonstrated higher sensitivity, specificity, PPV, and NPV for diagnosing PJI than swab cultures. Swab cultures had more false-negative and false-positive results than tissue cultures. Because swab cultures pose a higher risk of not identifying or incorrectly identifying infecting organisms in PJI, we believe their use in obtaining intraoperative culture specimens should be discouraged.
Level of Evidence
Level II, diagnostic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


References
Achermann Y, Vogt M, Leunig M, Wüst J, Trampuz A. Improved diagnosis of periprosthetic joint infection by multiplex PCR of sonication fluid from removed implants. J Clin Microbiol. 2010;48:1208–1214.
Atkins BL, Athanasou N, Deeks JJ, Crook DW, Simpson H, Peto TE, McLardy-Smith P, Berendt AR. Prospective evaluation of criteria for microbiological diagnosis of prosthetic-joint infection at revision arthroplasty. The OSIRIS Collaborative Study Group. J Clin Microbiol. 1998;36:2932–2939.
Bedair H, Ting N, Jacovides C, Saxena A, Moric M, Parvizi J, Della Valle CJ. The Mark Coventry Award. Diagnosis of early postoperative TKA infection using synovial fluid analysis. Clin Orthop Relat Res. 2011;469:34–40.
Costerton JW. Biofilm theory can guide the treatment of device-related orthopaedic infections. Clin Orthop Relat Res. 2005;437:7–11.
Dy Chua J, Abdul-Karim A, Mawhorter S, Procop GW, Tchou P, Niebauer M, Saliba W, Schweikert R, Wilkoff BL. The role of swab and tissue culture in the diagnosis of implantable cardiac device infection. Pacing Clin Electrophysiol. 2005;28:1276–1281.
Font-Vizcarra L, García S, Martínez-Pastor JC, Sierra JM, Soriano A. Blood culture flasks for culturing synovial fluid in prosthetic joint infections. Clin Orthop Relat Res. 2010;468:2238–2243.
Gomez E, Cazanave C, Cunningham SA, Greenwood-Quaintance KE, Steckelberg JM, Uhl JR, Hanssen AD, Karau MJ, Schmidt SM, Osmon DR, Berbari EF, Mandrekar J, Patel R. Prosthetic joint infection diagnosis using broad-range PCR of biofilms dislodged from knee and hip arthroplasty surfaces using sonication. J Clin Microbiol. 2012;50:3501–3508.
Helstad AG, Kimball JL, Maki DG. Recovery of anaerobic, facultative, and aerobic bacteria from clinical specimens in three anaerobic transport systems. J Clin Microbiol. 1977;5:564–569.
Koyonos L, Zmistowski B, Della Valle CJ, Parvizi J. Infection control rate of irrigation and débridement for periprosthetic joint infection. Clin Orthop Relat Res. 2011;469:3043–3048.
Malhotra R, Morgan DA. Role of core biopsy in diagnosing infection before revision hip arthroplasty. J Arthroplasty. 2004;19:78–87.
Nelson CL, McLaren AC, McLaren SG, Johnson JW, Smeltzer MS. Is aseptic loosening truly aseptic? Clin Orthop Relat Res. 2005;437:25–30.
Neut D, van Horn JR, van Kooten TG, van der Mei HC, Busscher HJ. Detection of biomaterial-associated infections in orthopaedic joint implants. Clin Orthop Relat Res. 2003;413:261–268.
Pandey R, Berendt AR, Athanasou NA. Histological and microbiological findings in non-infected and infected revision arthroplasty tissues. The OSIRIS Collaborative Study Group. Oxford Skeletal Infection Research and Intervention Service. Arch Orthop Trauma Surg. 2000;120:570–574.
Parvizi J, Della Valle CJ. AAOS Clinical Practice Guideline: diagnosis and treatment of periprosthetic joint infections of the hip and knee. J Am Acad Orthop Surg. 2010;18:771–772.
Parvizi J, Ghanem E, Menashe S, Barrack RL, Bauer TW. Periprosthetic infection: what are the diagnostic challenges? J Bone Joint Surg Am. 2006;88(suppl 4):138–147.
Parvizi J, Jacovides C, Zmistowski B, Jung KA. Definition of periprosthetic joint infection: is there a consensus? Clin Orthop Relat Res. 2011;469:3022–3030.
Parvizi J, Suh DH, Jafari SM, Mullan A, Purtill JJ. Aseptic loosening of total hip arthroplasty: infection always should be ruled out. Clin Orthop Relat Res. 2011;469:1401–1405.
Parvizi J, Zmistowski B, Berbari EF, Bauer TW, Springer BD, Della Valle CJ, Garvin KL, Mont MA, Wongworawat MD, Zalavras CG. New definition for periprosthetic joint infection: from the Workgroup of the Musculoskeletal Infection Society. Clin Orthop Relat Res. 2011;469:2992–2994.
Perry JL, Ballou DR, Salyer JL. Inhibitory properties of a swab transport device. J Clin Microbiol. 1997;35:3367–3368.
Rasouli MR, Harandi AA, Adeli B, Purtill JJ, Parvizi J. Revision total knee arthroplasty: infection should be ruled out in all cases. J Arthroplasty. 2012;27:1239–1243.e1–2.
Schäfer P, Fink B, Sandow D, Margull A, Berger I, Frommelt L. Prolonged bacterial culture to identify late periprosthetic joint infection: a promising strategy. Clin Infect Dis. 2008;47:1403–1409.
Schinsky MF, Della Valle CJ, Sporer SM, Paprosky WG. Perioperative testing for joint infection in patients undergoing revision total hip arthroplasty. J Bone Joint Surg Am. 2008;90:1869–1875.
Spangehl MJ, Masri BA, O’Connell JX, Duncan CP. Prospective analysis of preoperative and intraoperative investigations for the diagnosis of infection at the sites of two hundred and two revision total hip arthroplasties. J Bone Joint Surg Am. 1999;81:672–683.
Stoodley P, Ehrlich GD, Sedghizadeh PP, Hall-Stoodley L, Baratz ME, Altman DT, Sotereanos NG, Costerton JW, Demeo P. Orthopaedic biofilm infections. Curr Orthop Pract. 2011;22:558–563.
Trampuz A, Piper KE, Jacobson MJ, Hanssen AD, Unni KK, Osmon DR, Mandrekar JN, Cockerill FR, Steckelberg JM, Greenleaf JF, Patel R. Sonication of removed hip and knee prostheses for diagnosis of infection. N Engl J Med. 2007;357:654–663.
Williams JL, Norman P, Stockley I. The value of hip aspiration versus tissue biopsy in diagnosing infection before exchange hip arthroplasty surgery. J Arthroplasty. 2004;19:582–586.
Wilson ML, Winn W. Laboratory diagnosis of bone, joint, soft-tissue, and skin infections. Clin Infect Dis. 2008;46:453–457.
Acknowledgments
The authors thank Donald Jungkind PhD and the Thomas Jefferson University Hospital surgical and microbiology laboratory staff for cooperation in undertaking and completing the protocol for this study. The authors also thank the Thomas Jefferson University Hospital nursing and surgical staff for cooperating and aiding in specimen collection for this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article
Cite this article
Aggarwal, V.K., Higuera, C., Deirmengian, G. et al. Swab Cultures Are Not As Effective As Tissue Cultures for Diagnosis of Periprosthetic Joint Infection. Clin Orthop Relat Res 471, 3196–3203 (2013). https://doi.org/10.1007/s11999-013-2974-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-013-2974-y