
Abstract
Background
Nonsurgical management of de Quervain’s tenosynovitis often includes corticosteroid injections. If the injection does not enter the compartment, or all subcompartments, response to the injection is variable. To ensure proper location of injections we evaluated the role of ultrasound.
Questions/Purposes
We determined (1) the incidence of two or more subcompartments, (2) the incidence of anatomic variations during surgical release after failed injections, and (3) the relief of pain after ultrasound-guided injections.
Patients and Methods
A prospective series of 40 consecutive patients (42 wrists) diagnosed with de Quervain’s tenosynovitis by clinical examination were referred to a radiologist for an ultrasound-guided injection. The radiologist injected the first dorsal compartment and noted any septations. Patients returned for followup where outcomes, DASH, and VAS scores were calculated. The treating surgeon was blinded to any anatomic variations. Followup was at 6 weeks and a minimum of 6 months (mean, 6 weeks, range, 3–17 months; mean, 11 months, range, 7–18 months). Four patients were lost to followup.
Results
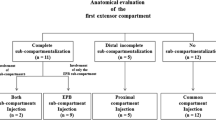
Multiple subcompartments were noted in 22 of 42 (52%) wrists. At the 6-week followup, 36 of the 37 wrists examined in 36 patients (97%) had at least partial resolution of symptoms. Multiple subcompartments were identified in 52% of cases. At last followup, the mean DASH and VAS scores were 18.4 and 2.2, respectively. However 14% of wrists had recurrence of symptoms, all of which had subcompartments on ultrasound. No adverse effects from the injections were noted.
Conclusion
We found ultrasound-guided injections to be useful for treatment of de Quervain’s tenosynovitis. Our success with ultrasound-guided injections was slightly better than that reported in the literature and without adverse reactions.
Level of Evidence
Level IV, therapeutic study. See the Guidelines for Authors for a complete description of levels of evidence.


Similar content being viewed by others

References
Alemohammad AM, Yazaki N, Morris RP, Buford WL, Viegas SF. Thumb interphalangeal joint extension by the extensor pollicis brevis: association with a subcompartment and de Quervain’s disease. J Hand Surg Am. 2009;34:719–723.
Anderson BC, Manthey R, Brouns MC. Treatment of de Quervain’s tenosynovitis with corticosteroids: a prospective study of the response to local injection. Arthritis Rheum. 1991;34:793–798.
Bahm J, Szabo Z, Foucher G. The anatomy of De Quervain’s disease: a study of operative findings. Int Orthop. 1995;19:209–211.
Chaffee A, Yakuboff M, Tanabe T. Responsiveness of the VAS and McGill pain questionnaire in measuring changes in musculoskeletal pain. J Sport Rehabil. 2011;20:250–255.
Quervain F. On a form of chronic tendovaginitis by Dr. Fritz de Quervain in la Chaux-de-Fonds. 1895. Am J Orthop Belle Mead NJ. 1997;26:641–644.
Finkelstein H. Stenosing tendovaginitis at the radial styloid process. J Bone Joint Surg Am. 1930;12:509–540.
Giles KW. Anatomical variations affecting the surgery of de Quervain’s disease. J Bone Joint Surg Br. 1960;42:352–355.
Gonzalez MH, Sohlberg R, Brown A, Weinzweig N. The first dorsal extensor compartment: an anatomic study. J Hand Surg Am. 1995;20:657–660.
Gousheh J, Yavari M, Arasteh E. Division of the first dorsal compartment of the hand into two separate canals: rule or exception? Arch Iran Med. 2009;12:52–54.
Harvey FJ, Harvey PM, Horsley MW. De Quervain’s disease: surgical or nonsurgical treatment. J Hand Surg Am. 1990;15:83–87.
Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med. 1996;29:602–608.
Ilyas AM, Ast M, Schaffer AA, Thoder J. De quervain tenosynovitis of the wrist. J Am Acad Orthop Surg. 2007;15:757–764.
Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM. Anatomical variations in the first extensor compartment of the wrist: a clinical and anatomical study. J Bone Joint Surg Am. 1986;68:923–926.
Jeyapalan K, Choudhary S. Ultrasound-guided injection of triamcinolone and bupivacaine in the management of De Quervain’s disease. Skeletal Radiol. 2009;38:1099–1103.
Jirarattanaphochai K, Saengnipanthkul S, Vipulakorn K, Jianmongkol S, Chatuparisute P, Jung S. Treatment of de Quervain disease with triamcinolone injection with or without nimesulide: a randomized, double-blind, placebo controlled trial. J Bone Joint Surg Am. 2004;86:2700–2706.
Keon-Cohen B. De Quervain’s disease. J Bone Joint Surg Br. 1951;33:96–99.
Kwon BC, Choi SJ, Koh SH, Shin DJ, Baek GH. Sonographic identification of the intracompartmental septum in de Quervain’s disease. Clin Orthop Relat Res. 2010;468:2129–2134.
Lane LB, Boretz RS, Stuchin SA. Treatment of de Quervain’s disease: role of conservative management. J Hand Surg Br. 2001;26:258–260.
Leao L. De Quervain’s disease: a clinical and anatomical study. J Bone Joint Surg Am. 1958,40:1063–1070.
Leslie BM, Ericson WB Jr, Morehead JR. Incidence of a septum within the first dorsal compartment of the wrist. J Hand Surg Am. 1990;15:88–91.
Loomis LK. Variations of stenosing tenosynovitis at the radial styloid process. J Bone Joint Surg Am. 1951;33:340–346.
Mahakkanukrauh P, Mahakkanukrauh C. Incidence of a septum in the first dorsal compartment and its effects on therapy of de Quervain’s disease. Clin Anat. 2000;13:195–198.
McKenzie JM. Conservative treatment of de Quervain’s disease. Br Med J. 1972;4:659–660.
Minamikawa Y, Peimer CA, Cox WL, Sherwin FS. De Quervain’s syndrome: surgical and anatomical studies of the fibroosseous canal. Orthopedics. 1991;14:545–549.
Mirzanli C, Ozturk K, Esenyel CZ, Ayanoglu S, Imren Y, Aliustaoglu S. Accuracy of intrasheath injection techniques for de Quervain’s disease: a cadaveric study. J Hand Surg Eur Vol. 2012;37:155–160.
Nagaoka M, Matsuzaki H, Suzuki T. Ultrasonographic examination of de Quervain’s disease. J Orthop Sci. 2000;5:96–99.
Nayak RS, Hussein M, Krishnamurthy A, Mansur DI, Prabhu LV, D’Souza P, Potu BK, Chettiar GK. Variation and clinical significance of extensor pollicis brevis: a study in South Indian cadavers. Chang Gung Med J. 2009;32:600–604.
Opreanu RC, Wechter J, Tabbaa H, Kepros JP, Baulch M, Xie Y, Lackey W, Katranji A. Anatomic variations of the first extensor compartment and abductor pollicis longus tendon in trapeziometacarpal arthritis. Hand (NY). 2010;5:184–189.
Peters-Veluthamaningal C, Winters JC, Groenier KH, Meyboom-DeJong B. Randomised controlled trial of local corticosteroid injections for de Quervain’s tenosynovitis in general practice. BMC Musculoskelet Disord. 2009;10:131.
Richie CA 3rd, Briner WW Jr. Corticosteroid injection for treatment of de Quervain’s tenosynovitis: a pooled quantitative literature evaluation. J Am Board Fam Pract. 2003;16:102–106.
Sawaizumi T, Nanno M, Ito H. De Quervain’s disease: efficacy of intra-sheath triamcinolone injection. Int Orthop. 2007;31:265–268.
Weiss AP, Akelman E, Tabatabai M. Treatment of de Quervain’s disease. J Hand Surg Am. 1994;19:595–598.
Witt J, Pess G, Gelberman RH. Treatment of de Quervain tenosynovitis: a prospective study of the results of injection of steroids and immobilization in a splint. J Bone Joint Surg Am. 1991;73:219–222.
Visuthikosol V, Chanyasawat S. Surgical treatment of de Quervain’s diseases: a clinical review of 42 cases. J Med Assoc Thai. 1988;71:637–639.
Volpe A, Pavoni M, Marchetta A, Caramaschi P, Biasi D, Zorzi C, Arcaro G, Grassi W. Ultrasound differentiation of two types of de Quervain’s disease: the role of retinaculum. Ann Rheum Dis. 2010;69:938–939.
Yuasa K, Kiyoshige Y. Limited surgical treatment of de Quervain’s disease: decompression of only the extensor pollicis brevis subcompartment. J Hand Surg Am. 1998;23:840–843.
Zingas C, Failla JM, Van Holsbeeck M. Injection accuracy and clinical relief of de Quervain’s tendinitis. J Hand Surg Am. 1998;23:89–96.
Author information
Authors and Affiliations
Corresponding author
Additional information
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that he, or a member of their immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
About this article
Cite this article
McDermott, J.D., Ilyas, A.M., Nazarian, L.N. et al. Ultrasound-guided Injections for de Quervain’s Tenosynovitis. Clin Orthop Relat Res 470, 1925–1931 (2012). https://doi.org/10.1007/s11999-012-2369-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2369-5