
Abstract
Background
Dislocation after revision THA is a common complication. Large heads have the potential to decrease dislocation rate, but it is unclear whether they do so in revision THA.
Questions/purposes
We therefore determined whether a large femoral head (36 and 40 mm) resulted in a decreased dislocation rate compared to a standard head (32 mm).
Methods
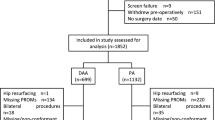
We randomized 184 patients undergoing revision THA to receive either a 32-mm head (92 patients) or 36- and 40-mm head (92 patients) and stratified patients by surgeon. The two groups had similar baseline demographics. The primary end point was dislocation. Quality-of-life (QOL) measures were WOMAC and SF-36. The mean followup for dislocation was 5 years (range, 2–7 years); the mean followup for QOL was 2.2 years (range, 1.6–4 years).
Results
In the 36- and 40-mm head group, the dislocation rate was 1.1% (one of 92) versus 8.7% (eight of 92) for the 32-mm head. There was no difference in QOL outcomes between the two groups.
Conclusions
Our observations confirm a large femoral head (36 or 40 mm) reduces dislocation rates in patients undergoing revision THA at short-term followup. We now routinely use large heads with a highly crosslinked polyethylene acetabular liner in all revision THAs.
Level of Evidence
Level I, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


References
Alberton GM, High WA, Morrey BF. Dislocation after revision total hip arthroplasty: an analysis of risk factors and treatment options. J Bone Joint Surg Am. 2002;84:1788–1792.
American Academy of Orthopaedic Surgeons. The burden of musculoskeletal diseases in the United States. Rosemont, IL. 2008. Available at: http://boneandjointburden.org/pdfs/BMUS_chpt4_arthritis.pdf. Accessed November 2, 2010.
Amlie E, Høvik Ø, Reikerås O. Dislocation after total hip arthroplasty with 28 and 32-mm femoral head. J Orthop Traumatol. 2010;11:111–115.
Bartz RL, Nobel PC, Kadakia NR, Tullos HS. The effect of femoral component head size on posterior dislocation of the artificial hip joint. J Bone Joint Surg Am. 2000;82:1300–1307.
Bellamy N, Buchanan W, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or the knee. J Rheumatol. 1988;15:1833–1840.
Bellamy N, Kirwan J, Boers M, Brooks P, Strand V, Tugwell P, Altman R, Brandt K, Dougados M, Lequesne M. Recommendations for a core set of outcome measures for future Phase III clinical trials in knee, hip, and hand osteoarthritis: consensus development at OMERACT III. J Rheumatol. 1997;24:799–802.
Berry DJ, von Knoch M, Schleck CD, Harmsen WS. Effect of femoral head diameter and operative approach on risk of dislocation after primary total hip arthroplasty. J Bone Joint Surg Am. 2005;87:2456–2463.
Burroughs BR, Hallstrom B, Golladay GJ, Hoeffel D, Harris WH. Range of motion and stability in total hip arthroplasty with 28-, 32-, 38-, and 44-mm femoral head sizes. J Arthroplasty. 2005;20:11–19.
Burroughs BR, Rubash HE, Harris WH. Femoral head sizes larger than 32 mm against highly cross-linked polyethylene. Clin Orthop Relat Res. 2002;405:150–157.
Conroy JL, Whitehouse SL, Graves SE, Pratt NL, Ryan P, Crawford RW. Risk factors for revision for early dislocation in total hip arthroplasty. J Arthroplasty. 2008;23:867–872.
Crowninshield RD, Maloney WJ, Wentz DH, Humphrey SM, Blanchard CR. Biomechanics of large femoral heads: what they do and don’t do. Clin Orthop Relat Res. 2004;429:102–107.
Dudda M, Gueleryuez A, Gautier E, Busato A, Roeder C. Risk factors for early dislocation after total hip arthroplasty: a matched case-control study. J Orthop Surg (Hong Kong). 2010;18:179–183.
Geller JA, Malchau H, Bragdon C, Greene M, Harris WH, Freiberg AA. Large diameter femoral heads on highly cross-linked polyethylene: minimum 3-year results. Clin Orthop Relat Res. 2006;447:53–59.
Jameson SS, Lees D, James P, Serrano-Pedraza I, Partington PF, Muller SD, Meek RM, Reed MR. Lower rates of dislocation with increased femoral head size after primary total hip replacement: a five-year analysis of NHS patients in England. J Bone Joint Surg Br. 2011;93:876–880.
Jenkinson C, Wright L, Coulter A. Criterion validity and reliability of the SF-36 in a population sample. Qual Life Res. 1994;3:7–12.
Kelley SS, Lachiewicz PF, Hickman JM, Paterno SM. Relationship of femoral head and acetabular size to the prevalence of dislocation. Clin Orthop Relat Res. 1998;355:163–170.
Kiguchi K, Horie T, Yamashita A, Ueno M, Kobayashi T, Mawatari M, Hotokebuchi T. A study of the effect of the femoral head diameter on prosthetic hip joint dislocation using a hip-joint motion simulator. Conf Proc IEEE Eng Med Biol Soc. 2009;2009:6058–6061.
Kung PL, Ries MD. Effect of femoral head size and abductors on dislocation after revision THA. Clin Orthop Relat Res. 2007;465:170–174.
Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780–785.
Lachiewicz PF, Soileau ES. Dislocation of primary total hip arthroplasty with 36 and 40-mm femoral heads. Clin Orthop Relat Res. 2006;453:153–155.
Morrey BF. Instability after total hip arthroplasty. Orthop Clin North Am. 1992;23:237–248.
Scifert CF, Brown TD, Pedersen DR, Callaghan JJ. A finite element analysis of factors influencing total hip dislocation. Clin Orthop Relat Res. 1998;355:152–162.
Skeels MD, Berend KR, Lombardi AV Jr. The dislocator, early and late: the role of large heads. Orthopedics. 2009;32:667. pii: orthosupersite.com/view.asp?rID = 42837. doi:10.3928/01477447-20090728-14.
Springer BD, Fehring TK, Griffin WL, Odum SM, Masonis JL. Why revision total hip arthroplasty fails. Clin Orthop Relat Res. 2009;467:166–173.
Yuan L, Shih C. Dislocation after total hip arthroplasty. Arch Orthop Trauma Surg. 1999;119:263–266.
Acknowledgments
The authors thank the following for recruiting patients: Dr. David Backstein, MD, MED, FRCSC, at Mount Sinai Hospital in Toronto, Canada; Dr. Colin Burnell, MD, FRCSC, Dr. David Hedden MD, FRCSC, and Dr. Thomas Turgeon, MD, MPH, FRCSC, at the University of Manitoba in Winnipeg, Canada; Dr. Scott Sporer, MD, at Rush University Medical Center in Chicago, IL, USA; Dr. Steven H. Weeden, MD, at the Texas Hip & Knee Center in Fort Worth, TX, USA; Dr. Paul Kim, MD, FRCSC, at the University of Ottawa, Canada; and Dr. Michael J. Dunbar, MD, PhD, FRCPC, at Dalhousie University in Halifax, Canada. The authors also thank Lorna McLean, Daphné Savoy, Matthew MacDonald, Sarah Tran, Emily Dittle, Carly Valdez, Heather Belanger, and Sue Moore for patient recruitment and study coordination and Eric Sayre, PhD, for his help with the statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author (DSG, BAM, CPD, AEG) certifies that he or she has or may receive payments or benefits (e.g, serve as a consultant) from a commercial entity (Zimmer, Inc, Warsaw, IN, USA) related to this work. Each author (NVG, ERB, MJP, CDV) certifies that he or she has no commercial associations (e.g, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. The institution of the authors (DSG, BAM, CPD, NVG, CDV) has received funding from Zimmer, Inc.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA approval status, of any drug or device before clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
This work was performed at the University of British Columbia; the University of Manitoba; Rush University Medical Center; and Mount Sinai Hospital.
About this article
Cite this article
Garbuz, D.S., Masri, B.A., Duncan, C.P. et al. The Frank Stinchfield Award: Dislocation in Revision THA: Do Large Heads (36 and 40 mm) Result in Reduced Dislocation Rates in a Randomized Clinical Trial?. Clin Orthop Relat Res 470, 351–356 (2012). https://doi.org/10.1007/s11999-011-2146-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-011-2146-x