
Opinion statement
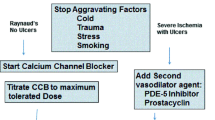
Raynaud’s phenomenon is characterized by intense vasospasm of digital arteries on cold exposure or with emotional stress, leading to well-defined color changes of digital skin. It may be primary (Raynaud’s disease) or secondary to an underlying condition, including autoimmune rheumatic diseases. Although Raynaud’s disease is predominantly a vasospastic condition, Raynaud’s phenomenon in connective tissue diseases often is a result of an underlying vaso-occlusive process. As a result, the manifestations are more severe and persistent and often warrant pharmacologic therapy. Dihydropyridine calcium channel blockers are by far the most commonly studied and prescribed class of agents for the treatment of Raynaud’s phenomenon. There is some evidence for the efficacy of other classes of drugs, such as topical nitrates, α-antagonists, angiotensin receptor blockers, selective serotonin reuptake inhibitors, and pentoxifylline. However, the data on the efficacy of these agents are not as convincing, and they are not proven to be more effective than calcium channel blockers. Hence, their place in the therapy of Raynaud’s phenomenon is limited to patients who fail to respond adequately to or are unable to tolerate calcium channel blockers. More expensive second-line agents, such as phosphodiesterase-5 inhibitors, endothelin receptor antagonists, and intravenous prostanoids, are reserved for refractory cases of secondary Raynaud’s phenomenon with severe digital ischemia leading to ulceration or gangrene. These drugs may be used in isolation or as adjunct therapy to the first-line agents. Chemical and/or surgical sympathectomy may be considered if sympathetically driven digital ischemia is severe and resistant to pharmacologic intervention. These procedures may temporarily reverse the digital ischemia and help tide over the crisis, whereas the improvement thus achieved can be maintained by continuing medical therapy. In cases of ischemic digital ulceration, it is important to achieve adequate analgesia and to identify and treat superadded infection.


Similar content being viewed by others


References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Raynaud M: Local Asphyxia and Symmetrical Gangrene of the Extremities. Paris: L. Leclerc; 1862.
Boin F, Wigley FM: Understanding, assessing and treating Raynaud’s phenomenon. Curr Opin Rheumatol 2005, 17(6):752–760.
Herrick AL: Pathogenesis of Raynaud’s phenomenon. Rheumatology (Oxford) 2005, 44(5):587–596.
Sunderkotter C, Riemekasten G: Pathophysiology and clinical consequences of Raynaud’s phenomenon related to systemic sclerosis. Rheumatology (Oxford) 2006, 45(Suppl 3):iii33–iii35.
Kuwana M, Okazaki Y, Yasuoka H, et al.: Defective vasculogenesis in systemic sclerosis. Lancet 2004, 364(9434):603–610.
Harrison BJ, Silman AJ, Hider SL, Herrick AL: Cigarette smoking as a significant risk factor for digital vascular disease in patients with systemic sclerosis. Arthritis Rheum 2002, 46(12):3312–3316.
Thompson AE, Shea B, Welch V, et al.: Calcium-channel blockers for Raynaud’s phenomenon in systemic sclerosis. Arthritis Rheum 2001, 44(8):1841–1847.
Rodeheffer RJ, Rommer JA, Wigley F, Smith CR: Controlled double-blind trial of nifedipine in the treatment of Raynaud’s phenomenon. N Engl J Med 1983, 308(15):880–883.
Kallenberg CG, Wouda AA, Kuitert JJ, et al.: Nifedipine in Raynaud’s phenomenon: relationship between immediate, short term and longterm effects. J Rheumatol 1987, 14(2):284–290.
La Civita L, Pitaro N, Rossi M, et al.: Amlodipine in the treatment of Raynaud’s phenomenon. Br J Rheumatol 1993, 32(6):524–525.
Kahan A, Amor B, Menkes CJ: A randomised double-blind trial of diltiazem in the treatment of Raynaud’s phenomenon. Ann Rheum Dis 1985, 44(1):30–33.
White CJ, Phillips WA, Abrahams LA, et al.: Objective benefit of nifedipine in the treatment of Raynaud’s phenomenon. Double-blind controlled study. Am J Med 1986, 80(4):623–625.
Takahara K, Kuroiwa A, Matsushima T, et al.: Effects of nifedipine on platelet function. Am Heart J 1985, 109(1):4–8.
Wise RA, Malamet R, Wigley FM: Acute effects of nifedipine on digital blood flow in human subjects with Raynaud’s phenomenon: a double blind placebo controlled trial. J Rheumatol 1987, 14(2):278–283.
Messerli FH, Grossman E: The calcium antagonist controversy: a posthumous commentary. Am J Cardiol 1998, 82(9B):35R–39R.
Comparison of sustained-release nifedipine and temperature biofeedback for treatment of primary Raynaud phenomenon. Results from a randomized clinical trial with 1-year follow-up. Arch Intern Med 2000, 160(8):1101–1108.
Ettinger WH, Wise RA, Schaffhauser D, Wigley FM: Controlled double-blind trial of dazoxiben and nifedipine in the treatment of Raynaud’s phenomenon. Am J Med 1984, 77(3):451–456.
Vinjar B, Stewart M: Oral vasodilators for primary Raynaud’s phenomenon. Cochrane Database Syst Rev 2008, CD006687. This comprehensive systematic review by the Cochrane Peripheral Vascular Diseases Group of randomized controlled trials evaluates the effects of various oral vasodilator agents on subjective symptoms in primary Raynaud’s phenomenon.
Henness S, Wigley FM: Current drug therapy for scleroderma and secondary Raynaud’s phenomenon: evidence-based review. Curr Opin Rheumatol 2007, 19(6):611-618. This is a nice review examining the efficacy of various pharmacologic therapies in treating scleroderma and Raynaud’s phenomenon secondary to scleroderma or other connective tissue diseases. Only fully published, randomized, controlled trials that had a duration of at least 1 month were included.
Anderson ME, Moore TL, Hollis S, et al.: Digital vascular response to topical glyceryl trinitrate, as measured by laser Doppler imaging, in primary Raynaud’s phenomenon and systemic sclerosis. Rheumatology (Oxford) 2002, 41(3):324–328.
Peterson LL, Vorhies C: Raynaud’s syndrome. Treatment with sublingual administration of nitroglycerin, swinging arm maneuver, and biofeedback training. Arch Dermatol 1983, 119(5):396–399.
Kan C, Akimoto S, Abe M, et al.: Preliminary thermographic evaluation of new nitroglycerine tape on the peripheral circulatory disturbance in systemic sclerosis. Ann Rheum Dis 2002, 61(2):177–179.
Teh LS, Manning J, Moore T, et al.: Sustained-release transdermal glyceryl trinitrate patches as a treatment for primary and secondary Raynaud’s phenomenon. Br J Rheumatol 1995, 34(7):636–641.
Chung L, Shapiro L, Fiorentino D, et al.: MQX-503, a novel formulation of nitroglycerin, improves the severity of Raynaud’s phenomenon: a randomized, controlled trial. Arthritis Rheum 2009, 60(3):870–877. This randomized placebo-controlled study demonstrated that this novel formulation of topical nitroglycerin is well tolerated and more effective than placebo for treating primary or secondary Raynaud’s phenomenon.
Jaffe IA: Serotonin reuptake inhibitors in Raynaud’s phenomenon. Lancet 1995, 345(8961):1378.
Coleiro B, Marshall SE, Denton CP, et al.: Treatment of Raynaud’s phenomenon with the selective serotonin reuptake inhibitor fluoxetine. Rheumatology (Oxford) 2001, 40(9):1038–1043.
Warren JB, Loi RK: Captopril increases skin microvascular blood flow secondary to bradykinin, nitric oxide, and prostaglandins. FASEB J 1995, 9(5):411–418.
Tosi S, Marchesoni A, Messina K, et al.: Treatment of Raynaud’s phenomenon with captopril. Drugs Exp Clin Res 1987, 13(1):37–42.
Gliddon AE, Dore CJ, Black CM, et al.: Prevention of vascular damage in scleroderma and autoimmune Raynaud’s phenomenon: a multicenter, randomized, double-blind, placebo-controlled trial of the angiotensin-converting enzyme inhibitor quinapril. Arthritis Rheum 2007, 56(11):3837–3846.
Dziadzio M, Denton CP, Smith R, et al.: Losartan therapy for Raynaud’s phenomenon and scleroderma: clinical and biochemical findings in a fifteen-week, randomized, parallel-group, controlled trial. Arthritis Rheum 1999, 42(12):2646–2655.
Gore J, Silver R: Oral sildenafil for the treatment of Raynaud’s phenomenon and digital ulcers secondary to systemic sclerosis. Ann Rheum Dis 2005, 64(9):1387.
Fries R, Shariat K, von Wilmowsky H, Bohm M: Sildenafil in the treatment of Raynaud’s phenomenon resistant to vasodilatory therapy. Circulation 2005, 112(19):2980–2985.
Friedman EA, Harris PA, Wood AJ, et al.: The effects of tadalafil on cold-induced vasoconstriction in patients with Raynaud’s phenomenon. Clin Pharmacol Ther 2007, 81(4):503–509. This well-done mechanistic study in subjects with Raynaud’s phenomenon proved that clinical benefit with PDE5 inhibitors, if any, probably involves mechanisms other than acute inhibition of cold-induced vasoconstriction.
Caglayan E, Huntgeburth M, Karasch T, et al.: Phosphodiesterase type 5 inhibition is a novel therapeutic option in Raynaud disease. Arch Intern Med 2006, 166(2):231–233.
Schiopu E, Hsu VM, Impens AJ, et al.: Randomized placebo-controlled crossover trial of tadalafil in Raynaud’s phenomenon secondary to systemic sclerosis. J Rheumatol 2009, 36(10):2264–2268. This recently published, well-designed, double-blind study demonstrated the lack of efficacy of oral tadalafil in improving subjective measures of Raynaud’s phenomenon in women with systemic sclerosis.
Muller R: Pentoxifylline—a biomedical profile. J Med 1979, 10(5):307–329.
Nenci GG, Gresele P, Agnelli G, Ballatori E: Effect of pentoxifylline on platelet aggregation. Pharmatherapeutica 1981, 2(8):532–538.
Neirotti M, Longo F, Molaschi M, et al.: Functional vascular disorders: treatment with pentoxifylline. Angiology 1987, 38(8):575–580.
Goodfield MJ, Rowell NR: Treatment of peripheral gangrene due to systemic sclerosis with intravenous pentoxifylline. Clin Exp Dermatol 1989, 14(2):161–162.
Korn JH, Mayes M, Matucci CM, et al.: Digital ulcers in systemic sclerosis: prevention by treatment with bosentan, an oral endothelin receptor antagonist. Arthritis Rheum 2004, 50(12):3985–3993.
Garcia de la Pena-Lefebvre P, Rodriguez RS, Valero EM, et al.: Long-term experience of bosentan for treating ulcers and healed ulcers in systemic sclerosis patients. Rheumatology (Oxford) 2008, 47(4):464–466. This recently published prospective, observational, noncontrolled study reinforced the findings of RAPIDS 1 [40] that bosentan is a safe and effective agent for long-term use in preventing ischemic digital ulcers in scleroderma.
Selenko-Gebauer N, Duschek N, Minimair G, et al.: Successful treatment of patients with severe secondary Raynaud’s phenomenon with the endothelin receptor antagonist bosentan. Rheumatology (Oxford) 2006, 45(Suppl 3):iii45–iii48.
Sfikakis PP, Papamichael C, Stamatelopoulos KS, et al.: Improvement of vascular endothelial function using the oral endothelin receptor antagonist bosentan in patients with systemic sclerosis. Arthritis Rheum 2007, 56(6):1985–1993. This recently published prospective study demonstrated that bosentan improves endothelial function, indicating a direct, reversible effect of endothelin in scleroderma vasculopathy.
Hettema ME, Zhang D, Stienstra Y, et al.: No effects of bosentan on microvasculature in patients with limited cutaneous systemic sclerosis. Clin Rheumatol 2009, 28(7):825–833. This interesting short-term mechanistic pilot study demonstrated no significant changes in vasodilator responses, capillary permeability, or capillary density following bosentan treatment, suggesting that bosentan is ineffective in improving microvascular structure and function in limited scleroderma.
Russell IJ, Lessard JA: Prazosin treatment of Raynaud’s phenomenon: a double blind single crossover study. J Rheumatol 1985, 12(1):94–98.
Wollersheim H, Thien T, Fennis J, et al.: Double-blind, placebo-controlled study of prazosin in Raynaud’s phenomenon. Clin Pharmacol Ther 1986, 40(2):219–225.
Wise RA, Wigley FM, White B, et al.: Efficacy and tolerability of a selective alpha(2C)-adrenergic receptor blocker in recovery from cold-induced vasospasm in scleroderma patients: a single-center, double-blind, placebo-controlled, randomized crossover study. Arthritis Rheum 2004, 50(12):3994–4001.
Clifford PC, Martin MF, Sheddon EJ, et al.: Treatment of vasospastic disease with prostaglandin E1. Br Med J 1980, 281(6247):1031–1034.
Mohrland JS, Porter JM, Smith EA, et al.: A multiclinic, placebo-controlled, double-blind study of prostaglandin E1 in Raynaud’s syndrome. Ann Rheum Dis 1985, 44(11):754–760.
Dowd PM, Martin MF, Cooke ED, et al.: Treatment of Raynaud’s phenomenon by intravenous infusion of prostacyclin (PGI2). Br J Dermatol 1982, 106(1):81–89.
Belch JJ, Newman P, Drury JK, et al.: Intermittent epoprostenol (prostacyclin) infusion in patients with Raynaud’s syndrome. A double-blind controlled trial. Lancet 1983, 1(8320):313–315.
Wigley FM, Wise RA, Seibold JR, et al.: Intravenous iloprost infusion in patients with Raynaud phenomenon secondary to systemic sclerosis. A multicenter, placebo-controlled, double-blind study. Ann Intern Med 1994, 120(3):199–206.
Gardinali M, Pozzi MR, Bernareggi M, et al.: Treatment of Raynaud’s phenomenon with intravenous prostaglandin E1alpha-cyclodextrin improves endothelial cell injury in systemic sclerosis. J Rheumatol 2001, 28(4):786–794.
Chung L, Fiorentino D: A pilot trial of treprostinil for the treatment and prevention of digital ulcers in patients with systemic sclerosis. J Am Acad Dermatol 2006, 54(5):880–882.
Tsukamoto H, Nagasawa K: Successful treatment of Raynaud’s phenomenon with limaprost, an oral prostaglandin E1 analogue. Br J Rheumatol 1991, 30(4):317.
Lau CS, Belch JJ, Madhok R, et al.: A randomised, double-blind study of cicaprost, an oral prostacyclin analogue, in the treatment of Raynaud’s phenomenon secondary to systemic sclerosis. Clin Exp Rheumatol 1993, 11(1):35–40.
Clagett GP, Sobel M, Jackson MR, et al.: Antithrombotic therapy in peripheral arterial occlusive disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004, 126(3 Suppl):609S–626S.
Denton CP, Howell K, Stratton RJ, Black CM: Long-term low molecular weight heparin therapy for severe Raynaud’s phenomenon: a pilot study. Clin Exp Rheumatol 2000, 18(4):499–502.
Hart DA, Fritzler MJ: Regulation of plasminogen activators and their inhibitors in rheumatic diseases: new understanding and the potential for new directions. J Rheumatol 1989, 16(9):1184–1191.
Van Beek AL, Lim PK, Gear AJ, Pritzker MR: Management of vasospastic disorders with botulinum toxin A. Plast Reconstr Surg 2007, 119(1):217–226. This is a very well-written, recently published case series of patients with critical digital ischemia, all of whom failed aggressive medical therapy. Most of the patients had scleroderma or mixed connective tissue disease. Treatment with perivascular injections of botulinum toxin A led to significant and persistent pain reduction, spontaneous ulcer healing, and a decrease in severity and frequency of Raynaud’s episodes.
Montorsi W, Ghiringhelli C, Annoni F: Indications and results of the surgical treatment in Raynaud’s phenomenon. J Cardiovasc Surg (Torino) 1980, 21(2):203–210.
de Trafford JC, Lafferty K, Potter CE, et al.: An epidemiological survey of Raynaud’s phenomenon. Eur J Vasc Surg 1988, 2(3):167–170.
Matsumoto Y, Ueyama T, Endo M, et al.: Endoscopic thoracic sympathicotomy for Raynaud’s phenomenon. J Vasc Surg 2002, 36(1):57–61.
Yee AM, Hotchkiss RN, Paget SA: Adventitial stripping: a digit saving procedure in refractory Raynaud’s phenomenon. J Rheumatol 1998, 25(2):269–276.
Tomaino MM, Goitz RJ, Medsger TA: Surgery for ischemic pain and Raynaud’s phenomenon in scleroderma: a description of treatment protocol and evaluation of results. Microsurgery 2001, 21(3):75–79.
Kotsis SV, Chung KC: A systematic review of the outcomes of digital sympathectomy for treatment of chronic digital ischemia. J Rheumatol 2003, 30(8):1788–1792.
Taylor MH, McFadden JA, Bolster MB, Silver RM: Ulnar artery involvement in systemic sclerosis (scleroderma). J Rheumatol 2002, 29(1):102–106.
Bunker CB, Reavley C, O’Shaughnessy DJ, Dowd PM: Calcitonin gene-related peptide in treatment of severe peripheral vascular insufficiency in Raynaud’s phenomenon. Lancet 1993, 342(8863):80–83.
Sambo P, Amico D, Giacomelli R, et al.: Intravenous N-acetylcysteine for treatment of Raynaud’s phenomenon secondary to systemic sclerosis: a pilot study. J Rheumatol 2001, 28(10):2257–2262.
Kuwana M, Kaburaki J, Okazaki Y, et al.: Increase in circulating endothelial precursors by atorvastatin in patients with systemic sclerosis. Arthritis Rheum 2006, 54(6):1946–1951.
Acknowledgment
The author is grateful to Ms. Marcia Wyman, PharmD, drug information pharmacist at the Cleveland Clinic, for providing the prices of the individual drugs.
Disclosure
Dr. Chatterjee is a member of the Scientific Advisory Board for and has also received grant support from Gilead Sciences, Inc. He is an investigator for clinical trials run by United Therapeutics Corporation, MedImmune, and MediQuest Therapeutics.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chatterjee, S. Management of Raynaud’s Phenomenon in the Patient with Connective Tissue Disease. Curr Treat Options Cardio Med 12, 185–204 (2010). https://doi.org/10.1007/s11936-010-0065-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11936-010-0065-x