
Abstract
Fungal rhinosinusitis presents in five clinicopathologic forms, each with distinct diagnostic criteria, treatment, and prognosis. The invasive forms are acute fulminant, chronic, and granulomatous ("indolent") invasive fungal sinusitis. The noninvasive forms are fungal ball ("sinus mycetoma") and allergic fungal sinusitis (AFS). AFS is the most common form of fungal rhinosinusitis. Patients with AFS are atopic to aeroallergens including the involved fungal organism, immunocompetent, have nasal polyps and chronic allergic rhinosinusitis, often produce nasal casts, and may occasionally present with proptosis from orbital extension of disease. Sinus CT shows sinus mucosal hypertrophy and often hyperattenuation of sinus contents. Diagnosis is made from surgical histopathology with or without an associated positive surgical sinus fungal culture. The histopathology shows extramucosal allergic mucin that stains positive for scattered fungal hyphae and eosinophilic-lymphocytic sinus mucosal inflammation. Bipolaris spicifera is the most common fungus cultured. The immunopathology of AFS has been shown to be analogous to allergic bronchopulmonary aspergillosis. Treatment requires surgery and aggressive postoperative medical management with close follow-up. Medical treatment includes allergy medications, allergen immunotherapy, and in many cases the addition of oral corticosteroids. Although medical management clearly improves patient outcomes, more studies are needed because AFS recurrence rates remain high.
Similar content being viewed by others


References and Recommended Reading
deShazo RD, Chapin K, Swain RE: Fungal sinusitis. N Engl J Med 1997, 337:254–259.
Mitchell TG: Overview of basic medical mycology. Otolaryngol Clin North Am 2000, 33:237–249.
Ferguson BJ: Mucormycosis of the nose and paranasal sinuses. Otolaryngol Clin North Am 2000, 33:349–365.
Schubert MS, Goetz DW: Evaluation and treatment of allergic fungal sinusitis: I: demographics and diagnosis. J Allergy Clin Immunol 1998, 102:387–394. With another article by Schubert and Goetz [8], this is the largest published case series (67 patients over 8 years) of diagnosis and treatment of AFS. It shows the southwestern United States to be a "hot spot" for the disease. It simplifies the working diagnostic criteria, expands the clinical and immunoserologic findings, analyzes and compares treatment outcomes between patients treated with and without a consistent postoperative protocol of OCS, and analyzes the clinical utility of following the total serum IgE postoperatively.
Millar JW, Johnston A, Lamb D: Allergic aspergillosis of the paranasal sinuses [Abstract]. Thorax 1981, 36:710.
Katzenstein AA, Sale SR, Greenberger PA: Allergic aspergillus sinusitis: a newly recognized form of sinusitis. J Allergy Clin Immunol 1983, 72:89–93.
deJuan E, Green WR, Iliff NT: Allergic periorbital mucopyocele in children. Am J Ophthalmol 1983, 96:299–303.
Schubert MS, Goetz DW: Evaluation and treatment of allergic fungal sinusitis: II: treatment and follow-up. J Allergy Clin Immunol 1998, 102:395–402. With another article by Schubert and Goetz [4], this is the largest published case series (67 patients over 8 years) of diagnosis and treatment of AFS.
Ence BK, Gourley DS, Jorgensen NL, et al.: Allergic fungal sinusitis. Am J Rhinol 1990, 4:169–178.
Schweitz LA, Gourley DS: Allergic fungal sinusitis. Allergy Proc 1992, 13:3–6.
Kaliner MA, Osguthorpe DJ, Fireman P, et al.: Sinusitis: bench to bedside. J Allergy Clin Immunol 1997, 99:S829-S848.
Shah A, Khan ZU, Chaturvedi S, et al.: Concomitant allergic aspergillus sinusitis and allergic bronchopulmonary aspergillosis associated with familial occurrence of allergic bronchopulmonary aspergillosis. Ann Allergy 1990, 64:507–512.
Sher TH, Schwartz HJ: Allergic aspergillus sinusitis with concurrent allergic bronchopulmonary aspergillosis: report of a case. J Allergy Clin Immunol 1988, 81:844–846.
Travis WD, Kwon-Chung KJ, Kleiner DE, et al.: Unusual aspects of allergic bronchopulmonary fungal disease: report of two cases due to Curvularia organisms associated with allergic fungal sinusitis. Hum Pathol 1991, 22:1240–1248.
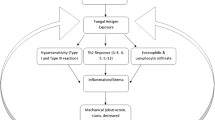
Schubert MS: Medical treatment of allergic fungal sinusitis. Ann Allergy Asthma Immunol 2000, 85:90–101. This recent review article includes a model for the "AFS rhinosinusitis Cycle" as integrated into the "allergic hypertrophic rhinosinusitis cycle" and a stepwise approach to diagnosis, treatment, and follow-up of AFS.
Gourley DS, Whisman BA, Jorgensen NL, et al.: Allergic Bipolaris sinusitis: clinical and immunopathologic characteristics. J Allergy Clin Immunol 1990, 85:583–591.
Bent JP, Kuhn FA: Diagnosis of allergic fungal sinusitis. Otolaryngol Head Neck Surg 1994, 111:580–588.
deShazo RD, Swain RE: Diagnostic criteria for allergic fungal sinusitis. J Allergy Clin Immunol 1995, 96:24–35.
Ponikau JU, Sherris DA, Kern EB, et al.: The diagnosis and incidence of allergic fungal sinusitis. Mayo Clin Proc 1999, 74:877–884.
Kuhn FA, Javer AR: Allergic fungal sinusitis: a four year follow-up. Am J Rhinol 2000, 14:149–156. One of the most experienced surgeons to diagnose and treat AFS in the southern United States provides an update on the postsurgical monitoring and follow-up of 11 patients with AFS. The authors discuss the utility of their endoscopic mucosal staging system for AFS.
Dibbern DA, Dreskin SC: Allergic fungal sinusitis [Letter]. Mayo Clin Proc 2000, 75:122.
Page EH: Allergic fungal sinusitis [Letter]. Mayo Clin Proc 2000, 75:122.
Mukherji SK, Figueroa RE, Ginsberg LE, et al.: Allergic fungal sinusitis: CT findings. Radiology 1998, 207:417–422. This is an excellent review of the CT findings for AFS. This is important because CT is the radiographic technique of choice for patients with virtually all forms of chronic sinusitis.
Greenberger PA, Patterson R: Diagnosis and management of allergic bronchopulmonary aspergillosis. Ann Allergy 1986, 56:444–452.
Greenberger PA: Allergic bronchopulmonary aspergillosis. In Allergy: Principles and Practice. Edited by Middleton E jr, Reed CE, Ellis EF, et al. St. Louis: Mosby; 1998:981–993.
Safirstein B: Allergic bronchopulmonary aspergillosis with obstruction of the upper respiratory tract. Chest 1976, 70:788–790.
Goldstein MF, Atkins PC, Cogen FC, et al.: Allergic aspergillus sinusitis. J Allergy Clin Immunol 1985, 76:515–524.
Waxman JE, Spector JG, Sale SR, Katzenstein AA: Allergic aspergillus sinusitis: concepts in diagnosis and treatment of a new clinical entity. Laryngoscope 1987, 97:261–266.
Sher TH, Schwartz HJ: Allergic aspergillus sinusitis with concurrent allergic bronchopulmonary aspergillosis: report of a case. J Allergy Clin Immunol 1988, 81:844–846.
Goldstein MF, Dvorin DJ, Dunsky EH, et al.: Allergic rhizomucor sinusitis. J Allergy Clin Immunol 1992, 90:394–403.
Roth M: Should oral steroids be the primary treatment for allergic fungal sinusitis? Ear Nose Throat J 1994, 73:928–930.
Kinsella JB, Bradfield JJ, Gourley WK, et al.: Allergic fungal sinusitis. Clin Otolaryngol 1996, 21:389–392.
Kupferberg SB, Bent JP: Allergic fungal sinusitis in the pediatric population. Arch Otolaryngol Head Neck Surg 1996, 122:1381–1384.
Frenkel L, Kuhls TL, Nitta K, et al.: Recurrent Bipolaris sinusitis following surgical and antifungal therapy. Pediatr Infect Dis J 1987, 6:1130–1132.
Bent JP, Kuhn FA: Antifungal activity against allergic fungal sinusitis organisms. Laryngoscope 1996, 106:1331–1334.
Andes D, Proctor R, Bush RK, Pasic TR: Report of successful prolonged antifungal therapy for refractory allergic fungal sinusitis. Clin Infect Dis 2000, 31:202–204.
Stevens DA, Schwartz HJ, Lee JY, et al.: A randomized trial of itraconazole in allergic bronchopulmonary aspergillosis. N Engl J Med 2000, 342:756–762.
Manning SC, Vuitch F, Weinberg AG, Brown OE: Allergic aspergillosis: a newly recognized form of sinusitis in the pediatric population. Laryngoscope 1989, 99:681–685.
Mabry RL, Marple BF, Folker RJ, Mabry CS: Immunotherapy in the treatment of allergic fungal sinusitis: three years’ experience. Otolaryngol Head Neck Surg 1998, 119:648–651.
Ramadan HH, Quraishi HA: Allergic mucin sinusitis without fungus. Am J Rhinol 1997, 11:145–147.
Ferguson BJ: Eosinophilic mucin rhinosinusitis: a distinct clinicopathological entity. Laryngoscope 2000, 110:799–813. This is a comprehensive review of chronic sinusitis that further substantiates the presence of allergic mucin but without fungal involvement in other forms of chronic sinusitis, proposing the term "eosinophilic mucin rhinosinusitis (EMRS)." The article discusses the possible clinical and immunologic differences between EMRS and AFS and serves as a caution in adhering to strict diagnostic criteria for AFS.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Schubert, M.S. Fungal rhinosinusitis: Diagnosis and therapy. Curr Allergy Asthma Rep 1, 268–276 (2001). https://doi.org/10.1007/s11882-001-0018-2
Issue Date:
DOI: https://doi.org/10.1007/s11882-001-0018-2