
Abstract
Carbon dioxide emissions (CO2e) which is caused by energy use contributes to the global average surface temperature increase by 1.5 °C as compared to the mid-1800s which is causing a certain change in the climate and becoming an adverse effect on health and economy. The relationship between health status, CO2e, and energy use has yet to be thoroughly investigated in the top 20 highest emitting economies. The data from 2000 to 2019 is analyzed by using advanced techniques of cross-sectional augmented distributed lag (CS-DL) and cross-sectional augmented autoregressive distributed lag (CS-ARDL) which take into consideration crucial elements of panel data, namely dynamics, heterogeneity, and cross-sectional dependence. Moreover, cross-sectional augmented error correction method (CS-ECM) and the common dynamic process of the augmented mean group (AMG) are applied for robustness checks. The empirical findings revealed that (i) CO2e weakens the health status only in the short-run, whereas health expenditure improves the health status in the both short- and long-runs, while economic growth is not contributing to the health status in the both short- and long-runs; (ii) health expenditure and economic growth only help to mitigate CO2e in the long-run, whereas energy use causes CO2e in the both short- and long-runs; (iii) energy use causes high economic growth in the both short- and long-runs, whereas CO2e aids economic growth in the short-run but is extremely damaging to economic growth in the long-run, while in the both short- and long-runs health expenditure is not aiding the economic growth. This study provides policy recommendations on improving human health by advocating massive health expenditures, CO2e easing, promoting renewable energy use or low-emission energy, and steering the economy toward green economic growth.
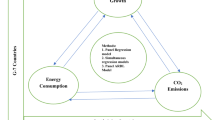
Graphical abstract

Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The United Nations member states aim to achieve Sustainable Development Goals (SDGs) by 2030. A principal goal of the SDGs is to improve healthy living and well-being (Goal-3) and ensure easy access to affordable, clean, and sustainable energy, and improve people’s health worldwide (Goal-7) (UN, 2015; WHO, 2018). Healthy living is a fundamental human right. However, recently, the COVID-19 pandemicsFootnote 1 have emphasized the need to rethink many health-related problems globally. The problems of healthy living and the increasing challenge of global warming are the result of deteriorating environmental quality around the world (Balan, 2016). The world’s population is undergoing a significant impact on its health status because of a lack of consideration and ignorance of many health-related factors such as CO2 emissions (CO2e), energy use, health expenditures (both public and private), environmental quality, and economic development. Energy usage and economic activities all have a major environmental impact, which contributes to an increasing worldwide burden of disease, lost work and school days, and harm to trade, transportation, agriculture, and other businesses (Jacobo & Viviana, 2013; Clark & Hammond, 2019). Therefore, the threat of global environmental change to human health and the economy is becoming more generally acknowledged, indicating the potential interaction among those variables.
Over the past few decades, the topic of environmental degradation and CO2e has been receiving considerable attention from both researchers and policymakers worldwide (Adebayo and Kirikkaleli 2021; Adeneye et al., 2021). From the 19th to the 20th centuries, global CO2e increased by 30% (Erdoğan et al., 2022). The problem of environmental deterioration and CO2e are among the major challenges facing the global economies, and has a significant negative impact on human health, income, society, environmental quality, economic growth, and the natural world (Muntean et al., 2018). Greenhouse Gases (GHGs) emissions have been universally acknowledged as contributing to climate change and global warming (Kirikkaleli et al., 2022). CO2e contributes approximately 75% of total worldwide GHGs emissions (Diffenbaugh, 2020); as a result, the global average surface temperature increased by 1.5 °CFootnote 2 as compared to the mid-1800s, causing a certain change in the climate and becoming an adverse effect on human lives, ecosystems, and long-term stability of the top 20 highest emitting economies (T20HEE)Footnote 3 (Gavurova et al., 2021; NASA, 2020). A prior study on the top emitting countries concluded that climate change causes additional 400 000 deaths each year, and by 2030, it will be responsible for 700 000 annual deaths (McKinnon, 2012). As CO2 temperatures rise, global climate change and extreme weather events, including floods, droughts, storms, heat waves, ice sheets melting, sea-level growth, and water system disturbances, are becoming more common (IPCC, 2021). The previous study on the “global climate risk index 2016” reported that over 15, 000 severe weather incidents occurred in the 10 developing countries between 1995 and 2014, resulting in over 525, 000 human deaths along with financial losses of more than 2.97 trillion U.S. dollars (Purchasing Power Parity) (Kreft et al., 2016). Japan was devastated by massive disasters in 2018, such as floods, severe weather events, the typhoon in Jebi, resulting in 1282 deaths and a 0.64 percent decline in gross domestic product (GDP). In Australia, a wildfire destroyed more than 8.4 million hectares, 1300 houses, 27 lives, and a record one billion livestock in 2019. The World Health Organization (2019) reported that approximately 1.6 million people suffer from lung cancer, 65 million from a "chronic obstructive pulmonary disorder," and around 334 million suffer from asthma, and these statistics are rapidly increasing. In this regard, problems regarding limiting environmental degradation are a global challenge that impacts all the countries. The global community, such as “the Kyoto protocol” which was signed in 1997 and implemented in 2005, “the Paris Climate Agreement (PCA)” in 2015, the COP26Footnote 4 in Glasgow, Scotland in 2021, held many climate agreements aimed at limiting global warming average temperature below 1.5 °C and protect human health worldwide, and the most recent “United Nations Climate Change Conference (COP27)Footnote 5 in Sharm El-Sheikh, Egypt” in 2022 which is important and timely for two reasons. First, the protracted war in Ukraine and the COVID-19 catastrophe compelled a number of countries to recommence coal-fired energy production, resulting in record-high CO2e. Second, the global crisis revealed our sensitivity to energy shortages and the necessity to develop alternate energy sources. Nonetheless, despite all of these climate agreements and policymaking, global temperatures continue to rise, and CO2e increased by 2.7% in 2018, prompting environmentalists, international organizations, and policy makers to focus more to identifying the critical factors and sources of CO2 influencing human health (Diffenbaugh, 2020).
The current study of casual relationships between health status, health expenditures, CO2e, energy use, and economic growth has recently received considerable attention from both developing and developed economies, particularly in the T20HEE. The T20HEE represents two-thirds of the world's population, which accounted for about (80%) of the world’s total CO2e (Mott et al. 2021). Countries such as China, the USA, India, Russia and Japan are the world highest emitters; therefore, global environmental success largely depends on them (Fig. 1). Meanwhile, these top-economies account for (77%) of global energy consumption and (81%) of global renewable energy, and their rapid economic growth contributes to (85%) of global GDP (World Bank, 2020). With such a great economic development, the top-emitting economies are among the world’s fastest-growing nations. According to World Bank statistics, global GDP has doubled between 1992 and 2019, with an average annual growth rate of 2.9% (World Bank, 2020). However, due to their large populations and rapid economic growth, these top economies have experienced a massive increase in energy demand as a whole, resulting in high amount of GHGs that are adversely impact on the environmental quality (Munir and Riaz, 2019; Zou and Zhang 2020). Thus, higher GHGs emissions are as a result of increased economic development and growth (Wang et al. 2022). As the economic development continue to increase in the top-emitting countries, environmental quality deteriorates due to the adverse effects of CO2e and polluting fossil fuels (Sinha et al., 2019), thus, posing a serious threat to the health condition of many countries (Li et al., 2022; Taghizadeh-Hesary et al., 2020). Globally, CO2 emissions are majorly caused by rising industrial activities and high energy use (Callan et al. 2009). According to the International Energy Agency (IEA), the top emitting economies' energy demand is expected to rise by 80% between 2013 and 2035 (IEA, 2017). The World Health Organization (WHO) reported that approximately (41%) of the world's population (about 2.8 billion people) are using fuel energy sources to fulfill their daily energy demands (WHO, 2015). The IEA (2017) estimated that the energy sector accounts for 69% of global CO2e, fuel energy (coal, gas, and petrol) generates about 44%, and the intensive usage of industrialization, manufacturing, transportation, and refrigeration has led to an excessive increase in other GHGs and is affecting environmental quality (Verma et al., 2021). Each country fulfills its energy demands using various types of energy sources based on several factors, including climate, culture, economic and social activities, population, war, and wealth (Gallo Cassarino et al., 2018). To alleviate environmental challenge, these top-emitting economies not only focus on reducing fossil fuels consumption, but also upsurge energy efficiency. Therefore, in order to achieve the SDGs, these selected countries needed significant improvements in their economies, particularly in their energy sectors. Due to the high population, rapid economic growth, excessive CO2e, and energy use, these top-economies are mostly prone to the threat of environmental degradation and climate change, therefore, it is crucial to understand the association and the factors of CO2e in these economies.

CO2 emissions (%) distribution based on top emitters in 2020
The deterioration of the environment and air quality increases the demand for healthcare expenditures in order to keep a healthy living (Alimi et al. 2019). Air pollution alone causes 9 million premature deaths globally each year, if urgent legislative and regulatory actions are not taken, deaths rate will increase in the coming future (Vohra et al., 2021). Furthermore, the World Health Organization (2019) declares that air pollution is expected to increase 250.000 additional deaths per year from 2030 and 2050. The increase in environmental pollution due to anthropogenic emissions such as CO2e significantly influence health expenditures (Ahmad et al., 2021). Health expenditure is continuously rising because governments are financing more in healthcare infrastructure and other healthcare facilities such as public health insurance. The demand for health insurance and healthcare infrastructure is increasing due to industrial development, infrastructure development, rise in energy consumption, urbanization, and rural-to-urban migration (Apergis et al., 2020). Furthermore, it is widely recognized that healthcare facilities play a vital role in reducing the adverse effects of climate change. The WHO (2011) reported that healthcare facilities represent between 3% to 8% of climate change footprints in developed countries, such as (8%) in the USA and (3%) in the United Kingdom. The total health expenditures were approximately 7.12% of GDP, among which the public health expenditures comprised (59.47%), and private health expenditures accounted for (40.28%), respectively, in the T20HEE (World Bank, 2020). Moreover, as life expectancy increases, the influence of health expenditures on CO2e and economic growth should not be neglected. According to the World Health Statistics (2019), the average age of the T20HEE was 77.6 years old. The complete detail of the average life expectancy of the T20HEE are provided in Fig. 2. Therefore, careful consideration is required of the issues of global CO2e, energy use, health expenditures (both public and private), and economic growth, promoting researchers and policymakers to conduct in-depth empirical research and provide critical analysis for the betterment of human health and life in the T20HEE.

The average life expectancy of top emitters in 2019
The previous studies have extensively examined the influence of CO2e on health expenditures and economic growth. At present, however, the empirical research on the link between health expenditure and CO2e is limited (Bilgili et al., 2021; Ghorashi and Alavi 2017). To this end, the first branch of studies focused on the impact of health expenditures on CO2e (Gündüz, 2020; Apergis et al., 2018). In addition, those studies neglected to consider the association between health expenditures and CO2e. Therefore, this study adds to the limited research to investigate the association between health expenditures and CO2e in the T20HEE. Furthermore, earlier conducted studies on health status have had mixed results and are often inconclusive, making it challenging to formulate consistent strategies in the health sector (Rahman and Alam 2021). These inconsistent results may be due to the different countries, methodologies, data, and variables, which create an ambiguous relationship among the related variables. Moreover, the challenges of environmental pollution have attracted worldwide attention due to its severe long-term effects on human health and economy. In spite of world attention, there are still some policy uncertainties in the current strategy due to the deficit of comprehensive and wide-ranging study, thus providing the opportunity for further research into the formulation and execution of appropriate policy initiatives for improving people’s health and environmental policy framework, to accomplish the SDGs. In this regard, this study is intended to examine the interaction of health status, CO2e, and energy use among the top 20 highest emitting economies.
The main contributions of the present study are the following: First, this study emphasizes T20HEE, which accounted for the large amount of the world population and significant contributors to global economic development and contribute considerably to CO2e. Second, to the best of our knowledge, this is the only study that investigates the relationship between health status, health expenditures (both public and private), CO2e, energy use, and economic growth using a dataset of the T20HEE from 2000 to 2019. Third, this study fills the gaps in previous studies by employing advanced econometric techniques, including the Cross-Sectional Augmented Distributed Lag (CS-DL) and Cross-sectional Augmented Autoregressive Distributed Lag (CS-ARDL) techniques by Chudik et al. (2016) to estimate the both short-run and long-run coefficients, where the two methods are complementary in nature. The combination of some of these countries consists of developing and developed countries as well as regions and continents; thus, in such an analysis, the CS-DL and CS-ARDL econometric procedures take into consideration three crucial elements of panel data, namely dynamics, heterogeneity, and cross-sectional dependence. Unlike earlier research studies, the current study applied econometrics analysis of second-generation panel methods such as the Pesaran unit root test, the Westerlund cointegration test, and the Dumitrescu-Hurlin Granger causality test was employed to determine the causal relationships between the variables. In addition, second-generation panel econometrics methods are regarded to be superior, advanced, and reliable to first-generation panel methods in terms of providing significant empirical results for guiding future policy decisions. This study, therefore, produces more effective and comprehensive estimates than previous studies in the context of T20HEE. Fourth, the Augmented Mean Group (AMG) and the Cross-sectionally Augmented Error Correction Method (CS-ECM) were employed to check the robustness. In addition, because slope coefficients change between nations and cross-country averages (and their lags) are proxies for unobserved shared characteristics, these models allow for common factors to influence countries. Eventually, the significance of the study is expected to help in achieving SDGs, particularly, SDG-3 and SDG-7, and these would serve as guiding principles for policymakers to use the outcomes of this study and improve human health by advocating massive health expenditures (both public and private), CO2e mitigation, increased use of renewable energy or low-emission energy, and steering the economies toward green economic growth.
Though the broad objective of this paper is to study the interaction of health status, CO2 emissions, and energy use among the top 20 highest emitting economies, it has the following specific objectives:
-
i.
To investigate whether health status is affected by CO2 emissions of the top 20 highest emitting countries;
-
ii.
To explore whether health expenditure is helping in mitigating CO2 emissions of the top 20 highest emitting countries;
-
iii.
To assess how energy use in the top 20 highest emitting countries is related to their production of CO2 emissions; and
-
iv.
To examine how energy use and CO2 emissions are related to the economic growth of the top 20 highest emitting countries.
The remaining sections of this study are distributed as follows: Section 2 will follow a literature review comprising both theoretical and empirical reviews; Section 3 describes research methodology, including data description, model specification, and estimation techniques; Sections 4 and 5 present results and discussion of the results, respectively; and the final Section 6 provides conclusion and recommendation for policy.
Literature Review
The topic setting of this study has theoretical justification from several well-known theories, including the Nightingale's Environmental Theory, Life Course Health Development (LCHD) framework, the Carbon Dioxide Theory, Health Expenditure and Carbon Emissions Systematic Linkage Model, and Environmental Kuznets Curve (EKC) Theory. On the other hand, the empirical review of the literature on the relationship between health status, CO2 emissions (CO2e), energy use and economic growth has been divided into three categories: (i) health status and CO2 emissions; (ii) energy use and CO2e; and (iii) energy use, CO2e and economic growth.
Theoretical Review
From a theoretical perspective, several theorists have shown a relationship between environmental problems and health consequences throughout the time. Some of these theories or postulations include: (1) The Nightingale's Environmental Theory, which was first proposed by Florence Nightingale in 1859 in England, which remains relevant today in health discourse, ties the individual's health is determined by his environment. In this theory, Florence Nightingale addresses that clean water, efficient drainage system, cleanliness/sanitation, pure air, sufficient food, and sunlight are crucial component of an environment that will assure good health outcomes or status of population. The Environmental Theory has led to improved human health. A healthy environment is important for healing. She believed that “nature alone cures.” (2) The Life Course Health Development (LCHD) framework, which was published by Halfon and Hochstein's in 2002, which relates variations in health of an individual to a number of determinants operating in a nested genetic, biological, and environmental network. Furthermore, based on to the LCHD framework, health development is an adaptive process that is influenced by biological, economic, environmental, genetic, and social circumstances. As a result of these developing contributing factors, health outcomes or status are also invariably changing. Considering comprehensive empirical assessment of the association between these variables (biocapacity, environmental quality, human capacity, and health status or outcomes), the research has been deficient. (3) The Carbon Dioxide Theory, as the amount of CO2 in the atmosphere increases, the atmosphere becomes opaque over a longer frequency interval. As a result, emitted radiation is trapped more efficiently close to the surface of the earth, which causes the temperature to rise. According to the most recent figures, if the amount of CO2 in the atmosphere were to be halved, the surface temperature would drop by 3.8 degrees Celsius, while if the amount were to be doubled, it would cause a rise in temperature of 3.6 degrees Celsius. These results come from calculations that used the most recent data available. The carbon dioxide theory, which was first proposed by John Tyndall in 1861. The first significant computations were necessarily done using very approximative techniques. Because of carbon dioxide, there are hundreds of spectral lines which are caused by absorption, and each of these lines occurs in a sophisticated pattern with fluctuations in the intensity and the width of the spectral lines. Furthermore, the pattern does not appear the same even at all heights in the atmosphere due to the fact that the breadth and strength of the spectral lines change depending on the temperature and pressure of the environment. A relatively accurate solution to the problem of the impact of CO2 on surface temperature has only recently been possible due to accurate infrared measurements, availability of a high-speed electronic computer, and the theoretical advancements. (4) Health Expenditure and Carbon Emissions Systematic Linkage Model postulated that spending money on healthcare equipment that is efficient in its energy consumption is a powerful lever for reducing carbon emissions and addressing rising operational energy costs for care providers. Specifically, the model stated that this would be the case if the expenditure was made on energy-efficient healthcare equipment. According to the most recent report published by the World Economic Forum in 2022 on how the healthcare industry can reduce its carbon footprint, hospital buildings have the highest energy intensity of all publicly funded buildings. As a result, hospital buildings emit 2.5 times more greenhouse gases than commercial buildings. Moreover, the amount of energy that is used by medical equipment is yet another area that has the potential to have a significant effect on large-scale, energy-intensive activities such as hospitals. Therefore, allocating funds for healthcare toward the purchase of energy-efficient medical equipment may have a significant bearing on the amount of carbon footprint reduced. (5) The Environmental Kuznets Curve (EKC) hypothesis was proposed by Kuznets (1955) regarding the income inequality and economic development and was named after it. The EKC examine the relationship between several indicators representing environmental pollution and per capita income. The EKC hypothesis was put forward by Grossman and Krueger (1995), which refers to an inverted U-shaped relationship between environmental degradation and per capita income. The term EKC argues that environmental pollution rises in the early steps of economic growth, when a certain level of income per capita are reached, the economic growth contributes to environmental improvement (Bilgili et al., 2021). For example, advancing production and consumption technologies for manufacturing processes, raising environmental awareness, increasing the usage of environmental-friendly technologies, establishing environmental protection laws, etc. Therefore, Ulucak and Bilgili (2018) stated in the prior study that the EKC hypothesis found an inverse U-shape association between per capita income and environmental deterioration. Numerous studies have documented EKC’s existence, while others have found no evidence of its existence, and still others have discovered EKCs in various shapes, thus leaving the conclusion ambiguous (Ahmad et al. 2020). Chen et al. (2020) confirmed conventional EKC while using China's city-level data.
Empirical Review
CO2 Emissions, Health Expenditure, and Health Status Nexus
The first section of the study looked at the association between health and CO2 emissions (CO2e) by employing a number of methodologies, data sets, and locations. The important issue of the influence of CO2e on health status is clearly revealed by many recent studies in the context of developing and developed economies. In this regard, Yang and Liu (2018) examine the impact of environmental deterioration on human health and health inequality from the 2014 national survey of “China Family Panel Studies (CFPS)”. The 2014 survey includes approximately 16000 households from 25 regions. They revealed that environmental pollution has a significantly negative impact on human health, and air pollution contributes to increasing health inequality. Another group of studies reported the same findings: Ahmad et al. (2020) for China, Balan (2016) for 25 European Union (EU) countries, Osabohien et al. (2021) for Nigeria, Rahman and Alam (2021) for SAARC-BIMSTEC countries, and Taghizadeh-Hesary et al. (2020) for middle-income Asian countries. Igbinedion (2019) identified environmental pollution as having a significant impact on neonatal life expectancy, and both enhanced sanitary facilities and public health expenditure had a significant and positive impact on health status and increased longevity in Nigeria from 1990 to 2016.
Furthermore, several empirical studies have explored the link between CO2e and health expenditures. In this regard, several recent studies employing different estimation techniques revealed that the increase in healthcare expenditures would significantly increase CO2e in various countries around the world. For example, Ahmad et al. (2021) in China; Alimi et al. (2019) for 15 ECOWAS countries; Blázquez-Fernández et al. (2019) for 29 OECD countries; and Khan et al. (2020) for 58 Belt and Road Initiative countries. Bilgili et al. (2021) applying the quantile regression analysis, they ascertained that both public and private health expenditures could help to decrease the adverse effects of CO2e. Ganda (2021) revealed that there is a negative linkage between health expenditures and CO2e. When the effect is disaggregated, public-health expenditure is positively related to CO2e, whereas private-health expenditure is adversely related to CO2e in the BRICS countries during 2000-2017 by using Fully Modified Ordinary Least Squares (FMOLS), Vector Error Correction Model (VECM), and the Dumitrescu-Hurlin causality tests. A recent study by Apergis et al. (2020) examined the long-run association between environmental pollution and healthcare expenditures among four global income groups in 178 countries during the period 1995–2017. According to the findings, they noted that a 1% increase in CO2e will increase health expenditures by about 2.5%. Apergis et al. (2018) revealed that both usage of renewable energy and health expenditures caused a reduction in CO2e, while real GDP leads to increase the CO2e levels in African countries during the period 1995-2011. Zeeshan et al. (2021) found that CO2e and environmental pollution positively increase the amount of household health expenditures in both the short- and long-runs. Also, the results demonstrate that there is a bidirectional link between household health spending, CO2e, and environmental pollution, indicating that CO2e significantly increases health expenditures in China from 1990 to 2019 by using the Nonlinear Autoregressive Distributed Lag (NARDL) model.
Energy Use and CO2 Emissions Nexus
The second section of the study focuses on the association between different types of energy usage and CO2e. Scholars have used a number of methodologies and data sets to conduct a study in various countries, regions, and continents. In this regard, Ummalla (2019) applying the Autoregressive Distributed Lag (ARDL) and Panel Quantile Regression (PQR) model to examine the effects of hydroelectric energy consumption on CO2e in the BRICS countries during the period 1990-2016. They discovered that using hydroelectric electricity results in lower CO2e emissions. Another recent study by Ashin and Muhammed (2020) examines CO2e and economic growth in India using Artificial Neutral Networks (ANN) and machine learning methodologies. They revealed that transitioning from fossil fuels (coal, gas, and petrol) to renewable energy can significantly minimize CO2e without affecting economic growth. Zou and Zhang (2020) investigate the linkage between CO2e, energy consumption, and economic growth in 30 Chinese provinces from the period 2000–2017. Employing the Spatial Durbin Model (SDM), they observed a two-way association between CO2e and energy use, implying that CO2e and energy use are related to a negative spatial spillover effect on CO2e in neighboring provinces and cities. Adeneye et al. (2021) determined the relationship between CO2e and energy use was highly significant in Asia during 2000–2014 by applying panel data models with dynamic common correlated effects. Litavcová and Chovancová (2021) employed the ARDL Model and found that energy usage is a significant long-run influence on CO2e across 14 Danube countries from 1990 to 2019. Salari (2021) identified a long-run relationship between several kinds of energy use and CO2e in the U.S. In addition to this, non-renewable energy and household energy are positively associated with CO2e, whereas renewable energy (RE) has a negative association with CO2 in the U.S. from 1997 to 2016. Murshed et al. (2021) noted that the usage of RE contributes to the sustainability of the environment in Bangladesh. Similarly, several prior studies confirmed that RE contributes negatively to environmental deterioration by Sharif et al. (2020) in Turkey, Destek and Sinha (2020) in the Organization for Economic Cooperation and Development (OECD) countries and Kayani et al. (2020) in the top 10 highest emitter countries. Bekun et al. (2021b) investigate the applicability of the conventional Environmental Kuznets Curve (EKC) with an extension for the case of emerging industrialized economies (E7) of the world, including China, India, Brazil, Mexico, Russia, Indonesia, and Turkey during the period 1995-2016. Applying second-generational panel econometrics strategies such as the Augmented Mean Group estimator, the Common Correlated Effects Mean Group estimator, the Driscoll-Kraay and Dumitrescu and Hurlin Causality analysis. The EKC phenomenon is supported by the declining impact of fossil fuel-based energy use in the bloc. However, renewable acts as a panacea for reducing pollution emissions, because RE has a negative and statistical association with CO2e. Bekun et al. (2021a) investigate the long-term and causal relationship between tourism development and the real income level in EKC framework for emerging industrialized economies (E7). Employing second-generation panel estimation techniques, in conjunction with the Driscoll-Kraay robust estimator, the findings support the notion that GDP growth and non-renewable energy degrades environmental quality. Adebayo et al. (2023a) applied the CS-ARDL technique to analyze the complex relationship among technological innovation, use of renewable energy sources, natural resources, and CO2e in the context of BRICS countries during the period 1990 to 2019. The findings discovered that natural resources, renewable energy consumption, and technological innovation increases environmental sustainability by reducing CO2e both in the short- and long-runs.
Energy Use, CO2 Emissions, and Economic Growth Nexus
The third section includes many studies that aim to investigate the link between environmental consequences and economic growth, which is known as the "Environmental Kuznets Curve (EKC)." A number of studies have been conducted to investigate the relationship between CO2e, energy consumption, and economic growth by employing a number of data sets, locations, and methodologies in the both developing and developed countries around the world. In this regard, Pao and Chen (2019) revealed that a long-run balanced relationship exists between CO2e, energy use, and economic growth for the developed countries by employing the panel cointegration test. Adebayo and Akinsola (2021) and Cai et al. (2018) applied different estimation techniques and discovered that changes in economic growth contributed to changes in CO2e. They also found that both short- and long-runs associations exist between economic growth and CO2e in Thailand and the G7 countries. Azam et al. (2016) employ the FMOLS model to examine the impact of CO2e on economic development in particular higher CO2 emitting countries from 1971 to 2013. They revealed that CO2e have a significantly positive influence on economic growth for China, Japan, and the USA, while significantly negative for India. Mensah et al. (2018) employing the STIRPAT model to evaluate the influence of innovation on CO2e at the individual level in 28 OECD countries from 1990-2014. The economic-EKC model was found to be inapplicable for most economies because rising GDP per capita increases CO2e in most OECD countries while reducing emissions in only a few OECD countries. Ummalla (2019) uses the ARDL model and PQR estimations to examine the effects of hydroelectric energy consumption on economic growth in the context of BRICS countries (Brazil, Russia, India, China, and South Africa) from 1990 to 2016. The findings support the idea that hydropower consumption is related to economic growth. Using dynamic simultaneous equation models, Ghorashi and Alavi (2017) examine the link between CO2e, health spending, and economic growth in Iran during 1972–2012. According to the empirical findings, a bidirectional causal relationship exists between CO2e and economic growth, whereas health expenditures and economic growth exhibited a one-way relationship. Litavcová and Chovancová (2021) identified that economic growth has only a long-term impact on CO2e by employing the ARDL model in 14 Danube Region countries during the period 1990–2019. Employing multi-spatial Convergent Cross Mapping (CCM), Liu et al. (2019) have discovered various causal relationships in the G7 countries, including unidirectional, bidirectional, and neutral nexus; whereas a bidirectional nexus exists between energy use and CO2e has been demonstrated in China and India from 1965 to 2017. Ssali et al. (2019) revealed a bidirectional causation exists between energy use and CO2 in the short-run, but in the long-run, there is one-way causation from energy use to CO2 in six Sub-Saharan African countries from 1980 to 2014 using the ARDL model. They found a rise in economic growth increases CO2, while an increase in economic growth squared results in a decrease in CO2. As a result, the EKC theory is supported by the positive and negative effects of economic development, as well as their square. Irfan et al. (2023) demonstrate the dynamic impact of the tourism industry on economic output, energy consumption, and environmental quality in China from 2001Q1 to 2019Q4. Using the ARDL approach and the Gradual shift causality method, they revealed that all tourism industry sub-sectors have a significant and positive impact on economic growth and energy consumption, while tourism-related travel consumes more energy. Similarly, entertainment and shopping boost the economic development more than other sub-sectors. Interestingly, globalization has had a negative impact on air pollution and GHGs emissions in the long-run. Adedoyina et al. (2021) revealed that rising energy usage, real GDP per capita, and tourism across the four EU macro regions contribute to increase in CO2e by employing the one-step system Generalized Method of moment (GMM) model in the 26 EU member states during the period 1995-2018. Caglar et al. (2021) using second-generation panel methodologies to investigate the factors that influence CO2e in the BRICS economies, including the contribution of partnerships' investments in energy and economic complexity from 1990-2018. The results demonstrate that improvements in economic complexity and trade openness promote environmental quality. On the other hand, environmental deterioration is a result of economic expansion, use of natural resources, and public-private partnerships. Bekun (2022) investigates the impact of renewable energy, non-renewable energy, economic growth, and investment in the energy sector on CO2e in the Indian economy. Using Canonical Cointegration Regression (CCR), Fully Modified Least Squares (FMOLS), and Dynamic Least Squares (DOLS), they demonstrated that, despite the economic growth trajectory, renewable energy acts as a panacea for sustainable development. However, there is positive association exists between CO2e and both non-renewable and GDP growth. Adebayo et al. (2023c) employ Wavelet local multiple computation (WLMC) to analyze the time- and frequency-varying effects of hydroelectricity energy consumption, natural gas energy consumption, and economic growth on environmental sustainability in the United States of America from 1965/Q1 to 2020/Q4. The findings provide new insights into how CO2e are caused by economic growth, which is demonstrated by a positive linkage exists between both factors at short-term and long-term time-frequencies. Adebayo et al. (2023b) employ CS-ARDL method, common correlated effects mean group (CCEMG), and AMG to investigate the impact of country risks and renewable energy usage on environmental quality and economic growth in MINT countries (Mexico, Indonesia, Nigeria, and Turkey) from 1990-2018. The findings indicated that economic growth, political risk, trade openness, and urbanization, all contribute to an upsurge in ecological footprint; nevertheless, environmental quality is positively influence by renewable energy use as well as economic and financial risks.
Literature Gap
According to the exploration of related literature, it is evident that relatively few studies have investigated the combined relationships among health status, both public and private health expenditures, CO2 emissions, and energy use, particularly in the top emitting economies. In addition, previous studies result on health status were often inconclusive and not encouraging to formulate consistent strategies towards a better health and environmental policy framework (Rahman and Alam 2021). Furthermore, earlier studies have mainly focused on the influence of CO2e on health expenditures and economic growth; however, minimal has studied the link between health expenditures and CO2e (Ghorashi and Alavi 2017). Moreover, unlike previous studies, this study fills the gaps of methodological advancement by the use of Cross-Sectional Augmented Distributed Lag (CS-DL) and Cross-sectional Augmented Autoregressive Distributed Lag (CS-ARDL) advanced techniques robust against dynamics, heterogeneity, and cross-sectional dependence. Specifically, we examine the unit root test, panel cointegration analysis, and causal relationships among these variables. Therefore, the current study aims to fill the existing gaps in the prior studies and provide a prudent way of exploring the interaction of health status, health expenditures (both public-private), CO2e, energy use, and economic growth in the T20HEE and the formulation of appropriate environmental policy implications in the selected countries.
Research methodology
Data description
The variables used in this study include health status, which following Rahman and Alam (2021) was proxied by life expectancy at birth (HS), public health expenditure (% of total health expenditure) (PBHEX), private health expenditure (% of total health expenditure) (PRHEX), total health expenditure (% of GDP) (HEX), CO2 emissions (in kilotons) (CO2), energy consumption (in quadrillion Btu) (ENERGY), and economic growth (GDP growth rate) (GDPGR). In addition to following the existing literature, the rationale for choosing the variables is that a combination of both public and private health expenditures ensures better health status; excessive CO2e damage improves health outcomes; the green economy reduces energy consumption and provides adequate facilities for good health status, and economic growth contributes to improved amenities for ensuring health status. However, the data were sourced from the "World Development Indicators (2020)" and the "U.S. Energy Information Administration international energy statistics database (2020)". The data range is for the period 2000 to 2019 from the T20HEE, which comprises "China, the United States, India, Russia, Japan, Iran, Germany, Indonesia, the Republic of Korea, Saudi Arabia, Canada, South Africa, Brazil, Mexico, Australia, Turkey, the United Kingdom, Italy, France, and Poland." All the variables are in their natural values; thus, the paper did not take the log of any because none of the HS, CO2, and ENERGY values are up to 100, while GDPGR, PBHEX, PRHEX, and HEX are all-in rates. As a result, there is no need to take either log.
Model specification
Following the objectives, three models will be estimated: to achieve the first objective, the first model specified in equation (1); to achieve the second and third objectives, the second model specified in equation (2); and to achieve the fourth objective, the last model specified in equation (3).
where for model one, the dependent variable is health status, while the independent variables are CO2 emissions, health expenditures, and economic growth. For model two, the dependent variable is CO2 emissions, while the independent variables are health expenditure, energy use, and economic growth. Lastly, for model three, the dependent variable is economic growth while the independent variables are energy use, CO2 emissions, and health expenditure. However, a represents the constant term, β1, β2, and β3 represent the respective coefficients of the parameters, e represents the error term, and i represents country i at time t.
Estimation techniques
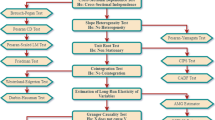
The estimation techniques of this study will start with the graphical illustration of data to understand the nature of the data trend. The second method is the descriptive analysis for understanding the statistical characteristics of the data. The third method is the multicollinearity test. The fourth method is the heterogeneity test for checking cross-section dependence (CD) in the panels, such as Pesaran (2004) test, on which the majority of the research relies. The fifth method is the panel unit root tests for checking the stochastic properties of the panels, which were employed as none of the panels are free from cross-section dependence, such as the cross-sectional Augmented Pesaran and Shin (CIPS) panel unit root test of Pesaran (2007) that deals with the problem of cross-section dependence and heterogeneous slope coefficients. The sixth method is the panel cointegration test, which will be used to check for the long-run association between the variables, such as the Westerlund (2007) panel cointegration test, because the panels are cross-sectionally dependent and it does not necessitate previous knowledge of the order in which variables are integrated (Bhujabal et al., 2021), even though the significance or otherwise of the Error Correction Term (ECT) will be used for reaffirming the presence of the cointegration. The seventh method is the execution of the Cross-sectional Augmented Distributed Lag (CS-DL) and Cross-sectional Augmented Autoregressive Distributed Lag (CS-ARDL) techniques by Chudik et al. (2016) to estimate both short-run and long-run coefficients, where the two methods are complementary in nature. Nonetheless, this study will employ Eberhardt and Teal (2010) Augmented Mean Group (AMG) and the Cross-sectionally Augmented Error Correction Method (CS-ECM) for robustness checks, both of which produce better results with unobserved common factors, non-stationarity, cross-section dependence, and heterogeneous slope (Wahab et al., 2021). Both approaches are suitable for nonlinear or nonstationary variables in complex common factor structures where variables may be influenced by other factors. The reason for choosing the AMG is that it employs explicit estimates for unobserved common factors (ft) that exhibit a common dynamic process as a meaningful construct, whereas the CS-ARDL and CS-DL estimators employ implicit estimates for ft using cross-sectional averages of regressors. While the reason for choosing the CS-ECM estimator is that it is a second approach to the CS-DL technique that also considers multifactor error structure, Lastly, the Dumitrescu-Hurlin (2012) Granger causality test can be used to check the direction of causality between pairs of variables. Fig. 3 presents the flowchart of the empirical analysis.

Flowchart of the empirical analysis
Cross-Sectional Augmented Autoregressive Distributed Lag (CS-ARDL) Model
The classic ARDL model is based on cross-sectionally independent error factors and homogenous units (countries). Error terms are likely to be cross-dependent because the models incorporate unobserved shared components. As a result, the fundamental ARDL model has been adjusted to account for both slope variation and error cross-sectional dependency. Therefore, Chudik et al. (2016) developed the CS-ARDL technique, a recent and advanced ARDL type estimator that can handle cross-sectional dependence in the presence of I(0) or I(1) order of integration and generate pooled long-run type estimates. The estimator also takes into consideration omitted variable bias. Apart from cointegration among variables, the only reason for using this type of estimator is that the model has a dynamic specification, which allows for weak exogeneity among the regressors to be taken into account and residuals to be no longer linked. The CS-ARDL approach, on the other hand, can be stated as follows:
when f is an n × 1 vector of unobserved common factors; \({\tau}_i^{\prime }\) is the corresponding factor loading and eit are the idiosyncratic errors. According to the both studies by Chudik et al. (2011) and Chudik et al. (2017), these idiosyncratic errors could be serially, cross-correlated, or uncorrelated with the common components. Unobserved common factors affect variables differently across nations, leading in erroneous cross-section dependence.
where Xi, t − 1 are the vector of the explanatory variables. The assumption is that the explanatory variables could be influenced by the unobserved common factors 𝑓t, \({\pi}_i^{\prime }\) is the n × m matrix of factor loadings, and 𝑣it are the idiosyncratic errors associated with Xi, t − 1 which are believed to be uncorrelated with 𝜀it.
According to Chudik et al. (2011), the common factor structure can be expressed as a combination of a finite number (mfs) of strong factors (\({f}_{it}^s\)) that can be correlated with the regressors of the original model, and a finite number (mfw) of weak, semi-weak, and semi-strong factors \({f}_{it}^w\) that may affect a subset of the sample countries. Furthermore, according to Chudik et al. (2017), strong factors or shocks include structural changes, such as changes in the commodity price shocks, global financial cycle, and interest rates.
The weak, semi-weak, and semi-strong variables include spillovers from agricultural production, climate factor, domestic consumption, domestic industrial activity, research and development, geographical proximity, and natural resources (Eberhardt and Vollrath, 2016; Eberhardt et al., 2013; Holly et al. 2010).
Cross-Sectional Augmented Distributed Lag (CS-DL) Model
Despite the fact that the CS-ARDL technique can address cross-sectional dependence in the presence of I(0) or I(1) order of integration and obtain pooled long-run type estimates while accounting for omitted variable bias and having a dynamic specification, because the CS-ARDL technique calculates the short-run coefficients first and the residuals are no longer calculated (Pesaran 2015). However, there is a problem when the rate of convergence to the long-run estimate is slow and the time dimension is insufficient (Chakraborty & Mazzanti, 2021). Furthermore, another problem may develop if the sampling uncertainty is considerable and the short-run coefficient is subject to a slight T bias (see Pesaran 2015, page 782). As a result, Chudik and Pesaran (2015) developed a new estimation method in which the long-run coefficients are estimated without first calculating the short-run coefficients. The following is the CS-DL methodology, which is based on the ARDL method:
where \({\overline{x}}_t={N}^{-1}\sum\limits_{i=1}^N{x}_{it}\) and \({\overline{y}}_t={N}^{-1}\sum\limits_{i=1}^N{y}_{it}\) and\({p}_{\overline{x}}\)is set equal to integer of T2/3, \(p={p}_{\overline{x}}\) and \({p}_{\overline{y}}\) is set to zero. Therefore, the mean group estimator for cross-sectional augmented distributed lag (CS-DL) can be stated as:
and
The CS-DL pooled estimator of the long-run coefficients can be written as:
Pesaran (2006) uses a heterogeneous number of regressors in his CCE estimator, but in the CS-DL estimator, θMG and θP incorporate ρT lags of ∆xit and its cross-sectional averages. The length of ρT increases with T, and the optimal lag length can be determined using Chudik et al. (2016), Chudik and Pesaran (2015), and Pesaran (2006).
Nonetheless, the CS-DL and CS-ARDL econometric procedures take into consideration three crucial elements of panel data, namely dynamics, heterogeneity, and cross-sectional dependence.
Results and Discussions
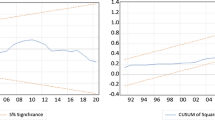
Fig. 4 is the graphical representation of health status (HS), CO2 emissions (CO2), energy use (ENERGY), public health expenditure (PBHEX), private health expenditure (PRHEX), health expenditure (HEX), and GDP growth rate (GDPGR) of the top 20 highest emitting economies. According to the figure, HS, Energy, PBHEX, and HEX displayed an upward trend, though the trend of energy declined in the year 2009 but picked up by the year 2010, while PRHEX portrayed a downward trend. CO2 increased until 2008, and then slowed until 2010, when it peaked in 2011, after which it plateaued until 2014, when it began to decline. GDPGR fluctuated throughout the period, but there was a huge decline in the year 2009. As a result, the trends of energy, PBHEX, and HEX moved in the same direction as that of HS, whereas PRHEX moved in the opposite direction, but for CO2 and GDPGR, it is a fluctuating direction that cannot be directly compared. Looking at the trends in recent years, it can be seen that HS, ENERGY, PBHEX, PRHEX, and HEX are increasing, but CO2 and GDPGR are decreasing.

Graphical representations. Source: Author’s Computation. Note: HS stands for health status, CO2 stands for CO2 emissions, ENERGY stands for energy use, PBHEX stands for public health expenditure, PRHEX stands for private health expenditure, HEX stands for health expenditure, and GDPGR stands for GDP growth rate.
Table 1 displays the statistical characteristics of the variables. According to the table, the means and standard deviations of HS, CO2, ENERGY, PBHEX, PRHEX, HEX, and GDPGR for the countries are 77, 8.9, 16.6, 62.7, 37.2, 7.4, 3.2, and 4.9, 5.1, 21.5, 16.5, 16.2, 3.1, 3.2, respectively. Therefore, for HS, CO2, PBHEX, PRHEX, HEX, and GDPGR the mean value is greater than the standard deviation; thus, it can be stated that the data were not widely dispersed in the countries, but for ENERGY it is. The countries' maximum and minimum statistics of HS, CO2, ENERGY, PBHEX, PRHEX, HEX, and GDPGR are 84, 20.5, 101.2, 84.3, 79.8, 17, 14.2 and 62.1, 0.9, 2.9, 18, 15.7, 3, -7.79, respectively. The skewness shows that the elements of CO2, ENERGY, PRHEX, HEX, and GDPGR of the countries are positively skewed, but that of HS and PBHEX is negatively skewed, so none is 0; also, none of the kurtosis is 3. This highlights that the distribution of the individual series is not likely to be symmetrical and passively explosive. Yet, according to the p-value of the Jarque-Bera statistic, the distribution of all the variables seems to be volatile, as the p-value is significant at the 1% level.
Table 2 displays the correlation analysis of the variables for each of the three models. In model I, HS is moderate negative and positive correlated with CO2 and HEX, respectively, while GDPGR is weakly but positively correlated with HS. For model II, CO2 is moderate positive correlated with ENERGY, while HEX, and GDPGR both are moderate negative related to CO2. For model III, there is a high positive correlation between GDPGR and ENERGY but a moderate negative correlation between GDPGR and CO2 whereas there is a very low negative correlation between GDPGR and HEX.
Table 3 reported the multicollinearity test results for each of the three models. The results indicated that all the variables evidenced that there is a serious multicollinearity problem between PBHEX and PRHEX variables as their variance inflation factor (VIF) is up to 10 and beyond. This depicts that between the two major remedies to the multicollinearity issue, such as dropping one of the variables or merging the two variables, the appropriate measure, in this case, is to merge the two variables, such as public health expenditure (PBHEX) and private health expenditure (PRHEX), which means total health expenditure (HEX). Therefore, total health expenditure will be used henceforth.
Table 4 presents the Pesaran (2004) test for cross-sectional dependence (CD) of panel variables such as health status, CO2 emissions, energy use, health expenditure, and economic growth. The results indicated that all the variables rejected the null hypothesis of no cross-sectional dependence in the data. Thus, it is concluded that there is cross-sectional dependence. Therefore, the Pesaran (2007) panel unit root test is used because none of the variables are free of cross-section dependence, which is indifferent, or rather, not sensitive to cross-section dependence, and will be used in place of the panel conventional unit root test.
Table 5 shows the results of the Pesaran (2007) CIPS panel unit root test. The CIPS results show that the variables HS and GDPGR reject the null hypothesis of homogeneous non-stationary at 1% level, whereas CO2, ENERGY, and HEX do not reject the null hypothesis of homogeneous non-stationary at 1% level. The results of the panel unit root test indicate that all the variables are found to be stationary at the first difference at the 1% level. This demonstrates that the variables' order of integration is a mixture of I(0) and I(1).
Table 6 displays the panel cointegration test results obtained applying the method by Westerlund (2007) for each of the three models. According to the results, the test rejected the null hypothesis of "no cointegration" among the variables at 1%, 10%, and 1% for the models, respectively. Therefore, this indicates that the variables in each of the models are linked in a long-term cointegration relationship among the selected variables. This enabled the use of the CS-DL and CS-ARDL models.
Table 7 displays the results of the CS-ARDL, CS-DL, CS-ECM, and AMG techniques for both the short- and long-runs coefficients, except for the AMG technique, which has no short-run coefficients. According to the CS-ARDL and CS-DL results, the coefficient of CO2 is negatively related to HS in the short-run, and the CS-ECM technique has also confirmed that it is negatively related to HS. The impact is significant at the 5% level, but the CS-DL technique's impact is higher, showing that a unit increase of CO2 kilotons will deteriorate HS by 0.8. This means that in the short-run, an increase in the production of CO2e is weakening the health status of people. The coefficient of HEX is positively and negatively related to HS, according to the CS-ARDL and CS-DL techniques, respectively, and both are significant at 10% and 5%, respectively. Since, both are significant in the opposite direction, the decision will be based on economic theory, indicating the relationship should be positive. Hence, a 1% increase in HEX will induce a 0.2 rise in HS. This shows that in the short-run, an increase in HEX improves the HS of people in the T20HEE. However, none of the techniques found the coefficient of GDPGR to be significant, though it was positively related to HS. This implies that economic growth is negligible in the short run, improving the countries' HS. The coefficient of ECMt-1 is negative and significant at a 1% level, as shown by CS-ARDL and reconfirmed by CS-ECM techniques. The significance level confirms the earlier cointegration test result that there is a long-term association between the variables, and the model will automatically adjust itself by 61% (0.61) every year if there is a short-term shock.
In the long run, according to the estimates of the CS-ARDL and CS-DL, the coefficient of CO2 is negatively related to HS, which is also confirmed by the AMG technique, but is still significant as shown by all the techniques. This means, unlike in the short-run, an increase in the production of CO2e is negligibly deteriorating the HS of people in the long-run. The coefficient of HEX is positively related to HS according to the techniques and also confirmed by the CS-ECM and AMG techniques, both of which are significant at the 5% level, which is also confirmed by the AMG technique. But the impact of CS-DL is higher, where a 1% increase in HEX will induce a 1.0 rise in HS. This implies that an increase in HEX improves individuals' HS in both the short and long run. However, in the short-run, none of the methodologies found the GDPGR coefficient to be significant in the long-run, implying that in the long-run, the GDPGR has no impact on the health of the people living in those countries. In all four techniques, the p-value of the heteroscedasticity test statistic of the estimated technique residuals is insignificant, which tells us that the residuals are homoscedastic, indicating healthy estimates of the techniques.
Table 8 shows the results of the CS-ARDL, CS-DL, CS-ECM, and AMG techniques for both the short- and long-runs coefficients, except for the AMG technique, which has no short-run coefficients. The short-run results show that the estimates of CS-ARDL and CS-ECM are the same but completely opposite in sign, except for the coefficient of ECMt-1. Based on economic theory or following economic assertion, the results of CS-ARDL are consistent, whereas those of CS-ECM are diametrically opposed. Nonetheless, they are exactly the same in the long-run. Hence, the attention in the short-run will be on the CS-ARDL and CS-DL techniques, while in the long-run, it will be on all four techniques in the analysis. According to the estimates of the CS-ARDL and CS-DL, the short-run results indicate that the coefficient of Energy is positively related to CO2, but only the impact of the CS-ARDL technique is significant at the 1% level, where a 1 unit increase in Quadrillion Btu of Energy will raise the production of CO2 by 0.7. This means that in the short-run, an increase in energy use is causing the release of more CO2e in these countries. Furthermore, the coefficient of HEX is negatively and positively related to CO2 according to the CS-ARDL and CS-DL techniques, respectively, but neither is statistically significant. Hence, the decision will be based on economic theory, and accordingly, the relationship should be negative. This suggests that in the short-run, an increase in HEX is negligibly reducing the production of CO2e in the T20HEE. However, none of the techniques found the coefficient of GDPGR to be significant, though negatively related to CO2. This means that, in the short run, economic growth is moving in the direction of countries reducing CO2 emissions. The coefficient of ECMt-1 is negative and statistically significant at a 1% level, as shown by CS-ARDL and reconfirmed by CS-ECM techniques. The significance re-endorses the earlier cointegration test result that there is a long-run association between the variables and that in the event of a shock in the short-run, the model will automatically adjust itself by 89% (0.89) per annum.
In the long-run results, according to all techniques, the coefficient of Energy is positively associated with CO2 and statistically significant at least at the 5% level, with the exception of the CS-DL technique, which is in the opposite sign and insignificant, thus, contradicting economic theory. However, the coefficient of the CS-ARDL technique is higher, where a 1 unit increase in Quadrillion Btu of Energy will raise the production of CO2 by 0.9. This indicates that an increase in energy use causes the release of more CO2 in the countries in both the short and long run. From all the techniques, the coefficient of HEX is negatively associated with CO2 and statistically significant at 10%, 10%, 10%, and 5% levels, respectively, but that of the CS-DL technique is higher where a 1% increase in HEX will reduce CO2 by 0.7. This suggests that, unlike in the short-run, an increase in HEX reduces CO2e in the long-run. However, none of the techniques found the GDPGR coefficient to be significant in both the short and long runs, with the exception of the AMG technique, which shows that GDPGR is negatively related to CO2 and the impact is statistically significant at the 5% level, with a 1% increase in GDPGR reducing CO2 by 0.03. This implies that in the long-run, the economic growth of the T20HEE countries is assisting in the reduction of CO2e in the countries. In all the four techniques, the p-value of the heteroscedasticity test statistic of the estimated techniques residuals is insignificant, indicating that the residuals are homoscedastic; therefore, the techniques' estimates are healthy.
Table 9 presents the results of the CS-ARDL, CS-DL, CS-ECM, and AMG techniques for both the short- and long-runs coefficients, except for the AMG technique, which has no short-run coefficients. In the short-run, according to the estimates of the CS-ARDL and CS-DL, the coefficient of Energy is positively related to GDPGR and is significant at 10% and 1% levels, respectively, also confirmed by the CS-ECM estimate at 5% level, but the coefficient of the CS-DL technique is higher, where a 1 unit increase in Quadrillion Btu of Energy will raise GDPGR by 18.6%. This suggests that in the short-run, an increase in energy use causes high economic growth in those countries. The coefficient of CO2 is positively related to GDPGR using CS-ARDL and CS-ECM techniques but negatively related to GDPGR using CS-DL and CS-ECM techniques; however, only the coefficient of the CS-DL technique is significant at the 10% level, where a 1 unit increase in kilotons of CO2 will raise GDPGR by 1.3%. This indicates that, in the short-run, CO2e is related to the increase in economic activities, such that the greater the CO2e, the higher the economic growth of the T20HEE. However, none of the techniques found the coefficient of HEX to be significant, though positively related to GDPGR. This means that in the short-run, the HEX is negligibly aiding countries' economic growth. As indicated by CS-ARDL and validated by CS-ECM methods, the coefficient of ECMt-1 is negative and significant at the 1% level. The significance confirms the earlier cointegration test, which concluded that there is a long-run association between the variables and that, in the event of a shock in the short-run, the model will automatically adjust itself by 120% (1.2) each year, resulting in a speedy convergence to the equilibrium path.
In the long-run, according to the estimates of all the techniques, the coefficient of Energy is negatively related to GDPGR using CS-ARDL and CS-ECM techniques and negatively related to GDPGR when applying CS-DL and AMG techniques; however, only that of the CS-DL is statistically significant at the 5% level, where a 1 unit increase in Quadrillion Btu of energy induces a 34.5% increase in GDPGR. This means that an increase in energy consumption causes rapid economic growth in the countries in both the short and long run. The coefficient of CO2 is positively related to GDPGR by CS-ARDL and CS-ECM techniques but negatively related with GDPGR by CS-DL and AMG techniques; however, only the coefficient of the CS-DL technique is statistically significant at the 10% level, where a 1 unit increase in kilotons of CO2 will decline GDPGR by 17.8%. This means that unlike in the short-run, where it is aiding the economy, in the long-run, the production of CO2e is extremely damaging the economic growth of the T20HEE. However, all the AMG techniques found the impact of HEX to be significant in relation to GDPGR at the 1% level, and the impact is negative, where a 1% increase in HEX will retard GDPGR by 1.4%. This implies that health expenditures have no impact on economic growth in the long-run. In all four techniques, the p-value of the heteroscedasticity test statistic of the estimated technique residuals is insignificant, and this indicates that the residuals are homoscedastic, which shows healthy estimates of the techniques.
Table 10 illustrates the Pairwise Dumitrescu-Hurlin (2012) panel Granger causality test results. According to the findings of the study, we observed that there is a bidirectional causality between HS and CO2, HS and HEX, HS and GDPGR, HS and Energy, HEX and CO2, CO2 and GDP, Energy and CO2, and Energy and HEX, but a unidirectional causality running from Energy to GDPGR. However, there is no causality between HEX and GDPGR. The outcomes of the Granger causality are graphical presented in Fig. 5.

Graphical representation of Granger causality test results
Discussion of the Results
This paper explored the interaction of health status, CO2 emissions, and energy use among the T20HEE. The first model is to achieve the first objective, which is to examine whether health status (HS) is affected by CO2 emissions (CO2) of the T20HEE, where variables – health status, CO2 emissions, health expenditure, and economic growth were used. The results revealed that in the short-run, CO2 emissions are weakening the health status, but in both short- and long-runs, health expenditure improves the health status, while in both the short- and long-runs, economic growth is not contributing to the health status of the countries. This finding is in line with that of Igbinedion (2019) in Nigeria on CO2, Taghizadeh-Hesary et al. (2020) in low- and middle-income Asian countries on CO2, Wang et al. (2020) in China on CO2, Osabohien et al. (2021) in Nigeria on CO2, and Zeeshan et al. (2021) in China on CO2, and environmental pollution shocks increase health expenditure both in the short- and long-runs. Therefore, health status is affected by CO2e of the T20HEE.
The second model is to achieve the second and third objectives, which are to explore whether health expenditure is helping in mitigating CO2 emissions and to assess how energy use is related to their production of CO2 emissions in the T20HEE, where variables – CO2 emissions, energy use, health expenditure, and economic growth were used. The results revealed that in the long-run health expenditure and economic growth are helping to mitigate CO2e, while in both the short and long runs; energy use is increasing CO2e in the selected countries. This is consistent with the findings of Keho (2017) in 59 countries on energy use, Apergis et al. (2018) in sub-Saharan African countries on health expenditure, Gündüz (2020) in the USA on health expenditure, Bilgili et al. (2021) in 36 Asian countries on health expenditure, Ganda (2021) in BRICS countries on health expenditure, Liu et al. (2019) in China, India, and G7 countries on energy use, Ssali et al. (2019) in six sub-Saharan African countries on energy use, Zou and Zhang (2020) in 30 Chinese provinces on energy use, Litavcová and Chovancová (2021) in 14 Danube-area nations on energy use, Salari (2021) in the United States on energy use, and Wu et al. (2022) in the Nordic countries on energy use. However, it is in contrast with the finding of Mensah et al. (2018) in 28 OCED nations on economic growth. Therefore, health expenditure is helping to mitigate CO2e, and energy use is raising the level of CO2e in the selected countries.
The third model is to achieve the fourth objective, which is to examine how energy use and CO2 emissions are related to the economic growth of the T20HEE, where variables for economic growth, energy use, CO2 emissions, and health expenditure were used. The results revealed that both in the short and long runs, energy use contributes to high economic growth in the selected countries, whereas CO2e is aiding economic growth in the short run but extremely damaging it in the long run, while both in the short and long runs, health expenditure is not aiding the economic growth of the countries. This finding is in line with that of Azam et al. (2016) in selected higher CO2 emitting countries on CO2e, Ghorashi and Alavi (2017) in Iran on CO2e, Ummalla (2019) in the BRICS countries on energy use, Wang et al. (2020) in China on CO2e, Radmehr et al. (2021) in the European Union on CO2e, Adebayo (2022) in China on CO2e, and Adebayo et al. (2023d) in BRICS countries on CO2e. Therefore, energy use is influencing the economic growth of the countries, while CO2e is retarding it.
Conclusion and Policy Recommendations
The current study examined the interrelationship of human health status, both public-private health expenditures, CO2 emissions, energy use, and economic growth, which could be pretty interesting in the context of the top-emitting economies from 2000 to 2019. To achieve this goal, we employ advanced techniques of Cross-Sectional Augmented Distributed Lag (CS-DL) and Cross-sectional Augmented Autoregressive Distributed Lag (CS-ARDL), which take into consideration crucial elements of panel data, namely dynamics, heterogeneity, and cross-sectional dependence. The study adopted advanced econometrics analysis of second-generation panel methods such as Pesaran unit root test, Westerlund cointegration test, and the Dumitrescu-Hurlin Granger causality test was employed to determine the causal relationships between the variables. The study also employs the Cross-sectional Augmented Error Correction Method (CS-ECM) and the common dynamic process of the Augmented Mean Group (AMG) for robustness testing. The findings revealed that CO2e weakens the health status only in the short-run, whereas health expenditure improves the health status in the both short- and long-runs, while economic growth is not contributing to the health status in the both short- and long-runs. Furthermore, health expenditure and economic growth only help to mitigate CO2e in the long-run, whereas energy use causes CO2e in the both short- and long-runs. Moreover, energy use causes high economic growth in the both short- and long-runs, whereas CO2e aids economic growth in the short-run but is extremely damaging to economic growth in the long-run, while in the both short- and long-runs health expenditure is not aiding the economic growth. Additionally, the Pairwise Dumitrescu Hurlin Panel Causality Test revealed that a bidirectional causality exists between health status and CO2 emissions, health status and health expenditure, health status and economic growth, health status and energy, health expenditure and CO2 emissions, energy use and CO2 emissions, CO2 emissions and economic growth, and energy use and health expenditure, while a unidirectional causality exists between energy use and economic growth. On the other hand, there is no causal relationship between health expenditures and economic growth.
Therefore, CO2 emissions are harming the health status, health expenditure is tackling the CO2 emissions, energy use is fueling the rate of the CO2 emissions and is stimulating economic growth, while CO2 emissions are retarding economic growth. Hence, the current study offers the following policy recommendations for the T20HEE and global policymakers to improving people’s health and environmental policy framework which will lead to accomplish the SDGs, particularly, SDG-3 and SDG-7, as follows:
First, the governments of the T20HEE should increase both public-private health expenditures by adopting a cost-effective service and energy-efficient health management approach in order to achieve sustainable healthcare services and create a sustainable environment. As a result, the proceeds of economic growth should be prudently channeled by increasing the portion of healthcare expenditure, thus improving health status and addressing the negative effects of CO2e, thereby, creating a healthy society with a green and clean environment for long-term development for the people. In addition, the health and well-being of patients can be improved by helping healthcare workers communicate more effectively. Improving health also necessitates strategies to ensure that medical professionals are aware of suggested services and treatment protocols.
Second, as CO2e has a significant negative impact on health by generating various health-related diseases, such as heart problems, lung problems, and recently, flu related diseases such as COVID-19. In this regard, policymakers should adopt green and clean environment policy to protect the environment quality and minimize the incidence of health diseases. It is also essential to develop and implement suitable environmental laws, particularly in the T20HEE to avoid the adverse impact of environmental pollution on human health.
Third, the governments and policymakers of the top-emitting economies should made additional efforts to promote technical innovation and cleaner production for manufacturing purposes in order to reduce consumption-based CO2e to secure a healthy environment for the people. In addition, the policymakers should be imposed a heavy carbon tax on emissions-intensive products and imported resources for both production and consumption purposes. Because the production process of these top-emitting countries emits high CO2 and resulting serious pollution in the environment. Therefore, policymakers should be implemented strict policy rules that assure the usage of modern environmental-friendly technologies and promote CO2e reduction technologies to improve environment quality. Moreover, governments of these economies should encourage locals to use less energy, recycle, and place a higher value on environmental products and services. It could be helpful to reduce the number of cars on the road and the amount of fossil fuels usage, and to encourage people to use public transportation and bikes instead of their cars.
Fourth, the governments of the top-economies must increase necessary investments in the field of technological innovation, especially in the energy sector, which will enhance energy efficiency infrastructure and boosting the usage of pollutant-free alternative energy sources and increase the supply of green energy. Additionally, public procurement reform can have a significant influence. Governments may reduce their own carbon footprint by using greener goods and services, while also motivating other players to enhance their own sustainable consumption and production habits by establishing strong green contract criteria.
Fifth, the T20HEE could not achieve environmental sustainability if they continue to increase their dependence on fuel energy sources (coal, gas, and petrol) to fulfill their domestic demands in the energy sector. As renewable (clean) energy consumption is essential for reducing CO2e, the governments of these economies should take considerable steps to develop supportive policies which increase the investment in clean energy sources and reduce the reliance on fossil fuel energy. These top-emitting countries consume extensive energy, therefore policymakers should carefully implement energy-saving policies with caution, as changes in energy could obstruct their economic growth rate, and also, they must strike a balance between energy production and economic growth. The industries which contribute to fuels energy sources should develop alternative energy such as clean energy sources in the manufacturing and transportation processes for sustainable economic growth. Therefore, policymakers should facilitate industries and organizations to promote green energy technologies and increase the investment in clean energy sources in order to achieve the SDGs-7.
Finally, subsidies and tax breaks are further strategies to increase the demand for eco-friendly goods and services, including electric vehicles, solar energy, and renewable energy. To encourage innovation and the development of game-changing technologies like renewable energy, carbon capture, waste management, and energy efficiency, governments must provide subsidies and grant funding to research organizations, academic institutions, and private R&D enterprises.
However, the current study has some limitations that should be addressed in future research studies. The large amount of the world population and high level of development and production of the top-emitting economies, the findings of this study may not be applicable to less emitting or other group of countries. However, further studies could conduct similar research on less developed economies or countries with less than one percent of the total world emission and examine the nexus among health status, CO2 emissions, and energy use across the economies. Nonetheless, such study could be conducted among the top industrial economies as well as among the energy transition economies. Furthermore, since CO2e are major contributor of environmental pollution, it is important to consider the negative impact of other GHGs emissions on human health, such as methane (CH4), nitrous oxide (N2O), and sulfur dioxide (SO2). Moreover, potential limitations of this study could not be extended to the current time period due to the unavailability of relevant data. Lastly, this study explores the relationship between health status, CO2e, and energy use in the T20HEE. Further studies can not only investigate this relationship in other economies but also need to include other important economic variables, such as financial development, technological innovation, globalization, etc.
Data availability
The datasets of this study are available upon request.
Notes
The Intergovernmental Panel on Climate Change (IPCC) is the United Nations body for assessing the science related to climate change. See: Reports, Global Warming of 1.5 °C, October, 2018. https://www.ipcc.ch/sr15/
T20HEE: “China, the United States, India, Russia, Japan, Iran, Germany, Indonesia, the Republic of Korea, Saudi Arabia, Canada, South Africa, Brazil, Mexico, Australia, Turkey, the United Kingdom, Italy, France, and Poland”.
Glasgow Climate Pact. https://ukcop26.org/.
Sharm El-Sheikh Climate Pact. https://japan-forward.com/cop27-summit-kicks-off-in-egypt-to-tackle-existential-climate-crisis/amp/?
Abbreviations
- CO2e:
-
Carbon Dioxide Emissions
- T20HEE:
-
Top 20 Highest Emitting Economies
- CS-DL:
-
Cross-Sectional Augmented Distributed Lag Model
- CS-ARDL:
-
Cross-Sectional Augmented Autoregressive Distributed Lag Model
- CS-ECM:
-
Cross-Sectional Augmented Error Correction Method
- AMG:
-
Augmented Mean Group
- SDGS:
-
Sustainable Development Goals
- IPCC:
-
Intergovernmental Panel on Climate Change
- COP:
-
Climate Change Conference
- PPP:
-
Purchasing Power Parity
- GDP:
-
Gross Domestic Product
- IEA:
-
International Energy Agency
- EKC:
-
Environmental Kuznets Curve
- RE:
-
Renewable Energy
- EU:
-
European Union
- SAARC:
-
South Asian Association for Regional Cooperation
- MINT:
-
Mexico, Indonesia, Nigeria, And Turkey
- ECOWAS:
-
Economic Community of West African States
- OECD:
-
Organization for Economic Cooperation and Development
- E7:
-
China, India, Brazil, Mexico, Russia, Indonesia, and Turkey
- FMOLS:
-
Fully Modified Ordinary Least Squares
- VECM:
-
Vector Error Correction Model
- NARDL:
-
Nonlinear Autoregressive Distributed Lag
- PQR:
-
Panel Quantile Regression
- BRICS:
-
Brazil, Russia, India, China, and South Africa
- ANN:
-
Artificial Neutral Networks
- SDM:
-
Spatial Durbin Model
- CCM:
-
Convergent Cross Mapping
- ECI:
-
Economic Complexity Index
- CCR:
-
Canonical Cointegration Regression
- DOLS:
-
Dynamic Ordinary Least Squares
- CD:
-
Cross-Sectional Dependence
- CIPS:
-
Cross-Sectional Augmented Pesaran and Shin
- GMM:
-
Generalized Method of Moment
References
Adebayo TS, Akinsola GD (2021) Investigating the causal linkage among economic growth, energy consumption and CO2 emissions in Thailand: An application of the wavelet coherence approach. IJRED 10(1):17–26
Adebayo TS, Kirikkaleli D (2021) Impact of renewable energy consumption, globalization, and technological innovation on environmental degradation in Japan: application of wavelet tools. Environ Dev Sustain 23(11):16057–16082
Adebayo TS (2022) Trade-off between environmental sustainability and economic growth through coal consumption and natural resources exploitation in China: new policy insights from wavelet local multiple correlation. Geol J. https://doi.org/10.1002/gj.4664
Adebayo TS, Ullah S, Kartal MT, Ali K, Pata UK, Aga M (2023a) Endorsing sustainable development in BRICS: The role of technological innovation, renewable energy consumption, and natural resources in limiting carbon emission. Sci Total Environ 859(1):160181. https://doi.org/10.1016/j.scitotenv.2022.160181
Adebayo TS, Kartal MT, Aga M, Al-Faryan MAS (2023b) Role of country risks and renewable energy consumption on environmental quality: Evidence from MINT countries. J Environ Manage 327:116884. https://doi.org/10.1016/j.jenvman.2022.116884
Adebayo TS, Kartal MT, Ullah S (2023c) Role of hydroelectricity and natural gas consumption on environmental sustainability in the United States: Evidence from novel time-frequency approaches. J Environ Manage 328:116987. https://doi.org/10.1016/j.jenvman.2022.116987
Adebayo TS, Ağa M, Kartal MT (2023d) Analyzing the co-movement between CO2 emissions and disaggregated nonrenewable and renewable energy consumption in BRICS: evidence through the lens of wavelet coherence. Environ Sci Pollut Res:1–18. https://doi.org/10.1007/s11356-022-24707-w
Adedoyina FF, Agboola FO, Ozturk I, Bekun FV, Agboolag MO (2021) Environmental consequences of economic complexities in the EU amidst a booming tourism industry: Accounting for the role of brexit and other crisis events. J Clean Prod 305:127117. https://doi.org/10.1016/j.jclepro.2021.127117
Adeneye YB, Jaaffar AH, Ooi CA, Ooi SK (2021) Nexus between Carbon Emissions, Energy Consumption, Urbanization and Economic Growth in Asia: Evidence From Common Correlated Effects Mean Group Estimator (CCEMG). Front Energy Res 18:1–15. https://doi.org/10.3389/fenrg.2020.610577
Ahmad M, Akram W, Ikram M, Ahmad A et al (2020) Estimating dynamic interactive linkages among urban agglomeration, economic performance, carbon emissions, and health expenditures across developmental disparities. Sustain Prod Consum 26:239–255. https://doi.org/10.1016/j.spc.2020.10.006
Ahmad M, Rehman A, Shah SAA, Solangi YA, Chandio AA, Jabeen G (2021) Stylized heterogeneous dynamic links among healthcare expenditures, land urbanization, and CO2 emissions across economic development levels. Sci Total Environ 753(2021):142228. https://doi.org/10.1016/j.scitotenv.2020.142228
Alimi OY, Ajide KB, Isola WA (2019) Environmental quality and health expenditure in ECOWAS. Environ Dev Sustain 22(6):5105–5127
Apergis N, Jebli MB, Youssef SB (2018) Does renewable energy consumption and health expenditures decrease carbon dioxide emissions? Evidence for sub-Saharan Africa countries. Renew Energ 127:1011–1016
Apergis N, Bhattacharya M, Hadhri W (2020) Health care expenditure and environmental pollution: a cross-country comparison across different income groups. Environ Sci Pollut Res 27(8):8142–8156
Ashin NMK, Muhammed AV (2020). Role of energy use in the prediction of CO2 emissions and economic growth in India: evidence from artificial neural networks (ANN). Environ Sci Pollut Res 27:23631–23642. https://doi.org/10.1007/s11356-020-08675-7
Azam M, Khan AQ, Abdullah HB et al (2016) The impact of CO2e on economic growth: evidence from selected higher CO2 emissions economies. Environ Sci Pollut Res 23:6376–6389. https://doi.org/10.1007/s11356-015-5817-4
Balan F (2016) Environmental quality and its human health effects: a causal analysis for the EU-25. Int J Appl Econ 13(1):57–71
Bekun FV (2022) Mitigating Emissions in India: Accounting for the Role of Real Income, Renewable Energy Consumption and Investment in Energy. Int J Energy Econ Policy 12(1):188–192. https://doi.org/10.32479/ijeep.12652
Bekun FV, Adedoyin FF, Etokakpan MU, Gyamfi BA (2021a) Exploring the tourism-CO2 emissions-real income nexus in E7 countries: accounting for the role of institutional quality. J Policy Res Tour Leis Events 14(1):1–19. https://doi.org/10.1080/19407963.2021.2017725
Bekun FV, Gyamfic BA, Onifadedef ST, Agboolag MO (2021b) Beyond the environmental Kuznets Curve in E7 economies: Accounting for the combined impacts of institutional quality and renewables. J Clean Prod 314(10):127924. https://doi.org/10.1016/j.jclepro.2021.127924
Bhujabal P, Sethi N, Padhan PC (2021) ICT, foreign direct investment and environmental pollution in major Asia Pacific countries. Environ Sci Pollut Res 7(1):1–11. https://doi.org/10.1007/s11356-021-13619-w
Bilgili F, Kuşkaya S, Khan M et al (2021) The roles of economic growth and health expenditure on CO2 emissions in selected Asian countries: a quantile regression model approach. Environ Sci Pollut Res 28:44949–44972. https://doi.org/10.1007/s11356-021-13639-6
Blázquez-Fernández C, Cantarero-Prieto D, MartaPascual-Sáez. (2019) On the nexus of air pollution and health expenditures: new empirical evidenceRelación entre la contaminación atmosférica y los gastos sanitarios: nueva evidencia empírica. Gac Sanit 33(4):389–394
Caglar AE, Zafar MW, Bekun FV, Mert M (2021) Determinants of CO2 emissions in the BRICS economies: The role of partnerships investment in energy and economic complexity. Sustain Energy Technol Assess 51:101907. https://doi.org/10.1016/j.seta.2021.101907
Cai Y, Sam CY, Chang T (2018) Nexus between clean energy consumption, economic growth and CO2 emissions. J Clean Prod 182:1001–1011. https://doi.org/10.1016/j.jclepro.2018.02.035
Callan T, Lyons S, Scott S, Tol RSJ, Verde S (2009) The distributional implications of a carbon tax in Ireland. Energy Policy 37(2):407–412. https://doi.org/10.1016/j.enpol.2008.08.034
Chakraborty, S.K. and Mazzanti, M. (2021). Renewable Electricity and Economic Growth relationship in the long run: panel data econometric evidence from the OECD. SEEDS Working Paper Series 04/2021.
Chen H, Zhang X, Wu R, Cai T (2020) Revisiting the environmental Kuznets curve for city-level CO2 emissions: based on corrected NPP-VIIRS nighttime light data in China. J Clean Prod 268:121575. https://doi.org/10.1016/j.jclepro.2020.121575
Chudik A, Pesaran MH (2015) Common correlated effects estimation of heterogeneous dynamic panel data models with weakly exogenous regressors. J Econom 188:393–420. https://doi.org/10.1016/j.jeconom.2015.03.007
Chudik A, Pesaran MH, Tosetti E (2011) Weak and strong cross-section dependence and estimation of large panels. J Econom 14(1):C45–C90
Chudik A, Kamiar M, Hashem Pesaran M, Raissi M (2016) Long-run effects in large heterogeneous panel data models with cross-sectionally correlated errors. In: Gloria Gonzlez-Rivera R, Hill C, Lee T-H (eds) Advances in Econometrics, vol 36. Emerald Group Publishing Limited, pp 85–135
Chudik A, Mohaddes K, Pesaran MH, Raissi M (2017) Is there a debt-threshold effect on output growth? Rev Econ Stat 99(1):135–150
Clark G, Hammond P (2019) Green finance strategy: Transforming finance for a greener future. Green Finance Institute Retrieved on 12th November 2019, from: https://www.gov.uk/government/publications/green-finance-strategy. Accessed 10 Jul 2022
Destek MA, Sinha A (2020) Renewable, non-renewable energy consumption, economic growth, trade openness and ecological footprint: evidence from organization for economic Cooperation and development countries. J Clean Prod 242:118537. https://doi.org/10.1016/j.jclepro.2019.118537
Diffenbaugh NS (2020) Verification of extreme event attribution using out-of-sample observations to assess changes in probabilities of unprecedented events. Sci Adv 6(12):eaay2368
Dumitrescu EI, Hurlin C (2012) Testing for Granger non-causality in heterogeneous panels. Econ Model 29:1450–1460. https://doi.org/10.1016/j.econmod.2012.02.014
Eberhardt M, Teal F (2010) Productivity analysis in global manufacturing production. DEGIT, Dynamics, Economic Growth, and International Trade
Eberhardt, M. and Vollrath, D. (2016). ‘The effect of agricultural technology on the speed of development’, forthcoming in world development.
Eberhardt M, Helmers C, Strauss H (2013) Do spillovers matter when estimating private returns to RandD? Rev Econ Stat 95:436–448
Erdoğan S, Pata UK, Solarin SA, Okumus I (2022) On the persistence of shocks to global CO2 emissions: a historical data perspective (0 to 2014). Environ. Sci. Pollut Control Ser 29:77311–77320
Gallo Cassarino T, Sharp E, Barrett M (2018) The impact of social and weather drivers on the historical electricity demand in Europe. Appl Energy 229:176–185. https://doi.org/10.1016/j.apenergy.2018.07.108
Ganda F (2021) The impact of health expenditure on environmental quality: the case of BRICS. Dev Stud Res 8(1):199–217. https://doi.org/10.1080/21665095.2021.1955720
Gavurova B, Rigelsky M, Ivankova V (2021) Greenhouse Gas Emissions and Health in the Countries of the European Union. Front Public Health 9
Ghorashi N, Alavi RA (2017) CO2e, Health expenditures and economic growth in Iran: Application of dynamic simultaneous equation models. J Community Health Res 6(2):109–116
Grossman GM, Krueger AB (1995) Economic growth and the environment. Q J Econ 110(2):353–377. https://doi.org/10.2307/2118443
Gündüz M (2020) Healthcare expenditure and carbon footprint in the USA: evidence from hidden cointegration approach. Eur J Health Econ 21(5):801–811
Holly S, Pesaran MH, Yamagata T (2010) A spatial-temporal model of house prices in the USA. J Econom 158:160–173
IEA (2017). CO2 emissions from fuel combustion. Retrieved August 10, 2020, from International Energy Agency website: http://www.iea.org/publications/freepublications/publication/CO2-emissions fromfuelcombustion-highlights-2017.html. Accessed 15 Jul 2022
Igbinedion SO (2019) Environmental emissions and life expectancy Nexus: Further Evidence from Nigeria. Ann Univ Petroşani, Economics 19(1):115–128
IPCC (2021) Climate change 2021: The physical science basis: working group I contribution to the sixth assessment report of the intergovernmental panel on climate change. Available at https://www.unep.org/resources/report/climate-change-2021-physical-sciencebasisworking-group-i-contribution-sixth. Accessed 15 Jul 2022
Irfan M, Ullah S, Razzaq A, Cai J, Adebayo TS (2023) Unleashing the dynamic impact of tourism industry on energy consumption, economic output, and environmental quality in China: A way forward towards environmental sustainability. J Clean Prod 387:135778. https://doi.org/10.1016/j.jclepro.2022.135778
Jacobo C, Viviana S (2013) The relationship between energy consumption and GDP: Evidence From a Panel Of 10 Latin American Countries. Lat Am J Econ 50(2):233–255
Kayani GM, Ashfaq S, Siddique A (2020) Assessment of financial development on environmental effect: implications for sustainable development. J Clean Prod 261:120984. https://doi.org/10.1016/j.jclepro.2020.120984
Keho Y (2017) Revisiting the Income, Energy Consumption and Carbon Emissions Nexus: New Evidence from Quantile Regression for Different Country Groups. Int J Energy Econ. Policy 7(3):1–13
Khan A, Hussain J, Bano S, Chenggang Y (2020) The repercussions of foreign direct investment, renewable energy and health expenditure on environmental decay? An econometric analysis of B&RI countries. J Environ Plan Manag 63(11):1965–1986
Kirikkaleli D, Güngör H, Adebayo TS (2022) Consumption-based carbon emissions, renewable energy consumption, financial development and economic growth in Chile. Bus Strategy Environ 31(3):1123–1137
Kreft S, Eckstein D, Dorsch L, Fischer L (2016) Global climate risk index 2016: who suffers most from extreme weather events? weather-related loss events in 2014 and 1995 to 2014. Global climate risk index.
Kuznets S (1955) Economic growth and income inequality. Am Econ Rev 45(1):1–28
Li F, Chang T, Wang MC, Zhou J (2022) The relationship between health expenditure, CO2 emissions, and economic growth in the BRICS countries—based on the Fourier ARDL model. Environ Sci Pollut Res:1–20
Litavcová E, Chovancová J (2021) Economic Development, CO2 emissions and Energy Use Nexus-Evidence from the Danube Region Countries. Energies 2021(14):3165. https://doi.org/10.3390/en14113165
Liu H, Lei M, Zhang N, Du G (2019) The causal nexus between energy consumption, carbon emissions and economic growth: New evidence from China, India and G7 countries using convergent cross mapping. PLoS ONE 14(5):e0217319. https://doi.org/10.1371/journal
McKinnon M (2012) Climate vulnerability monitor: A guide to the cold calculus of a hot planet. Estudios Gráfcos Europeos, SA, Spain, p 331
Mensah CN, Long X, Boamah KB et al (2018) The effect of innovation on CO2 emissions of OCED countries from 1990 to 2014. Environ Sci Pollut Res 25:29678–29698. https://doi.org/10.1007/s11356-018-2968-0
Mott G, Razo C, Hamwey R (2021) Carbon emissions anywhere threaten development everywhere. https://unctad.org/news/carbon-emissions-anywhere-threaten-development-everywhere. Accessed 15 Jul 2022
Munir K, Riaz N (2019) Energy consumption and environmental quality in South Asia: evidence from panel non-linear ARDL. Environ Sci Pollut Res. https://doi.org/10.1007/s11356-019-06116-8
Murshed M, Ahmed Z, Alam MS et al (2021) Reinvigorating the role of clean energy transition for achieving a low-carbon economy: evidence from Bangladesh. Environ Sci Pollut Res:1–22
Muntean M, Guizzardi D, Schaaf E, Crippa M, Solazzo E, Olivier J, Vignati E (2018) Fossil CO2 emissions of all world countries. Publications Office of the European Union, Luxembourg, p 2
NASA (2020) Global climate change. Retrieved from https://climate.nasa.gov. Accessed 17 Jul 2022
Osabohien R, Aderemi TA, Akindele DB, Jolayemi LB (2021) Carbon Emissions and Life Expectancy in Nigeria. Int J Energy Econ Policy 11(1):497–501
Pao HT, Chen CC (2019) Decoupling strategies: CO2 emissions, energy resources, and economic growth in the Group of Twenty. J Clean Prod 206:907–919. https://doi.org/10.1016/j.jclepro.2018.09.190
Pesaran MH (2004) General diagnostic tests for cross-section dependence in panels. IZA Discussion Paper.:1240
Pesaran MH (2006) Estimation and Inference in Large Heterogeneous Panels with a Multifactor Error Structure. Econometrica 74(4):967–1012
Pesaran M (2007) A simple panel unit root test in the presence of cross-section dependence. J Appl Econom 22(2):265–312
Pesaran MH (2015) Time series and panel data econometrics. First edition. Oxford, United Kingdom: Oxford University Press
Radmehr R, Henneberry SR, Shayanmehr S (2021) Renewable Energy Consumption, CO2 emissions, and Economic Growth Nexus: A Simultaneity Spatial Modeling Analysis of EU Countries. Structural Change and Economic Dynamics 57:13–27
Rahman MM, Alam K (2021) The nexus between health status and health expenditure, energy consumption and environmental pollution: empirical evidence from SAARC-BIMSTEC regions. BMC Public Health 21(1694):1–12. https://doi.org/10.1186/s12889-021-11534-w
Salari M, Javid RJ, Noghanibehambari H (2021) Energy The nexus between CO2 emissions, energy consumption, and economic growth in the U.S. Econ Anal Policy 69:182–194
Sharif A, Baris-Tuzemen O, Uzuner G et al (2020) Revisiting the role of renewable and non-renewable energy consumption on Turkey’s ecological footprint: evidence from Quantile ARDL approach. Sustain Cities Soc 57:102138. https://doi.org/10.1016/j.scs.2020.102138
Sinha A, Gupta M, Shahbaz M, Sengupta T (2019) Impact of corruption in public sector on environmental quality: Implicationsfor sustainability in BRICS and next 11 countries. J Clean Prod 232:1379–1393. https://doi.org/10.1016/j.jclepro.2019.06.066
Ssali MW, Du J, Mensah IA, Hongo DO (2019) Investigating the nexus among environmental pollution, economic growth, energy use, and foreign direct investment in 6 selected sub-Saharan African countries. Environ Sci Pollut Res 26:11245–11260. https://doi.org/10.1007/s11356-019-04455-0
Taghizadeh-Hesary F, Rasoulinezhad E, Yoshino N, Chang Y, Taghizadeh-Hesary F, Morgan PJ (2020) The energy–pollution–health nexus: A panel data analysis of low- and middle-income asian nations. In: ADBI Working Paper 1086. Asian Development Bank Institute, Tokyo https://www.adb.org/publications/energy-pollution-health-nexus-asian-nations. Accessed 12 Jul 2022
U.S. Energy Information Administration-international energy statistics database (2020) statistical bulletin. https://www.eia.gov/international/data/world. Accessed 11 Jul 2022
UN (2015) Sustainable development goals. General assembly. Retrieved from: https://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E. Accessed 15 Jul 2022
Ulucak R, Bilgili F (2018) A reinvestigation of EKC model by ecological footprint measurement for high-, middle- and low-income countries. J Clean Prod 188:144–157. https://doi.org/10.1016/j.jclepro.2018.03.191
Ummalla M, Samal A, Goyari P (2019) Nexus among the hydropower energy consumption, economic growth, and CO2 emissions: evidence from BRICS countries. Environ Sci Pollut Res 26:35010–35022. https://doi.org/10.1007/s11356-019-06638-1
Verma P, Kumari T, Raghubanshi. (2021) Energy emissions, consumption and impact of urban households: A review. Elsevier https://www.sciencedirect.com/science/article/pii/S1364032121004986. Accessed 10 Jul 2022
Vohra K, Vodonos A, Schwartz J, Marais EA, Sulprizio MP, Mickley LJ (2021) Global mortality from outdoor fine particle pollution generated by fossil fuel combustion: Results from GEOS-Chem. Environ Res 195:110754. https://doi.org/10.1016/j.envres.2021.110754
Wahab S, Zhang X, Safi A, Wahab Z, Amin M (2021) Does Energy Productivity and Technological Innovation Limit Trade-Adjusted Carbon Emissions? Econ Res-Ekon Istraz 34(1):1896–1912. https://doi.org/10.1080/1331677X.2020.1860111
Wang J, Ma F, Bouri E, Zhong J (2022) Volatility of clean energy and natural gas, uncertainty indices, and global economic conditions. Energy Economics 108:105904
Wang C, Chang C, Yuan C, Wang J, Feng Y (2020) Examine the relationship between China’s health expenditure and CO2 emissions taking into account economic growth. IOP Conf Ser: Earth Environ Sci 555 12020. https://doi.org/10.1088/1755-1315/555/1/012020
WHO (2018) Accelerating SDG 7 achievement-policy brief # 10: health and energy linkages maximizing health benefits from the sustainable energy transition: World Health Organization. Available at: https://sustainabledevelopment.un.org/content/documents/17486PB10.pdf. Accessed 17 Jul 2022
World Health Statistics (2019). Monitoring health for the sustainable development goals (SDGs). https://apps.who.int/iris/bitstream/handle/10665/324835/9789241565707-eng.pdf. Accessed 20 Jul 2022
World Health Organization (2011) Health in the green economy: co-benefits to health of climate change mitigation: Household energy sector in developing countries. http://www.who.int/hia/green_economy/en/. Accessed 20 Jul 2022
World Health Organization (2015) Residential heating with wood and coal: health impacts and policy options in Europe and North America. https://apps.who.int/iris/handle/10665/153671
World Health Organization (2019) Household air pollution and health, fact sheet number 292. Retrieved from http://www.who.int/mediacentre/factsheets/fs292/en/. Accessed 7 Jul 2022
World Bank (2020) World Development Indicators online statistical bulletin. https://data.worldbank.org/. Accessed 7 Jul 2022
Wu L, Adebayo TS, Yue X, Umutd A (2022) The role of renewable energy consumption and financial development in environmental sustainability: implications for the Nordic Countries. Int J Sustain Dev World Ecol 30(1):21–36. https://doi.org/10.1080/13504509.2022.2115577
Yang T, Liu W (2018) Does air pollution affect public health and health inequality? Empirical evidence from China. J Clean Prod 203:43–52
Zeeshan M, Han J, Rehman A, Ullah I, Afridi FEA (2021) Exploring Asymmetric Nexus between CO2 emissions, Environmental Pollution, and Household Health Expenditure in China. Risk Manag Health Policy. 14:527–539. https://doi.org/10.2147/RMHP.S281729
Zou S, Zhang T (2020) CO2 emissions, Energy Consumption, and Economic Growth Nexus: Evidence from 30 Provinces in China. Math Probl Eng 2020:8842770, 10 pages, 2020. https://doi.org/10.1155/2020/8842770
Westerlund J (2007) Testing for error correction in panel data. Oxf Bull Econ Stat 69(6):709–748
Funding
This research is supported by The National Key R&D Program of China (2017YFE0119200)
Author information
Authors and Affiliations
Contributions
Ali Sohail: Conceptualization, Formal Analysis, Methodology, Software, Data Curation, Writing-Original Draft preparation. Jinfeng Du: Formal Analysis, Supervision, Investigation, Visualization. Babar Nawaz Abbasi: Writing - Review and Editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sohail, A., Du, J. & Abbasi, B.N. Exploring the interrelationship among health status, CO2 emissions, and energy use in the top 20 highest emitting economies: based on the CS-DL and CS-ARDL approaches. Air Qual Atmos Health 16, 1419–1442 (2023). https://doi.org/10.1007/s11869-023-01350-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11869-023-01350-z
Keywords
- Health status
- Carbon emissions
- Energy use
- Economic growth
- CS-DL model
- CS-ARDL model
- Top 20 highest emitting economies