
Abstract
In recent times, the literature has seen considerable growth in research at the intersection of CO2 emission, health expenditure, and economic growth. But looking at the literature, it appears that the relationship between health expenditures, CO2 emissions, and economic growth is unclear. To resolve this uncertainty, this study was conducted with different data, countries, and methods. To this end, the present study analyzed the nexus between CO2 emissions, health expenditure, and economic growth in Türkiye from 1975 to 2020 using the Autoregressive Distributed Lagged (ARDL) model developed by Pesaran et al. (J Appl Econ 16(3):289–326, 2001). The study reveals a connection between CO2 emissions, health spending, and economic development in Türkiye over the long term. It also highlights a short-term correlation among these factors. The study indicates that a 1% increase in economic growth results in a 0.553 and 0.297 rise in CO2 emissions in the short and long term, respectively. That is, it suggests that if economic growth in Türkiye doesn’t involve renewable energy, it could negatively affect CO2 emissions both in the short and long term. To address this, substantial efforts are needed to transition to low-carbon technologies like renewable energy and energy efficiency, aiming to reduce emissions and support long-term economic growth. The study further demonstrates that a 1% growth in health expenditure leads to a 0.124% decrease in CO2 emissions over the long term. This implies that Türkiye’s health sector could benefit from utilizing more renewable energy or using fossil fuels more efficiently. Additionally, the study warns that long-term population growth could negatively affect CO2 emissions in Türkiye.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
In recent years, increasing greenhouse gases have become a global environmental problem that threatens people’s ability to breathe freely (Mehmood et al., 2022). Increased greenhouse gas emissions influence precipitation and temperature elevation due to global climate change. Unavoidable climate change poses a grave threat to the long-run survival of people, society, the economy, and the environment (Muntean et al., 2018). The effects of climate change, high greenhouse gas concentrations, and public health effects of global warming are all significantly correlated (Wang et al., 2019a). Respiratory illnesses are caused by air pollutants like CO2 and SO2. Therefore, the public’s health suffers as air pollution levels rise (Kayani et al., 2020; Li et al., 2019; Mujtaba & Shahzad, 2021). Burning fossil fuels and deforestation are two examples of human actions that produce CO2, a greenhouse gas, into the atmosphere. A rising body of research indicates a connection between healthcare spending and carbon emissions, despite the fact that the two may not initially appear to be connected. For instance, the manufacture and delivery of medical supplies and medications, as well as the energy requirements of hospitals and other healthcare institutions, all contribute to the emission of CO2. In addition, the growing need for healthcare services, which is being fueled in part by aging populations, might result in increased healthcare costs and, consequently, higher carbon emissions. On the other hand, as a result of the emission of several different air toxins into the atmosphere, increased economic growth, urbanization, and industrialization in both industrialized and developing countries have significantly worsened air quality. Besides, it is known that the deterioration in environmental conditions is associated with economic growth, and worsening in environmental conditions causes heart diseases, cancer, and respiratory diseases. The connection between environmental factors, population health, ecological conservation, public policy, and the price of healthcare services is becoming increasingly significant. While environmental pollution harms human health, it also negatively affects labor productivity (Dağ & Kızılkaya, 2021).
It has only lately come up for consideration how health, air quality, and economic growth are related. This literature may be divided into three research areas (Zaidi & Saidi, 2018). The first line concentrated on the connection between environmental preservation and economic expansion, a subject of several studies since 1960. Despite different findings from research on the relationship between the environment and economic growth, there is a widespread understanding that economic growth leads to environmental deterioration (Arouri et al., 2012; Dinda, 2004; Iwata et al., 2010; Jalil & Mahmud, 2009; Liu et al., 2019; Lotfalipour et al., 2010; Marrero, 2010; Mujtaba & Jena, 2021; Musibau et al., 2021; Pao & Tsai, 2010; Soytas et al., 2007; Wang et al., 2011). It has been discovered that CO2 emissions and economic development have a complicated connection. Economic activity frequently results in higher energy consumption and industrial production; hence CO2 emissions have generally been linked to economic expansion. According to some studies, when countries advance and become wealthy, they may also increase their investments in clean energy and energy efficiency, which can reduce emissions.
The relationship between environment and health expenditure is the subject of the second line (Burnett et al., 1998). Air pollution from carbon dioxide (CO2), nitrogen oxides (NOX), sulfur dioxide (SO2), and methane (CH4) is blamed for environmental damage. Health and environmental issues have recently been discussed (Zaidi & Saidi, 2018). Research on the relationship between health and the environment is necessary due to the increase in infectious diseases brought on by air pollution and high temperatures (Béral-Guyonnet, 1996). Many ecosystems and the creatures that inhabit them are affected by climate change, but it also has an effect on human health.
The third line indicates how health and economic growth are related (Akram et al., 2008; Baltagi & Moscone, 2010; Bloom & Canning, 2003a, 2003b; Erçelik, 2018; Gerdtham & Löthgren, 2002; Lucian, et al., 2009; Murthy & Okunade, 2016; Rivera & Currais, 2003; Wang, 2011). Health is one of the most crucial components of human capital. People are more motivated and productive when they are in good physical and mental health, which helps with both their academic and professional lives. Because of this, this condition can help countries’ economies flourish by improving the effectiveness of their people resources.
The literature, continuous economic growth and increases in health expenditures are linked to CO2 emissions, but this relationship is complex and uncertain. To clarify this complex and uncertain relationship, this study is addressed with different data, countries, and methods. Therefore, the motivation of the current study is to contribute to the literature by observing the impact of health expenditure and economic growth on CO2 emissions through the autoregressive-distributed lag (ARDL) test in Türkiye for the period 1975–2020. The major contribution of our research to the field is to be useful to decision makers in other developing countries, especially Türkiye, and to provide important information on reducing CO2 emissions for developing countries such as Türkiye.
The paper is divided into five sections. An overview of the literature is given in Sect. 2. In Sect. 3, the data and techniques are explained. The results and comments are presented in Sect. 4, and the research is concluded in Sect. 5.
2 Literature review
The purpose of this study is to demonstrate the potential connection, if exists, between GDP growth, CO2 emissions, and health expenditures in Türkiye. We’ll focus on the pairwise correlation variables between the key researches. The literature review is organized into three sections: literature on CO2 emissions and GDP growth, literature on CO2 emissions and health expenditure, and literature on health expenditure and GDP growth.
2.1 The nexus between CO2 emissions and economic growth
In recent decades, there has been a lot of discussion over the relationship between economic growth and CO2 emissions. The Environmental Kuznets Curve (EKC) theory is investigated using several sorts of econometric techniques for various economies (Cai et al., 2018). Income and environmental pollution appear to have an inverted U-shape connection. Numerous investigations back up the EKC concept. The initial empirical analysis was based on Grossman and Krueger’s work, and many scholars have examined the Environmental Kuznets Curve (EKC), which connects economic development to environmental quality. Gökmenoğlu and Taspinar (2016) examined the presence of the environmental Kuznets curve (EKC) hypothesis in Türkiye for the period 1974–2010 using carbon dioxide emissions and GDP growth with ARLD bound test and Toda-Yamamo causality. They find evidence for the EKC theory for CO2 emissions in Türkiye. Similar to this, Apergis and Payne (2010) found that during the years 1992 to 2004, the panel vector error correction model demonstrated that the EKC hypothesis was true when looking at the relationship between CO2 and GDP for eleven countries. Along the same lines, Ahmed and Long (2012), Kanjilal and Ghosh (2013), Bouznit and Pablo-Romero (2016), Shahbaz et al. (2013), Pata (2018), Suki et al. (2020), and He and Lin (2019) each discovered the presence of EKC. On the contrary, several researchers, such as Richmond and Kaufmann (2006), Begum et al. (2015), Pontarollo and Muñoz (2020), Mikayilov et al. (2018), Zhou et al. (2019), Robalino-López et al. (2015) did not find the presence of EKC hypothesis.
2.2 The nexus between CO2 emissions and health expenditure
The second part focuses on CO2 emission and health expenditures. Less research has been done on the connection between CO2 emissions and health expenditures (Wang et al., 2019a). CO2 emissions are regarded as a significant factor in the environmental issue, of their increased detrimental effects on public health. Using the ARDL bound test, Khoshnevis Yazdi and Khanalizadeh (2017) examine how environmental quality (CO2 and PM10) affects health expenditures in the Middle East and North Africa (MENA) area countries during the years 1995 to 2014. They demonstrate that a co-integrated panel of health expenditure, CO2 emissions, and PM10 emissions exists. Long-run elasticities indicate that CO2 and PM10 emissions have statistically significant positive impacts on health expenditures. Using the panel co-integration approach, When Narayan and Narayan (2008) investigated how environmental quality affected per capita health spending, they found that carbon monoxide emissions had a favorable impact on it in the short run. Long-run results demonstrate that sulfur oxide emissions, together with carbon monoxide emissions, have a statistically significant positive impact on healthcare expenditures. Similarly, Ullah et al. (2020), Wang et al. (2019b), and Blázquez-Fernández et al. (2019) found a positive effect of CO2 on health expenditures. On the contrary, Boachie et al. (2014) find that health expenditure and CO2 emissions in Ghana between 1970 and 2008 have a negative association. While investigating the impact of CO2 and health expenditures, results discovered by Zaidi and Saidi (2018) indicate that increased CO2 emissions negatively affect health expenditures in long run. Additionally, Bilgili et al. (2021) investigated the relationship between environmental pollution, economic growth, and public and private healthcare spending in 36 Asian countries. Spending on both private and public health can lower CO2 emissions, according to the quantile regression results for the panel data. According to the study, improved environmental quality in Asian countries is a direct result of increased spending on healthcare services.
2.3 The nexus between health expenditure and GDP growth
The third part contains studies that look at the connection between GDP growth and health expenditures. The empirical study’s third pairing shows that a variety of research techniques have been employed to look at the connection between GDP growth and health spending. Previous economists concentrated on methods for estimating healthcare demand and distributing resources according to income elasticity (Apergis et al., 2018; Wang et al., 2019a).
Wang et al. (2019a) evaluated the relationship between health expenditure and GDP using data from 1975 to 2017 using the ARDL technique and Granger causality application. They found a bidirectional causation for GDP growth in Germany and the United States. Similar research by Nasiru and Usman (2012) and Mehmood et al. (2014) shows a two-way association between health expenditures and economic growth. Using dynamic simultaneous equation models, Ghorashi and Rad (2017)looked at the correlation between health spending and GDP growth in Iran from 1972 to 2012. They found a one-way causal relationship between GDP growth and health spending. Using data from 1995 to 2005 for a sample of 13 MEAN countries, Mehrara et al. (2012) evaluated the stationarity and co-integration between health spending and GDP. They found that the unit root tests indicate that the two variables are not stationary. Despite this, the findings indicate a connection between GDP and health spending. They found that the proportion of health spending to GDP decreases as GDP rises. This suggests that healthcare is essential in MEAN countries. In a similar vein, Baltagi and Moscone (2010) investigated the relationship between health expenditure and GDP growth in a sample of 20 OECD countries. Because of the low coefficient of elasticity involved, the study’s findings, which covered the years 1971–2004, show that spending on health is more of a need than a luxury. According to Wang (2011), more health spending has a long-term positive influence on GDP growth. Wang (2011) looked studied the relationship between health spending and GDP growth in 31 countries, including in the years 1986–2007. In contrast, Zaidi and Saidi (2018) showed through modeling the long run and short run using the estimating approach ARDL that economic growth has a favorable impact on health expenses. Gerdtham and Löthgren (2002) discovered that for 12 of the OECD conutries, health expenditure and GDP growth are co-integrated in their study of the co-integration between health spending and GDP growth in the 25 OECD countries from 1960 to 1997. Similar to this, Tang (2011) found that from 1970 to 2009, Malaysia’s GDP and health spending were co-integrated.
3 Material and methods
3.1 Data
The study uses GDP per capita (GDP) (constant 2015 \({{\text{US}}\$}\)), health expenditure (HE) (US$ per capita), and population (Pop) (total) as independent variables, with CO2 emissions (CO2) (metric tons per capita) as a dependent variable. The natural logarithm form is applied to all variables. To ensure that the data were distributed regularly, this was done (Rjoub et al., 2021; Kirikkaleli et al., 2021). The variables, research abbreviations, and measurement methods are listed in Table 1. Additionally, Table 2 displays the variables’ descriptive statistics.
3.2 Modeling and methodological framework
This study aims to investigate the relationship between health expenditures, CO2 emissions, and economic growth using data for Türkiye from 1975 to 2020. By drawing on the methodologies of Zaidi and Saidi (2018), Apergis et al. (2018), Karaaslan and Çamkaya (2022), Wang et al. (2019a), and Wang et al. (2019b), In order to evaluate the dynamic link between CO2, GDP, HE, and POP in Türkiye, this study creates a framework. The fundamental model is expressed as follows:
The natural logarithms of the variables were employed to remove multicollinearity between the variables, resulting in the natural logarithmic transformation of Eq. 1 described above.
In Eq. (2), where t stands for the years from 1975 to 2020, CO2 for CO2 emissions, HE for health expenses, GDP for gross domestic product per person, POP for the population, β for coefficient and \(\varepsilon\) for the error term.
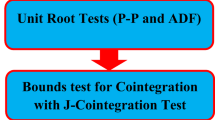
3.3 Unit root test
Before checking for the existence of a co-integration relationship between the variables, the integration levels of the series should be defined. The augmented Dickey-Fuller (ADF) (1979) and Phillips-Perron (PP) (1988) unit root tests were used to ascertain the levels of integration of the variables in this investigation. The alternative hypothesis in these tests is that there is no unit root, which would imply that the series is stationary. According to the null hypothesis in these tests, there is a unit root, which suggests that the series is not stationary. The results of the unit root test are shown in Table 3.
None of the variables in the ADF and PP unit root tests are level stationary, except for POP. However, when the first difference between the variables is considered, they are all stationary. This illustrates that the variables’ order of integration is a mixture of I (1) and I (0). These outcomes enable the use of the ARDL limit test.
3.4 The ARDL approach
The autoregressive distributed lag (ARDL) model, first introduced by Shin and Pesaran (1999) and developed by Pesaran et al. (2001), addresses single cointegration. The ARDL method has the benefit of allowing I(0) and I(1) variables in a set without requiring that they all be I(1) variables. The ARDL approach has been employed in most research, including the current study, because of its convenience. As a result, this method has been used to determine the series’ long-term connection. Equation (2) can be rewritten as an ARDL formula as the model with intercept in Eq. (3) as follows:
The Bounds test is used to examine whether the variables have a long-term relationship. The alternative hypothesis (H1: β5 ≠ β6 ≠ β7 ≠ β8) contradicts the null hypothesis (H0: β5 ═ β6 ═ β7 ═ β8), which implies that there is no cointegration. The null hypothesis will be rejected if the estimated F statistic is greater than the upper bound critical value I (1) for the number of explanatory variables (k) proposed by Pesaran et al. The null hypothesis cannot be proved if the F statistic is lower than the lower bound critical value I (0). The F statistic indicates uncertainty regarding cointegration when it is between I (0) and I (1). Alternative critical values I (0) and I (1), which are more suitable than those of small sample sizes, were proposed by Narayan. The optimal lag values p and q in Eqs. (3) and (4) are determined by model selection criteria such as Akaike (AIC) or Schwarz (SIC). Optimal p and q are implied by the model’s minimal AIC or SIC. Additionally, the residuals of the model cannot have serial correlation. The model with the highest R-squared value or the smallest information criterion is the one that has the best estimation. Last but not least, the following equation estimates the short-run estimation of the ARDL model, also referred to as the error-correction model:
The speed of adjustment parameter, also known as the coefficient of the error-correction term (\({ECM}_{t-1}\)) \(\lambda\) in Eq. (4), determines how quickly the series achieves long-run equilibrium. The model is put through diagnostic tests to ensure its suitability, including tests for serial correlation, normalcy, functional form, and heteroscedasticity. Brown et al. used stability tests such as the cumulative sum (CUSUM) and cumulative sum of squares (CUSUMSQ) to determine whether the coefficients on the graphical representations were stable.
4 The empirical results
This study’s main aim is to give empirical evidence of how health expenditure and economic growth affect CO2 emissions. The study first uses the co-integration of bound test to analyze the data set, then long-run and short-run estimate findings, and lastly the cumulative sum (CUSUM) and cumulative sum of squares (CUSUMSQ) test results are described.
We ran a bounds test using the following model specifications: unrestricted intercept and no trend (case III) based on the estimated ARDL model (4,6,4,6). Table 4 shows the estimated F test as well as the equivalent Narayan (2005) critical values for the lower and upper boundaries. According to the F computed values when compared to critical values, the null hypothesis of no cointegration is firmly rejected. This demonstrates that in Türkiye, there is a long-run link between CO2, health spending, economic growth, and population.
Table 5 displays the long-run and short-run estimate findings. All of the coefficients (long-run estimates) are significant. Economic growth has a statistically significant positive effect on CO2 emissions. Economic growth of 1% increased CO2 emissions by 0.297. Previous research are supported by our empirical results (Ahmed & Long, 2012; Bouznit & Pablo-Romero, 2016; He & Lin, 2019; Kanjilal & Ghosh, 2013; Pata, 2018; Shahbaz et al., 2013; Suki et al. 2020)). These findings are consistent with Türkiye’s growth trends because the manufacturing industry and transportation services are two essential areas that drive economic growth in Türkiye. The energy used in the manufacturing industry and transportation services in Türkiye is mostly nonrenewable (natural gas, hard coal, coke, oil, lignite, and similar). This arrangement assures that CO2 emissions will rise in tandem with growth. In other words, it contributes to more pollution. What matters here is that renewable energy sources are prioritized over nonrenewable energy sources. Environmental pollution will be decreased as a result, as will steady growth.
In contrast, health investment boosts public awareness of pollution and reduces carbon emissions. Because the variable HE has a negative coefficient, CO2 decreases by 0.124% for every 1% rise in HE. The results are explained in terms of the decreased influence of increased health-care costs on pollution. Contrary to Narayan and Narayan (2008), Ullah et al. (2020), Wang et al. (2019b), and Blázquez-Fernández et al. (2019), these results are in line with those of Boachie et al. (2014), Apergis et al. (2018), Bilgili et al. (2021), and Karaaslan and Çamkaya (2022). These results, our long-run elasticity estimates demonstrate that a rise in health care spending relative to GDP lowers CO2 emissions. This is most likely because the healthcare industry uses more renewable energy (like solar energy) and/or is more efficient at using fossil fuels than the other economic sectors. Population growth and health expenses are linked, therefore as the population rises, more energy is spent, increasing pollution. Our findings corroborate Türkiye’s position. For every 1% increase in POP, CO2 rises by 1.523%.
The short-run GDP connection, like the long-run relationship, increased CO2 emissions by 0.553% (Table 5). In contrast to the long-term connection, HE increased CO2 emissions by 0.037% in the short run. Furthermore, Table 5 reveals that short-term population increase is unrelated to emissions. The equilibrium correction mechanism (ECM) is a statistical model used to investigate the connection between two or more non-stationary variables that tend to trend over time. The error correction term in the ECM model is the difference between the current value of the dependent variable and its equilibrium level. The error correction term’s coefficient reflects the rate at which the dependent variable adjusts to departures from its long-run equilibrium. In other words, it measures the pace at which a shock or disturbance causes the dependent variable to converge to its equilibrium level. The error correction term coefficient is an essential parameter in the ECM model because it gives vital information about the dynamics of the relationship between the variables being researched. A high coefficient value implies that the dependent variable quickly adapts to departures from equilibrium, whereas a low coefficient value indicates that the adjustment process is longer. The coefficient of the error correction term is negative and statistically significant, as predicted (Table 5). When CO2 emissions are far from their equilibrium level, they adapt by around 84% within the first year. After complete convergence, it takes around 1/0.839 = 1.19 years to reach the equilibrium level.
Diagnostic testing on ARDL models are critical for verifying the correctness and dependability of the results. The diagnostic test results are also provided at the bottom of Table 5. As a result of these findings, the model exhibits no autocorrelation or heteroskedasticity issues and a normal distribution with no model setup error. CUSUM and CUSUMSQ tests were also done to determine whether there is a structural break in the series, as illustrated in Fig. 1.

CUSUM and CUSUM of square
According to the CUSUM and CUSUMSQ test findings, the statistics are between the critical boundaries (5% significance level), indicating that the coefficients are stable during the research time; that is, the results may be understood to mean that the estimated parameters are stable throughout the research period.
5 Conclusion
This study examined the short- and long-run links between health expenditures, CO2 emissions, and economic growth in Türkiye from 1975 to 2020. The data were examined using the Autoregressive Distributed Lagged (ARDL) cointegration methodology developed by Pesaran et al. (2001). The investigation uncovers a number of interesting conclusions. First, there is evidence in Türkiye of a long-run co-integrating connection between CO2 emissions, economic growth, healthy expenditure, and population expansion. Second, just as in the long run, a relationship was discovered between these factors in the short term. In the long and short term, each 1% rise in economic growth increased CO2 emissions by 0.297 and 0.553, respectively, from 1975 to 2020. According to the study, economic growth may have a negative impact on CO2 emissions in Türkiye in the long and short run if it cannot be done with renewable energy. Balancing economic growth with CO2 emissions reductions is thus a daunting problem that needs a comprehensive and coordinated strategy. This policy proposal highlights the need to implement sustainable practices to foster economic growth while mitigating the negative consequences of climate change. We can pave the road for a greener and more prosperous future by establishing emission reduction goals, supporting renewable energy sources, enhancing energy efficiency, switching to low-carbon transportation, putting carbon price systems into place, and encouraging international collaboration. Besides, governments, corporations, and people all need to understand how urgent it is to combat climate change and accept their roles as contributors to sustainable development. In order to create a sustainable balance between economic growth and environmental preservation, this proposal highlights the need for creative solutions, technology improvements, and behavioral adjustments. However, the success of these policies relies on practical implementation, continuous monitoring, and adaptive measures. To ensure that policies remain in line with developing scientific understanding, technological improvements, and shifting economic environments, regular analyses and reviews are required.
In order to address the health hazards and difficulties brought on by high emissions of carbon dioxide, health expenditure is crucial. Spending more on healthcare systems has the potential to increase public health efforts, disease prevention and control, and access to medical treatment. These initiatives are essential for reducing the damaging impacts on human health brought on by pollution and environmental deterioration brought on by CO2 emissions. Societies can better address the health effects of climate change and advance sustainable development by investing in healthcare infrastructure, research, and education. It demonstrates that the link between health expenditures and CO2 emissions reflects this condition, i.e., in the long run, CO2 decreases by 0.124% for every 1% rise in health expenditure, but this conclusion has little importance in the short run. Furthermore, the study suggests that population growth in Türkiye may have a detrimental long-term impact on CO2 emissions.
References
Ahmed, K., & Long, W. (2012). Environmental Kuznets curve and Pakistan: An empirical analysis. Procedia Economics and Finance, 1, 4–13.
Akram, N., Padda, I. U. H., & Khan, M. (2008). The long term impact of health on economic growth in Pakistan. Pakistan Development Review, 47(4), 487–500.
Apergis, N., & Payne, J. E. (2010). The emissions, energy consumption, and growth nexus: evidence from the commonwealth of independent states. Energy policy, 38(1), 650–655.
Apergis, N., Jebli, M. B., & Youssef, S. B. (2018). Does renewable energy consumption and health expenditures decrease carbon dioxide emissions? Evidence for sub-Saharan Africa countries. Renewable Energy, 127, 1011–1016.
Arouri, M. E. H., Youssef, A. B., M’henni, H., & Rault, C. (2012). Energy consumption, economic growth and CO2 emissions in Middle East and North African countries. Energy policy, 45, 342–349.
Baltagi, B. H., & Moscone, F. (2010). Health care expenditure and income in the OECD reconsidered: Evidence from panel data. Economic Modelling, 27(4), 804–811.
Begum, R. A., Sohag, K., Abdullah, S. M. S., & Jaafar, M. (2015). CO2 emissions, energy consumption, economic and population growth in Malaysia. Renewable and Sustainable Energy Reviews, 41, 594–601.
Béral-Guyonnet, I. (1996). Influence des facteurs météorologiques sur la pollution atmosphérique: le cas de l’agglomération lyonnaise/The influence of meteorological factors on atmospheric pollution: The case of the city of Lyon. Géocarrefour, 71(1), 71–77.
Bilgili, F., Kuşkaya, S., Khan, M., Awan, A., & Türker, O. (2021). The roles of economic growth and health expenditure on CO2 emissions in selected Asian countries: A quantile regression model approach. Environmental Science and Pollution Research, 28, 44949–44972.
Blázquez-Fernández, C., Cantarero-Prieto, D., & Pascual-Sáez, M. (2019). On the nexus of air pollution and health expenditures: New empirical evidence. Gaceta Sanitaria, 33, 389–394.
Bloom, D., & Canning, D. (2003a). The health and poverty of nations: From theory to practice. Journal of Human Development, 4(1), 47–71.
Bloom, D., & Canning, D. (2003b). Health as human capital and its impact on economic performance. The Geneva Papers on Risk and Insurance: Issues and Practice, 28(2), 304–315.
Boachie, M. K., Mensah, I. O., Sobiesuo, P., Immurana, M., Iddrisu, A. A., & Kyei-Brobbey, I. (2014). Determinants of public health expenditure in Ghana: a cointegration analysis. Journal of Behavioural Economics, Finance, Entrepreneurship, Accounting and Transport, 2(2), 35–40.
Bouznit, M., & Pablo-Romero, M. D. P. (2016). CO2 emission and economic growth in Algeria. Energy Policy, 96, 93–104.
Burnett, R. T., Cakmak, S., & Brook, J. R. (1998). The effect of the urban ambient air pollution mix on daily mortality rates in 11 Canadian cities. Canadian Journal of Public Health, 89, 152–156.
Cai, Y., Sam, C. Y., & Chang, T. (2018). Nexus between clean energy consumption, economic growth and CO2 emissions. Journal of Cleaner Production, 182, 1001–1011.
Dağ, K., & Kızılkaya, F. (2021). Examining health expenditures, CO2 emissions and economic growth nexus for Turkey. Journal of Management and Economics Research, 19(3), 211–229.
Dickey, D. A., & Fuller, W. A. (1979). Distribution of the estimators for autoregressive time series with a unit root. Journal of the American Statistical Association, 74(366a), 427–431.
Dinda, S. (2004). Environmental Kuznets curve hypothesis: A survey. Ecological Economics, 49(4), 431–455.
Erçelik, G. (2018). The relationship between health expenditure and economic growth in Turkey from 1980 to 2015. Journal of Politics Economy and Management, 1(1), 1–8.
Gerdtham, U. G., & Löthgren, M. (2002). New panel results on cointegration of international health expenditure and GDP. Applied Economics, 34(13), 1679–1686.
Ghorashi, N., & Rad, A. A. (2017). CO2 emissions, health expenditures and economic growth in Iran: Application of dynamic simultaneous equation models. Journal of Community Health Research, 6(2), 109–116.
Gökmenoğlu, K., & Taspinar, N. (2016). The relationship between CO2 emissions, energy consumption, economic growth and FDI: The case of Turkey. The Journal of International Trade & Economic Development, 25(5), 706–723.
He, Y., & Lin, B. (2019). Investigating environmental Kuznets curve from an energy intensity perspective: Empirical evidence from China. Journal of Cleaner Production, 234, 1013–1022.
Iwata, H., Okada, K., & Samreth, S. (2010). Empirical study on the environmental Kuznets curve for CO2 in France: The role of nuclear energy. Energy Policy, 38(8), 4057–4063.
Jalil, A., & Mahmud, S. F. (2009). Environment Kuznets curve for CO2 emissions: A cointegration analysis for China. Energy Policy, 37(12), 5167–5172.
Kanjilal, K., & Ghosh, S. (2013). Environmental Kuznet’s curve for India: Evidence from tests for cointegration with unknown structural breaks. Energy Policy, 56, 509–515.
Karaaslan, A., & Çamkaya, S. (2022). The relationship between CO2 emissions, economic growth, health expenditure, and renewable and non-renewable energy consumption: Empirical evidence from Turkey. Renewable Energy, 190, 457–466.
Kayani, G. M., Ashfaq, S., & Siddique, A. (2020). Assessment of financial development on environmental effect: Implications for sustainable development. Journal of Cleaner Production, 261, 120984.
Khoshnevis Yazdi, S., & Khanalizadeh, B. (2017). Air pollution, economic growth and health care expenditure. Economic Research-Ekonomska Istraživanja, 30(1), 1181–1190.
Kirikkaleli, D., Adebayo, T. S., Khan, Z., & Ali, S. (2021). Does globalization matter for ecological footprint in Turkey? Evidence from dual adjustment approach. Environmental Science and Pollution Research, 28(11), 14009–14017.
Li, Y., Chiu, Y. H., & Lin, T. Y. (2019). The impact of economic growth and air pollution on public health in 31 Chinese cities. International Journal of Environmental Research and Public Health, 16(3), 393.
Liu, J., Qu, J., & Zhao, K. (2019). Is China’s development conforms to the Environmental Kuznets Curve hypothesis and the pollution haven hypothesis? Journal of Cleaner Production, 234, 787–796.
Lotfalipour, M. R., Falahi, M. A., & Ashena, M. (2010). Economic growth, CO2 emissions, and fossil fuels consumption in Iran. Energy, 35(12), 5115–5120.
Lucian, U., Oreste, S., Traian, M. T., & Tudor, B. C. (2009). Relationship and causality between economic growth rate and certain diseases in the European Union. Annals of Faculty of Economics, 1(1), 478–484.
Marrero, G. A. (2010). Greenhouse gases emissions, growth and the energy mix in Europe. Energy Economics, 32(6), 1356–1363.
Mehmood, B., Raza, S. H., & Mureed, S. (2014). Health expenditure, literacy and economic growth: PMG evidence from Asian countries. Euro-Asian Journal of Economics and Finance, 2(4), 408–417.
Mehmood, U., Agyekum, E. B., Kamel, S., Shahinzadeh, H., & Moshayedi, A. J. (2022). Exploring the roles of renewable energy, education spending, and CO2 emissions towards health spending in South Asian countries. Sustainability, 14(6), 3549.
Mehrara, M., Fazaeli, A. A., Fazaeli, A. A., & Fazaeli, A. R. (2012). The relationship between health expenditures and economic growth in Middle East & North Africa (MENA) countries. International Journal of Business Management and Economic Research, 3(1), 425–428.
Mikayilov, J. I., Galeotti, M., & Hasanov, F. J. (2018). The impact of economic growth on CO2 emissions in Azerbaijan. Journal of Cleaner Production, 197, 1558–1572.
Mujtaba, A., & Jena, P. K. (2021). Analyzing asymmetric impact of economic growth, energy use, FDI inflows, and oil prices on CO2 emissions through NARDL approach. Environmental Science and Pollution Research, 28, 30873–30886.
Mujtaba, G., & Shahzad, S. J. H. (2021). Air pollutants, economic growth and public health: Implications for sustainable development in OECD countries. Environmental Science and Pollution Research, 28, 12686–12698.
Muntean, M., Guizzardi, D., Schaaf, E., Crippa, M., Solazzo, E., Olivier, J., & Vignati, E. (2018). Fossil CO2 emissions of all world countries. Luxembourg: Publications Office of the European Union, 2.
Murthy, V. N., & Okunade, A. A. (2016). Determinants of US health expenditure: Evidence from autoregressive distributed lag (ARDL) approach to cointegration. Economic Modelling, 59, 67–73.
Musibau, H. O., Shittu, W. O., & Ogunlana, F. O. (2021). The relationship between environmental degradation, energy use and economic growth in Nigeria: New evidence from non-linear ARDL. International Journal of Energy Sector Management, 15(1), 81–100.
Narayan, P. K. (2005). The saving and investment nexus for China: Evidence from cointegration tests. Applied Economics, 37(17), 1979–1990.
Narayan, P. K., & Narayan, S. (2008). Does environmental quality influence health expenditures? Empirical evidence from a panel of selected OECD countries. Ecological Economics, 65(2), 367–374.
Nasiru, I., & Usman, H. M. (2012). Health expenditure and economic growth nexus: An ARDL approach for the case of Nigeria. Journal of Research in National Development, 10(3), 95–100.
Pao, H. T., & Tsai, C. M. (2010). CO2 emissions, energy consumption and economic growth in BRIC countries. Energy Policy, 38(12), 7850–7860.
Pata, U. K. (2018). Renewable energy consumption, urbanization, financial development, income and CO2 emissions in Turkey: Testing EKC hypothesis with structural breaks. Journal of Cleaner Production, 187, 770–779.
Pesaran, M. H., Shin, Y., & Smith, R. J. (2001). Bounds testing approaches to the analysis of level relationships. Journal of Applied Econometrics, 16(3), 289–326.
Phillips, P. C., & Perron, P. (1988). Testing for a unit root in time series regression. Biometrika, 75(2), 335–346.
Pontarollo, N., & Muñoz, R. M. (2020). Land consumption and income in Ecuador: A case of an inverted environmental Kuznets curve. Ecological Indicators, 108, 105699.
Richmond, A. K., & Kaufmann, R. K. (2006). Is there a turning point in the relationship between income and energy use and/or carbon emissions? Ecological Economics, 56(2), 176–189.
Rivera, B., & Currais, L. (2003). The effect of health investment on growth: A causality analysis. International Advances in Economic Research, 9(4), 312–323.
Rjoub, H., Odugbesan, J. A., Adebayo, T. S., & Wong, W. K. (2021). Sustainability of the moderating role of financial development in the determinants of environmental degradation: Evidence from Turkey. Sustainability, 13(4), 1844.
Robalino-López, A., Mena-Nieto, Á., García-Ramos, J. E., & Golpe, A. A. (2015). Studying the relationship between economic growth, CO2 emissions, and the environmental Kuznets curve in Venezuela (1980–2025). Renewable and Sustainable Energy Reviews, 41, 602–614.
Shahbaz, M., Hye, Q. M. A., Tiwari, A. K., & Leitão, N. C. (2013). Economic growth, energy consumption, financial development, international trade and CO2 emissions in Indonesia. Renewable and Sustainable Energy Reviews, 25, 109–121.
Shin, Y., & Pesaran, M. H. (1999). An autoregressive distributed lag modelling approach to cointegration analysis. In S. Strom (ed.) Econometrics and Economic Theory in the 20th century: The Ragnar Frish Centennial Symposium, (pp. 371–413). Cambridge University Press.
Soytas, U., Sari, R., & Ewing, B. T. (2007). Energy consumption, income, and carbon emissions in the United States. Ecological Economics, 62(3–4), 482–489.
Suki, N. M., Sharif, A., Afshan, S., & Suki, N. M. (2020). Revisiting the environmental Kuznets curve in Malaysia: The role of globalization in sustainable environment. Journal of Cleaner Production, 264, 121669.
Tang, C. F. (2011). Multivariate Granger causality and the dynamic relationship between health care spending, income and relative price of health care in Malaysia. Hitotsubashi Journal of Economics, 52, 199–214.
Ullah, I., Rehman, A., Khan, F. U., Shah, M. H., & Khan, F. (2020). Nexus between trade, CO2 emissions, renewable energy, and health expenditure in Pakistan. The International Journal of Health Planning and Management, 35(4), 818–831.
Wang, K. M. (2011). Health care expenditure and economic growth: Quantile panel-type analysis. Economic Modelling, 28(4), 1536–1549.
Wang, S. S., Zhou, D. Q., Zhou, P., & Wang, Q. W. (2011). CO2 emissions, energy consumption and economic growth in China: A panel data analysis. Energy Policy, 39(9), 4870–4875.
Wang, C. M., Hsueh, H. P., Li, F., & Wu, C. F. (2019a). Bootstrap ARDL on health expenditure, CO2 emissions, and GDP growth relationship for 18 OECD countries. Frontiers in Public Health, 7, 324.
Wang, Z., Asghar, M. M., Zaidi, S. A. H., & Wang, B. (2019b). Dynamic linkages among CO2 emissions, health expenditures, and economic growth: Empirical evidence from Pakistan. Environmental Science and Pollution Research, 26, 15285–15299.
Zaidi, S., & Saidi, K. (2018). Environmental pollution, health expenditure and economic growth in the Sub-Saharan Africa countries: Panel ARDL approach. Sustainable Cities and Society, 41, 833–840.
Zhou, C., Wang, S., & Wang, J. (2019). Examining the influences of urbanization on carbon dioxide emissions in the Yangtze River Delta, China: Kuznets curve relationship. Science of the Total Environment, 675, 472–482.
Funding
Open access funding provided by the Scientific and Technological Research Council of Türkiye (TÜBİTAK). The authors have no conflicts of interest to declare that are relevant to the content of this article.
Author information
Authors and Affiliations
Contributions
The author’s contribution to the article is 100%.
Corresponding author
Ethics declarations
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors did not receive support from any organization for the submitted work.
Availability of data and materials
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Çobanoğulları, G. Exploring the link between CO2 emissions, health expenditure, and economic growth in Türkiye: evidence from the ARDL model. Environ Dev Sustain (2024). https://doi.org/10.1007/s10668-024-04835-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10668-024-04835-8