
Abstract
Objective
The purpose of this consensus conference was to determine whether video-assisted thoracic surgery (VATS) improves clinical outcomes compared with conventional thoracotomy in patients undergoing surgery for pneumothorax, and to outline evidence-based recommendations for the use of VATS.
Methods
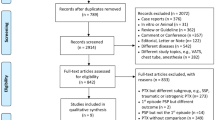
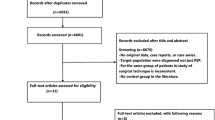
Before the consensus conference, the best available evidence was reviewed, with systematic reviews, randomized trials, and nonrandomized trials all taken into consideration in descending order of validity and importance. At the consensus conference, evidence-based interpretative statements were created, and consensus processes were used to determine the ensuing recommendations. The Medical Information Network Distribution Service in Japan (Minds) system was used to label the levels of evidence for the references and the classes of recommendations.
Results and recommendations
The consensus panel agreed upon the following statements and recommendations for patients with pneumothorax undergoing surgery:
-
1.
VATS is broadly indicated as surgery for pneumothorax.
-
2.
VATS is judged to be less invasive, as it results in minimal postoperative pain, the periods of chest tube placement and hospitalization are short, and it shows a trend toward early realization of social integration.
-
3.
There is no difference in terms of safety and complications between VATS and open thoracotomy.
-
4.
As it is anticipated that VATS will result in a higher recurrence rate than open thoracotomy, it may be desirable to add a supplemental procedure during surgery.
In summary, VATS can be recommended as pneumothorax surgery (Recommendation grade: Level B).
Similar content being viewed by others

Abbreviations
- VATS:
-
Video-assisted thoracic surgery
- RCT:
-
Randomized controlled trial
References
Hunter JG. Minimally invasive surgery: the next frontier. World J Surg. 1999;23:422–4.
Yim AP, Wan S, Lee TW, Arifi AA. VATS lobectomy reduces cytokine responses compared with conventional surgery. Ann Thorac Surg. 2000;70:243–7.
Vittimberga FJ Jr, Foley DP, Meyers WC, Callery MP. Laparoscopic surgery and the systemic immune response. Ann Surg. 1998;227:326–34.
McCulloch P. Half full or half empty VATS? BMJ. 2004;329:1012.
Sedrakyan A, van der Meulen J, Lewsey J, Treasure T. Variation in use of video assisted thoracic surgery in the United Kingdom. BMJ. 2004;329:1011–2.
Sedrakyan A, van der Meulen J, Lewsey J, Treasure T. Video assisted thoracic surgery for treatment of pneumothorax and lung resections: systematic review of randomised clinical trials. BMJ. 2004;329:1008 (Evidence Level: I).
Fukui T, Yoshida M, Yamaguchi N. Minds 2007 Manual for Production of Clinical Guidelines. Tokyo: Igakushoin; 2007.
Kuwano H, Amano J, Yokomise H. Thoracic and cardiovascular surgery in Japan during 2010: annual report by The Japanese Association for Thoracic Surgery. Gen Thorac Cardiovasc Surg. 2012;60:680–708 (Evidence Level: IV).
MacDuff A, Arnold A, Harvey J. Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65 Suppl 2:ii18–31.
Watanabe M, Sato M, Deguchi H, Tsumatori G, Aoki T, Takagi K, et al. Thoracoscopic treatment for spontaneous pneumothorax in patients over 50 years old: a comparison with younger patients. Surg Laparosc Endosc. 1996;6:181–3 (Evidence Level: IV).
Chung PH, Wong KK, Lan LC, Tam PK. Thoracoscopic bullectomy for primary spontaneous pneumothorax in pediatric patients. Pediatr Surg Int. 2009;25:763–6 (Evidence Level: IV).
Alifano M, Roth T, Broet SC, Schussler O, Magdeleinat P, Regnard JF. Catamenial pneumothorax: a prospective study. Chest. 2003;124:1004–8 (Evidence Level: III).
Foroulis CN, Anastasiadis K, Charokopos N, Antonitsis P, Halvatzoulis HV, Karapanagiotidis GT, et al. A modified two-port thoracoscopic technique versus axillary minithoracotomy for the treatment of recurrent spontaneous pneumothorax: a prospective randomized study. Surg Endosc. 2012;26:607–14 (Evidence Level: II).
Wu YC, Lu MS, Yeh CH, Liu YH, Hsieh MJ, Lu HI, et al. Justifying video-assisted thoracic surgery for spontaneous hemopneumothorax. Chest. 2002;122:1844–7 (Evidence Level: IV).
Balduyck B, Hendriks J, Lauwers P, Van Schil P. Quality of life evolution after surgery for primary or secondary spontaneous pneumothorax: a prospective study comparing different surgical techniques. Interact Cardiovasc Thorac Surg. 2008;7:45–9 (Evidence Level: III).
Freixinet JL, Canalis E, Julia G, Rodriguez P, Santana N, Rodriguez de Castro F. Axillary thoracotomy versus videothoracoscopy for the treatment of primary spontaneous pneumothorax. Ann Thorac Surg. 2004;78:417–20 (Evidence Level: II).
Sekine Y, Miyata Y, Yamada K, Yamada H, Yasukawa T, Saitoh Y, et al. Video-assisted thoracoscopic surgery does not deteriorate postoperative pulmonary gas exchange in spontaneous pneumothorax patients. Eur J Cardiothorac Surg. 1999;16:48–53 (Evidence Level: II).
Gebhard FT, Becker HP, Gerngross H, Bruckner UB. Reduced inflammatory response in minimal invasive surgery of pneumothorax. Arch Surg. 1996;131:1079–82 (Evidence Level: II).
Schramel FM, Sutedja TG, Braber JC, van Mourik JC, Postmus PE. Cost-effectiveness of video-assisted thoracoscopic surgery versus conservative treatment for first time or recurrent spontaneous pneumothorax. Eur Respir J. 1996;9:1821–5 (Evidence Level: IV).
Cardillo G, Facciolo F, Giunti R, Gasparri R, Lopergolo M, Orsetti R, et al. Videothoracoscopic treatment of primary spontaneous pneumothorax: a 6-year experience. Ann Thorac Surg. 2000;69:357–61 (discussion 61–62; Evidence Level: IV).
Naunheim KS, Mack MJ, Hazelrigg SR, Ferguson MK, Ferson PF, Boley TM, et al. Safety and efficacy of video-assisted thoracic surgical techniques for the treatment of spontaneous pneumothorax. J Thorac Cardiovasc Surg. 1995;109:1198–203 (discussion 203–204; Evidence Level: IV).
Lang-Lazdunski L, Chapuis O, Bonnet PM, Pons F, Jancovici R. Videothoracoscopic bleb excision and pleural abrasion for the treatment of primary spontaneous pneumothorax: long-term results. Ann Thorac Surg. 2003;75:960–5 (Evidence Level: IV).
Kitano M, Yamashita Y, Shiraishi N, Hashizume M, Kitagawa Y, Endo S, et al. 11th Nationwide Survey of Endoscopic Surgery in Japan. J Jpn Soc Endosc Surg. 2012;17:571–694 (Evidence Level: V).
Rieger R, Woisetschlager R, Schrenk P, Wayand W. Thoracoscopic bleb resection selectively combined with pleurectomy for complicated spontaneous pneumothorax. Eur J Surg. 1998;164:333–8 (Evidence Level: IV).
Kraenzler EJ, Hearn CJ. Anesthetic considerations for video-assisted thoracic surgery. Semin Thorac Cardiovasc Surg. 1993;5:321–6 (Evidence Level: IV).
Sihoe AD, Au SS, Cheung ML, Chow IK, Chu KM, Law CY, et al. Incidence of chest wall paresthesia after video-assisted thoracic surgery for primary spontaneous pneumothorax. Eur J Cardiothorac Surg. 2004;25:1054–8 (Evidence Level: IV).
Nishimura M, Kobayashi M, Hamagashira K, Noumi S, Ito K, Kato D, et al. Quadrilateral space syndrome: a rare complication of thoracic surgery. Ann Thorac Surg. 2008;86:1350–1 (Evidence Level: V).
Gonzalez AV, Bezwada V, Beamis JF Jr, Villanueva AG. Lung injury following thoracoscopic talc insufflation: experience of a single North American center. Chest. 2010;137:1375–81 (Evidence Level: IV).
Sawada S, Watanabe Y, Moriyama S. Video-assisted thoracoscopic surgery for primary spontaneous pneumothorax: evaluation of indications and long-term outcome compared with conservative treatment and open thoracotomy. Chest. 2005;127:2226–30 (Evidence Level: IV).
Matsuzoe D, Iwasaki A, Okabayashi K, Shiraishi T, Inada K, Yoneda S, et al. Recurrence after thoracoscopic surgery for spontaneous pneumothorax. Int Surg. 1999;84:111–4 (Evidence Level: IV).
Muramatsu T, Nishii T, Takeshita S, Ishimoto S, Morooka H, Shiono M. Preventing recurrence of spontaneous pneumothorax after thoracoscopic surgery: a review of recent results. Surg Today. 2010;40:696–9 (Evidence Level: IV).
Barker A, Maratos EC, Edmonds L, Lim E. Recurrence rates of video-assisted thoracoscopic versus open surgery in the prevention of recurrent pneumothoraces: a systematic review of randomised and non-randomised trials. Lancet. 2007;370:329–35 (Evidence Level: I).
Chen JS, Hsu HH, Chen RJ, Kuo SW, Huang PM, Tsai PR, et al. Additional minocycline pleurodesis after thoracoscopic surgery for primary spontaneous pneumothorax. Am J Respir Crit Care Med. 2006;173:548–54 (Evidence Level: IV).
Sakamoto K, Takei H, Nishii T, Maehara T, Omori T, Tajiri M, et al. Staple line coverage with absorbable mesh after thoracoscopic bullectomy for spontaneous pneumothorax. Surg Endosc. 2004;18:478–81 (Evidence Level: IV).
Nakanishi K. An apical symphysial technique using a wide absorbable mesh placed on the apex for primary spontaneous pneumothorax. Surg Endosc. 2009;23:2515–21 (Evidence Level: IV).
Chen JS, Hsu HH, Huang PM, Kuo SW, Lin MW, Chang CC, et al. Thoracoscopic pleurodesis for primary spontaneous pneumothorax with high recurrence risk: a prospective randomized trial. Ann Surg. 2012;255:440–5 (Evidence Level: II).
Conflict of interest
The authors have no competing interests to declare.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is based on a study first reported in “Clinical Guidelines of Endoscopic Surgery, 2nd Edition, Wiley-JAPAN, Tokyo (Japanese, in press)”.
This review was submitted at the invitation of the editorial committee.
Rights and permissions
About this article

Cite this article
Goto, T., Kadota, Y., Mori, T. et al. Video-assisted thoracic surgery for pneumothorax: republication of a systematic review and a proposal by the guideline committee of the Japanese Association for Chest Surgery 2014. Gen Thorac Cardiovasc Surg 63, 8–13 (2015). https://doi.org/10.1007/s11748-014-0468-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-014-0468-9