
Abstract
Background
Bariatric surgery contributes to the improvement in glucose metabolism that may be related to a postoperative increase in serum bile acids (BAs). Three commonly used types of bariatric procedures, laparoscopic sleeve gastrectomy (LSG) (without creation of a bile loop), Roux-en-Y gastric bypass (RYGB), and omega-loop gastric bypass (OLGB) (with creation of shorter 100–150 cm and longer 200–280 cm bile loops, respectively), differ in their effects on glycemic control. The aim of the study was to compare the effects of various bariatric procedures on serum BA concentration and glucose homeostasis.
Methods
Serum BAs in 26 obese patients were determined by liquid chromatography-mass spectrometry prior to bariatric surgery, as well as 4 days and 3 months thereafter.
Results
Four days after the surgery, serum concentrations of BAs in LSG and OLGB groups were similar as prior to the procedure, and a slight decrease in serum BAs was observed in the RYGB group. Serum BA level in the LSG group remained unchanged also at 3 months after the surgery, whereas a significant 0.5- and 3-fold increase in this parameter was noted in the RYGB and OLGB groups, respectively. Serum concentration of BAs correlated positively with the length of the bile loop (R = 0.47, p < 0.05).
Conclusion
The evident improvement of glycemic control observed 3 months after OLGB might be associated with a postoperative increase in serum BAs, resulting from their better absorption from the longer bile loop. However, the changes in serum BAs probably had little or no impact on insulin sensitivity improvement at 4 days post-surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obesity is a major public health problem worldwide; it is frequently associated with various comorbidities, such as diabetes mellitus, metabolic syndrome, lipid disorders, cholelithiasis, sleep apnea, nonalcoholic fatty liver disease, chronic kidney disease, cardiovascular diseases, and some malignancies [1,2,3,4]. Due to the lack of other effective therapies, bariatric surgeries are performed in obese patients with type 2 diabetes mellitus (T2DM) and were shown to induce the remission of diabetes in this group. The most commonly used bariatric procedures include Roux-en-Y gastric bypass (RYGB), omega-loop gastric bypass (OLGB), and laparoscopic sleeve gastrectomy (LSG). All these procedures result not only in a weight loss but also in the resolution of hyperglycemia, insulin resistance, and T2DM, all observed within hours or days after the surgery, well before the reduction of body weight [5, 6]. Although the exact mechanism underlying the beneficial effect of bariatric surgeries on glucose metabolism is still not fully understood, some evidence points to potential involvement of bile acids (BAs) [7]. BAs are a heterogeneous group of compounds with different biological functions and physicochemical properties. Primary BAs are synthesized in the liver; the vast majority of this pool is conjugated with glycine and taurine and released to the proximal duodenum. Approximately 5% of the primary BAs undergo transformation to secondary bile acids by intestinal microflora [8]. Ninety-five percent of BAs are reabsorbed from the intestine and delivered back to the liver. An overview of BA metabolism is presented in Supplementary Fig. 1.
While blood concentrations of BAs in healthy persons are generally low, they increase considerably in patients with hepatobiliary and intestinal diseases or drug-induced liver injury [9]. Elevated level of bile acids, especially secondary BAs and their conjugates, is particularly harmful for hepatocytes and colon cells, since the accumulation of these compounds may result in oxidative stress, apoptosis, and liver failure [10,11,12], or may stimulate colonic carcinogenesis [13]. However, an increase in serum BAs may also be beneficial, as it may be associated with the normalization of glucose metabolism after bariatric surgeries [8].
Also, body weight loss and/or calorie restriction have an impact on glucose and BA homeostasis [14, 15]. During malabsorptive procedures, such as various types of gastric bypass surgeries performed commonly nowadays, a small pouch is created in the stomach, connecting it with the proximal jejunum. As a result, BAs can reach the distal intestine and be absorbed by ileocytes [7]. In turn, during a restrictive procedure, such as LSG, a large part of the stomach is removed along the greater curvature [7]. These modifications of intestinal passage contribute to changes in the secretion of gut hormones and peptides and may affect both the absorption of BAs and the serum concentrations thereof [16]. BAs may influence glucose homeostasis acting on muscles, liver, adipose tissue, and pancreatic cells via nuclear FXR and membrane TGR-5 receptors [17, 18]. However, previous clinical trials of bariatric procedures produced inconclusive results with regard to prognosis in patients with T2DM. It is generally believed that RYGB provides better glycemic control than LSG. Many previous studies demonstrated that RYGB and LSG exert a plethora of effects on carbohydrate metabolism, contributing to a decrease in serum glucose, serum insulin, HOMA-IR, and HbA1c levels, and to an increase in serum GLP-1 [8]. The effect of RYGB on BA status is known better than that of LSG. Some evidence suggests that RYGB may stimulate an increase in primary, secondary, and conjugated BAs [19]. In contrast, LSG seems to exert less evident effect on circulating BAs or has no effect at all [20]. In our recent study, we observed the most evident improvement of insulin sensitivity after OLGB [7]. Therefore, we decided to compare the effects of various bariatric procedures (with a long or short bile loop, or without the loop) on the composition and concentration of serum BAs and glucose metabolism in morbidly obese patients. Moreover, we searched for plausible mechanisms explaining the differences in the outcomes of various bariatric procedures.
Material and Methods
Patients
Twenty six obese female patients aged 41 ± 2.2 years underwent bariatric surgeries at the Department of General, Endocrine and Transplant Surgery, Medical University of Gdansk (Poland). Seven patients (mean BMI 41 ± 1.6 kg/m2) were subjected to LSG, another nine (mean BMI 41 ± 1.0 kg/m2) to RYGB, and ten (mean BMI 44 ± 1.0 kg/m2) to OLGB. All study subjects were non-smokers, and none of them presented with a clinical evidence of heart, liver, and kidney diseases. Ten persons suffered from concomitant T2DM. Anthropometric and laboratory parameters of the study participants were determined prior to the surgery, as well as 4 days and 3 months thereafter. Blood samples for the analysis were collected after an overnight fast (from all 26 patients at each time point). Routine laboratory parameters were determined at the Central Clinical Laboratory, Medical University of Gdansk. All tests used in this study followed relevant protocols and guidelines. Selected biochemical and anthropometric characteristics of the study participants are presented in Table 1.
Surgical Technique
A 36-Fr calibration tube was used to confirm the volume restriction of the gastric sleeve or the gastric pouch (ca 40–45 ml). Since a long narrow reservoir has been constructed for OLGB to reduce the risk of the bile reflux, the same type of gastric tube was used in RYGB procedures to create the similar restriction conditions in both subgroups. The continuity of the digestive tract in LSG was preserved and no exclusion of the intestine was performed. The alimentary limb in RYGB operation has been established for 150 cm. The extent of biliopancreatic exclusion in both types of gastric bypass procedures was related to BMI, age, presence of diabetes, and the total length of the small intestine. The range in RYGB was 100–150 cm and that in OLGB was 200 to 250 cm, exceptionally 280 cm, where the total intestinal length approached 800 cm. The common limb has never been shorter than 300 cm in both gastric bypass procedures. The measurement of the intestinal loops was based on the not-strained organ manipulation and the 10-cm marker fixed to the grasping instrument was used to the equable calibration. All of the procedures were performed laparoscopically. The intra-operative complications and adverse events have not been experienced in the investigated cohort of patients. The average operation time was 62.5 min in the SG group and 75.6 and 90.8 min in the OLGB and RYGB groups respectively. All of the procedures were completed by the fixed team of the bariatric surgeons.
High-Performance Liquid Chromatography-Tandem Mass Spectrometry
Sample Collection and Storage
Blood samples were collected into tubes without anticoagulant and kept at room temperature for 30 min to allow clotting. Then, the material was centrifuged at 3000×g for 15 min at 4 °C. The separated sera were stored in aliquots at − 80 °C until the analysis.
Preparation of Standard Solutions
Standard stocks of all BAs and deuterated internal standards (IS, CA-d5) were diluted with methanol to obtain 10 μM solutions and stored in sealed glass vials at − 20 °C. Final solutions of individual BA standards and IS were obtained by diluting the 10 μM solutions with methanol and miliQ water mixture (50:50, v/v). Standard calibration curves were prepared for seven concentrations, from 0.1 to 100 μM.
Sample Preparation
The samples were prepared in glass tubes. First, each serum sample (250 μl) was mixed with 25 μl of IS. Then, 800 μl of cold acetonitrile was added for protein precipitation, and the sample was vortexed for 1 min, followed by a 15-min centrifugation at 4000×g at 25 °C. The supernatants were transferred to new tubes, dried in a stream of nitrogen, and the residue was dissolved in 250 μl of methanol and miliQ water mixture (50:50, v/v). Finally, 70 μl of the dissolved supernatant was transferred to 96-well plates for LC-MS/MS analysis.
Chromatography
Chromatographic separation was performed on a Biocrates® Bile Acids Kit (U)HPLC column (Biocrates, Innsbruck, Austria), using a Surveyor™ Plus high-performance liquid chromatography (HPLC) system (Thermo Fisher Scientific, USA). The mobile phase consisted of aqueous solution of 10 mM ammonium acetate with 0.015% formic acid (A), and acetonitrile and methanol mixture (325:150, v/v) with aqueous solution of 10 mM ammonium acetate and 0.015% formic acid (B). Each 5 μl sample was injected onto the column and subjected to gradient elution (0–1.05 min at 35% phase B, 9.45 min to 100% phase B, 1.5 min at 100% phase B, 0.30 min to 35% phase B, 2.5 min at 35% phase B). The whole chromatographic separation lasted 15 min at a maximum flow rate of 0.33 ml/ml, with maximum temperatures of a column oven and autosampler up to 50 and 4 °C, respectively.
Mass Spectrometry
Specific BAs were identified and quantified with the Thermo Scientific™ TSQ Vantage™ Triple Quadrupole Mass Spectrometer (Thermo Fisher Scientific, USA) working in negative ESI mode and multiple reaction monitoring (MRM) mode. Capillary voltage, capillary temperature, and source temperature were set at − 3000 V, 200 °C, and 200 °C, respectively. Transitions, collision energies, and S-Lens parameters are presented in Supplementary Table S1.
Data Analysis
Peak finding, filtering, alignment, and scaling to internal standard were carried out with Xcalibur QuanBrowser software, version 2.1 (Thermo Fisher Scientific, USA) capable of MRM data processing.
Statistical Analysis
Statistical significance of differences in pre- and postoperative values of the study variables was verified with paired t test. The significance of differences between the subgroups of patients subjected to three various types of bariatric surgeries was verified by ANOVA with an appropriate post hoc test. The differences were considered significant at p < 0.05. Power and direction of relationships between pairs of variables were determined by means of linear regression analysis. All statistical calculations were carried out with SigmaPlot software.
Results
Three months after bariatric surgery, significant improvements were observed in many study parameters, including BMI, serum triacylglycerols, total cholesterol, LDL cholesterol, glucose, HOMA, glycated hemoglobin (HbA1c), and CRP (Table 1, Fig. 1). OLBG contributed to the most evident improvement of BMI and HOMA and HbA1c levels (Fig. 1). A significant improvement in serum glucose and HOMA levels was observed at 4 days post-surgery as well, especially in the OLGB group, even despite a considerable increase in serum CRP suggesting the presence of a postoperative inflammation (Table 1). Irrespective of its type, bariatric surgery contributed to a significant decrease in HDL cholesterol concentration at both 4 days and 3 months, but without a concomitant change in LDL/HDL ratio (Table 1).

Changes in a BMI, b HOMA, and c HbA1c observed 3 months after various types of bariatric surgeries. *p < 0.05 vs. LSG, #p < 0.05 vs. RYGB
Four days after the surgery, serum concentrations of BAs in the LSG and OLGB groups were similar as prior to the procedure, and a slight albeit significant decrease in serum BAs was observed in the RYGB group (Fig. 2). While serum BA level in the LSG group remained also unchanged at 3 months post-surgery, a significant 0.5- and 3-fold increase in this parameter was noted in the RYGB and OLGB groups, respectively (Fig. 2).

Effect of bariatric surgery type on serum concentration of total bile acids
Since the post-surgery increase in serum concentration of BAs was postulated to be associated with an improvement of glucose metabolism and insulin sensitivity, we analyzed relationships between relative changes in total BAs, HbA1c, and HOMA at 3 months after the bariatric procedure. Our analysis demonstrated that the postoperative increase in serum BAs was associated with a significant decrease in both HbA1c and HOMA values (Fig. 3).

Correlations between relative changes (delta) in serum concentrations of total bile acids, serum HbA1c, and HOMA determined 3 months after various types of bariatric surgeries
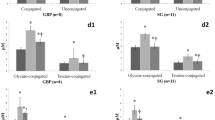
Detailed information about pre- and postoperative profiles of serum BAs in the study patients is presented in Table 2. Three months after OLGB, a particularly evident increase was observed in primary and secondary conjugated BAs, especially GCA, GCDCA, and GDCA (Supplementary Table S2). Also, RYGB contributed to an evident increase in primary conjugated BAs. In turn, LSG resulted in a slight increase in secondary conjugated BAs and a concomitant decrease in primary unconjugated BAs. Regardless of bariatric procedure type, no significant increase in BA concentrations was observed at 4 days post-surgery. In contrast, the treatment contributed to a significant decrease in primary unconjugated BAs (in the OLGB and RYGB groups), secondary unconjugated BAs (in the LSG group), or both primary and secondary conjugated BAs (in the RYGB group).
No bile loop is created during LSG, and the loop created during OLGB is longer than that formed during RYGB; this implies that the length of the bile loop might influence serum concentrations of BAs in our patients at 3 months after the bariatric procedure. Indeed, total concentration of serum BAs 3 months after RYGB and OLGB correlated positively with the length of the bile loop (Fig. 4).

Correlation between the length of bile loop created during RYGB and OLGB and serum concentration of total bile acids determined 3 months after the bariatric procedure. R = 0.47, p < 0.05
Discussion
To the best of our knowledge, our present experiment was the first study to compare the effects of three various bariatric procedures, LSG, RYGB, and OLGB, on serum concentrations of BAs in morbidly obese patients. The results of previous research in this matter were inconclusive. While the majority of recent studies demonstrated that RYGB contributed to a significant increase in serum concentration of bile acids, LSG resulted in either a decrease or increase in serum BAs, or had no effect at all [8]. In turn, the influence of OLGB on serum BAs has not been studied thus far. Our hereby presented findings suggest that OLGB contributed to a more evident increase in serum BAs at 3 months post-surgery than RYGB. Not surprisingly, LSG exerted the least evident effect on postoperative serum BA levels. According to some authors, the post-surgery increase in serum BAs was associated with an improvement of glucose metabolism [15, 21,22,23,24]. Our findings are consistent with those data, since the levels of serum glucose, insulin, HOMA, and HBA1c at 3 months after the bariatric procedure were significantly lower than those prior to the surgery. However, the magnitude of this effect depended on the type of bariatric procedure, with the most prominent changes observed after OLGB and the least evident improvement documented in the LSG group. Also, according to other authors, OLGB contributed to a greater improvement in glucose metabolism than RYGB [25]. Altogether, these findings suggest that the more evident the postoperative increase in serum BAs, the greater the improvement in glucose metabolism and insulin sensitivity. The results of our study support this hypothesis, as we found strong inverse correlations between relative postoperative changes in serum BAs, HbA1c, and HOMA levels.
However, the question arises about a plausible underlying mechanism of these associations. One difference between the three bariatric procedures analyzed in this study is the length of bile loop [7]. While the loop created during OLGB is longer than that formed during RYGB, no bile loop is made during LSG. Since the most evident increase in serum BAs was observed after OLGB, followed by RYGB and LSG, the magnitude of this effect might have been directly related to the length of bile loop created during various bariatric procedures. This hypothesis seems to be supported by a significant positive correlation between bile loop length and serum concentrations of BAs at 3 months after RYGB and OLBG. The differences in postoperative dynamics of serum BAs probably resulted from the fact that bile acids released to the intestinal segment excluded from the alimentary passage did not mix with food and hence might be reabsorbed at higher concentrations [8]. Primary conjugated BAs were the group of bile acids that showed the most evident increase at 3 months after RYGB and OLGB. These BAs are synthesized in the liver and released directly to the intestinal segment which is partially excluded from the alimentary passage during bariatric procedure, which might contribute to their higher reuptake.
Our findings are partially consistent with the results published recently by Risstad et al. [26]; according to these authors, the increase in total serum BAs in obese patients subjected to biliopancreatic diversion with duodenal switch (BPD/DS) was greater than that in individuals after RYGB. Similar to OLGB, BPD/DS also results in a longer passage of concentrated bile via the biliopancreatic limb. Unfortunately, Risstad et al. did not analyze the link between serum concentration of BAs and biliary loop length [26]. The importance of the latter parameter as a determinant of serum BA level after bariatric surgery was also demonstrated in an animal study in which an increase in bile acid concentration and improvement of glucose metabolism were observed in rats with longer biliopancreatic limb, but not in those with the shorter limb [27]. Both our hereby presented findings and the results of previous studies support the conclusion that the length of concentrated bile passage created during a bariatric surgery influences the serum level of BAs in morbidly obese patients.
In general, bariatric surgery leads to reversion or prevents nonalcoholic fatty liver disease (NAFLD). However, recent studies revealed that in some cases, the deterioration of liver parameters and fibrosis may occur after RYGB and OLGB [28, 29]. OLGB results in greater worsening of liver parameters than RYGB [28]. Increased amounts of BA in hepatocytes cause damage of these cells by induction of apoptosis, necrosis, and mitochondrial injury [10]. Moreover, serum BA level increases with increasing liver fibrosis [30]. However, further studies are needed to find out if prominent increase of serum BA concentrations after OLGB may contribute to increased liver fibrosis.
The fact that bariatric treatment, in particular various types of gastric bypass procedures, results in a rapid improvement of insulin sensitivity, observed already a few days after the procedure, raises interest of researchers and clinical practitioners. However, although this phenomenon has been reported by many authors [7, 31,32,33,34,35], its underlying mechanism is still not fully understood. We hypothesized that the rapid improvement of insulin sensitivity observed shortly after bariatric surgery may be associated with BA response. Our hypothesis was driven by the results published by Pournaras et al. [36] who documented an increase in total serum BAs in 12 obese patients as early as 3 days after RYGB. However, the effect observed in their study was not statistically significant and individual results varied considerably. Unlike Pournaras et al., we did not observe an increase in serum BAs during early postoperative period (at 4 days post-surgery), and the serum level of bile acids in the RYGB group was even slightly, albeit significantly, lower than at the baseline. Thus, our findings do not support the role of BAs in the improvement of insulin sensitivity shortly after bariatric surgery. Perhaps this phenomenon can be explained by other mechanisms, e.g., reduced food intake and increased secretion of incretin shortly after the bariatric procedure [20, 32].
Conclusions
Recent evidence suggests that changes in the concentration of circulating BAs may contribute to metabolic improvement observed after bariatric surgeries, but underlying mechanisms of this phenomenon are poorly understood. The evident improvement of glucose metabolism observed in our patients after OLGB might be associated with a significant increase in serum concentrations of bile acids, especially primary conjugated BAs that can be more efficiently absorbed from a longer bile loop. However, the changes in serum BAs probably had little or no impact on insulin sensitivity improvement observed 4 days after the surgery.
References
Redinger RN. The pathophysiology of obesity and its clinical manifestations. Gastroenterol Hepatol. 2007;3:856–63.
Caruso C, Balistreri CR, Candore G. The role of adipose tissue and adipokines in obesity-related inflammatory diseases. Mediat Inflamm. 2010;2010:802078.
Athyros VG, Tziomalos K, Karagiannis A, et al. Cardiovascular benefits of bariatric surgery in morbidly obese patients. Obes Rev. 2011;12:515–24.
Bray GA. Medical consequences of obesity. J Clin Endocrinol Metab. 2004;89:2583–9.
Thaler JP, Cummings DE. Minireview: hormonal and metabolic mechanisms of diabetes remission after gastrointestinal surgery. Endocrinology. 2009;150:2518–25.
Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122:248–56.
Kaska Ł, Proczko M, Wiśniewski P, et al. A prospective evaluation of the influence of three bariatric procedures on insulin resistance improvement. Should the extent of undiluted bile transit be considered a key postoperative factor altering glucose metabolism? Videosurgery Other Miniinvasive Tech. 2015;2:213–28.
Kaska L, Sledzinski T, Chomiczewska A, et al. Improved glucose metabolism following bariatric surgery is associated with increased circulating bile acid concentrations and remodeling of the gut microbiome. World J Gastroenterol. 2016;22:8698–719.
García-Cañaveras JC, Donato MT, Castell JV, et al. Targeted profiling of circulating and hepatic bile acids in human, mouse, and rat using a UPLC-MRM-MS-validated method. J Lipid Res. 2012;53:2231–41.
Palmeira CM, Rolo AP. Mitochondrially-mediated toxicity of bile acids. Toxicology. 2004;203:1–15.
Humbert L, Maubert MA, Wolf C, et al. Bile acid profiling in human biological samples: comparison of extraction procedures and application to normal and cholestatic patients. J Chromatogr B Anal Technol Biomed Life Sci. 2012;899:135–45.
Yang L, Xiong A, He Y, et al. Bile acids metabonomic study on the CCl4- and alpha-naphthylisothiocyanate-induced animal models: quantitative analysis of 22 bile acids by ultraperformance liquid chromatography-mass spectrometry. Chem Res Toxicol. 2008;21:2280–8.
Reddy BS, Watanabe K, Weisburger JH, et al. Promoting effect of bile acids in colon carcinogenesis in germ-free and conventional F344 rats. Cancer Res. 1977;37:3238–42.
Jansen PLM, van Werven J, Aarts E, et al. Alterations of hormonally active fibroblast growth factors after Roux-en-Y gastric bypass surgery. Dig Dis. 2011;29:48–51.
Simonen M, Dali-Youcef N, Kaminska D, et al. Conjugated bile acids associate with altered rates of glucose and lipid oxidation after Roux-en-Y gastric bypass. Obes Surg. 2012;22:1473–80.
Hutch CR, Sandoval DA. Physiological and molecular responses to bariatric surgery: markers or mechanisms underlying T2DM resolution? Ann N Y Acad Sci. 2017;1391:5–19.
Raghow R. Ménage-à-trois of bariatric surgery, bile acids and the gut microbiome. World J Diabetes. 2015;6:367–70.
Watanabe M, Houten SM, Mataki C, et al. Bile acids induce energy expenditure by promoting intracellular thyroid hormone activation. Nature. 2006;439:484–9.
Scholtz S, Miras AD, Chhina N, et al. Obese patients after gastric bypass surgery have lower brain-hedonic responses to food than after gastric banding. Gut. 2014;63:891–902.
Steinert RE, Peterli R, Keller S, et al. Bile acids and gut peptide secretion after bariatric surgery: a 1-year prospective randomized pilot trial. Obesity. 2013;21:E660–8.
Werling M, Vincent RP, Cross GF, et al. Enhanced fasting and post-prandial plasma bile acid responses after Roux-en-Y gastric bypass surgery. Scand J Gastroenterol. 2013;48:1257–64.
Patti M-E, Houten SM, Bianco AC, et al. Serum bile acids are higher in humans with prior gastric bypass: potential contribution to improved glucose and lipid metabolism. Obesity (Silver Spring). 2009;17:1671–7.
Nakatani H, Kasama K, Oshiro T, et al. Serum bile acid along with plasma incretins and serum high-molecular weight adiponectin levels are increased after bariatric surgery. Metabolism. 2009;58:1400–7.
Gerhard GS, Styer AM, Wood GC, et al. A role for fibroblast growth factor 19 and bile acids in diabetes remission after Roux-en-Y gastric bypass. Diabetes Care. 2013;36:1859–64.
Tam MS, Kaoutzanis C, Mullard AJ, et al. A population-based study comparing laparoscopic and robotic outcomes in colorectal surgery. Surg Endosc. 2016;30:455–63.
Risstad H, Kristinsson JA, Fagerland MW, et al. Bile acid profiles over 5 years after gastric bypass and duodenal switch: results from a randomized clinical trial. Surg Obes Relat Dis. 2017;13:1544–53.
Miyachi T, Nagao M, Shibata C, et al. Biliopancreatic limb plays an important role in metabolic improvement after duodenal–jejunal bypass in a rat model of diabetes. Surgery. 2016;159:1360–71.
Kruschitz R, Luger M, Kienbacher C, et al. The effect of Roux-en-Y vs. omega-loop gastric bypass on liver, metabolic parameters, and weight loss. Obes Surg. 2016;26:2204–12.
Eilenberg M, Langer FB, Beer A, et al. Significant liver-related morbidity after bariatric surgery and its reversal—a case series. Obes Surg. 2018;28:812–9.
Jahnel J, Zöhrer E, Alisi A, et al. Serum bile acid levels in children with nonalcoholic fatty liver disease. J Pediatr Gastroenterol Nutr. 2015;61:85–90.
Faria G, Preto J, da Costa EL, et al. Acute improvement in insulin resistance after laparoscopic Roux-en-Y gastric bypass: is 3 days enough to correct insulin metabolism? Obes Surg. 2013;23:103–10.
Laferrère B. Diabetes remission after bariatric surgery: is it just the incretins? Int J Obes. 2011;35(Suppl 3):S22–5.
Cohen RV, Pinheiro JC, Schiavon CA, et al. Effects of gastric bypass surgery in patients with type 2 diabetes and only mild obesity. Diabetes Care. 2012;35:1420–8.
Laferrère B. Do we really know why diabetes remits after gastric bypass surgery? Endocrine. 2011;40:162–7.
Camastra S, Gastaldelli A, Mari A, et al. Early and longer term effects of gastric bypass surgery on tissue-specific insulin sensitivity and beta cell function in morbidly obese patients with and without type 2 diabetes. Diabetologia. 2011;54:2093–102.
Pournaras DJ, Glicksman C, Vincent RP, et al. The role of bile after Roux-en-Y gastric bypass in promoting weight loss and improving glycaemic control. Endocrinology. 2012;153:3613–9.
Acknowledgements
The authors would like to thank Marcin Lipinski and Adrianna Radulska for their technical assistance.
Funding
This study was supported by the Medical University of Gdansk (grant nos. ST40, ST41, and ST89) and by the National Science Centre of Poland (grant no. NCN 2016/21/D/NZ5/00219).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Electronic Supplementary Material
ESM 1
(DOCX 188 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Mika, A., Kaska, L., Proczko-Stepaniak, M. et al. Evidence That the Length of Bile Loop Determines Serum Bile Acid Concentration and Glycemic Control After Bariatric Surgery. OBES SURG 28, 3405–3414 (2018). https://doi.org/10.1007/s11695-018-3314-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-018-3314-9