
Abstract
Background
The use of bariatric surgery to treat diabetes mellitus (DM) requires procedures developed for morbid obese in patients with normal and over-weight. Therefore, we started tailoring one anastomosis gastric bypass (BAGUA) adapted to each patient. This study analyzes changes in body composition (BC) of patients with BMI 23–50 after BAGUA as well as influence of DM and MS.
Methods
We studied 79 (37 diabetic and 42 non-diabetic) patients (BMI 23–50) who completed all evaluation appointment (preoperative, 10 days, 1, 3, 6, and 12 months) after tailored BAGUA for obesity, diabetes, or diabesity. Patients were classified according to BMI (23–29, 30–34, 35–50) and bearing or not diabetes. Variables are components of BC as well as DM and MS.
Results
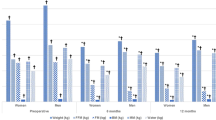
Preoperatively, mean values of weight varied 37 kg (78–115 kg), muscle mass (MM) 8 kg (54–62 kg), while fat mass (FM) 30 kg (22–53 kg). Basal metabolism (BM) was higher in diabetic. After surgery, percentage (%) of excess weight loss (%EWL) ranged from 76 % (BMI 35–50) to 128 % (BMI 23–29), FM 56 % (BMI 23–29) to 65 % (BMI 35–50), without differences bearing DM. MM 12 % (non-diabetics BMI 30–34) to 17 % (diabetics BMI 35–50) and visceral fat (VF) 50 % (diabetics BMI 30–34) to 56 % (non-diabetics BMI 35–50).
Conclusions
After tailored BAGUA, MM maintains steady while FM is highly reduced and variable. BM is reduced in all groups. Diabetics lose less weight and VF but more MM than non-diabetic patients. Preoperative presence of MS influences the changes in BC.

Similar content being viewed by others

Abbreviations
- BAGUA:
-
Bypass Gástrico Una Anastomosis (one anastomosis gastric bypass in Spanish)
- DM:
-
Diabetes mellitus
- BC:
-
Body composition
- MS:
-
Metabolic syndrome
- BMI:
-
Body mass index
- MM:
-
Muscle mass
- FM:
-
Fat mass
- BM:
-
Basal metabolism
- VF:
-
Visceral fat
- FFM:
-
Fat-free mass
- T2DM:
-
Type 2 diabetes mellitus
- TBW:
-
Total water
- Mini GB:
-
Mini gastric bypass
References
Das SK, Roberts SB, McCrory MA, et al. Long-term changes in energy expenditure and body composition after massive weight loss induced by gastric bypass surgery. Am J Clin Nutr. 2003;78(1):22–30.
Levitt DG, Beckman LM, Mager JR, et al. Comparison of DXA and water measurements of body fat following gastric bypass surgery and a physiological model of body water, fat, and muscle composition. J Appl Physiol. 2010;109(3):786–95.
Strain GW, Gagner M, Pomp A, et al. Comparison of weight loss and body composition changes with four surgical procedures. Surg Obes Relat Dis. 2009;5(5):582–7.
Olbers T, Bjorkman S, Lindroos A, et al. Body composition, dietary intake, and energy expenditure after laparoscopic Roux-en-Y gastric bypass and laparoscopic vertical banded gastroplasty: a randomized clinical trial. Ann Surg. 2006;244(5):715–22.
Marks BL, Rippe JM. The importance of fat free mass maintenance in weight loss programmes. Sports Med. 1996;22(5):273–81.
Faria SL, Faria OP, Buffington C, et al. Energy expenditure before and after Roux-en-Y gastric bypass. Obes Surg. 2012;22(9):1450–5.
Werling M, Olbers T, Fandriks L, et al. Increased postprandial energy expenditure may explain superior long term weight loss after Roux-en-Y gastric bypass compared to vertical banded gastroplasty. PLoS One. 2013;8(4):e60280.
Liu X, Lagoy A, Discenza I, et al. Metabolic and neuroendocrine responses to Roux-en-Y gastric bypass. I: energy balance, metabolic changes, and fat loss. J Clin Endocrinol Metab. 2012;97(8):E1440–50.
Blanchard J, Conrad KA, Harrison GG. Comparison of methods for estimating body composition in young and elderly women. J Gerontol. 1990;45(4):B119–24.
Cunningham JJ. Body composition as a determinant of energy expenditure: a synthetic review and a proposed general prediction equation. Am J Clin Nutr. 1991;54(6):963–9.
Campbell WW, Crim MC, Young VR, et al. Increased energy requirements and changes in body composition with resistance training in older adults. Am J Clin Nutr. 1994;60(2):167–75.
Kenney WL, Buskirk ER. Functional consequences of sarcopenia: effects on thermoregulation. J Gerontol A Biol Sci Med Sci. 1995;50:78–85.
Aloia JF, Vaswani A, Ma R, et al. To what extent is bone mass determined by fat-free or fat mass? Am J Clin Nutr. 1995;61(5):1110–4.
Marks BL, Perkins KA. The effects of nicotine on metabolic rate. Sports Med. 1990;10(5):277–85.
Dutta C, Hadley EC. The significance of sarcopenia in old age. J Gerontol A Biol Sci Med Sci. 1995;50:1–4.
Shephard RJ, Bouhlel E, Vandewalle H, et al. Muscle mass as a factor limiting physical work. J Appl Physiol. 1985;64(4):1472–9.
Svendsen OL, Hassager C, Christiansen C. Effect of an energy-restrictive diet, with or without exercise, on lean tissue mass, resting metabolic rate, cardiovascular risk factors, and bone in overweight postmenopausal women. Am J Med. 1993;95(2):131–40.
Ballor DL, Poehlman ET. Exercise-training enhances fat-free mass preservation during diet-induced weight loss: a meta-analytical finding. Int J Obes Relat Metab Disord. 1994;18(1):35–40.
Donnelly JE, Jakicic J, Gunderson S. Diet and body composition. Effect of very low calorie diets and exercise. Sports Med. 1991;12(4):237–49.
Kim MK, Lee HC, Kwon HS, et al. Visceral obesity is a negative predictor of remission of diabetes 1 year after bariatric surgery. Obesity. 2011;19(9):1835–9.
Scopinaro N, Adami GF, Papadia FS, et al. Effects of biliopanceratic diversion on type 2 diabetes in patients with BMI 25 to 35. Ann Surg. 2011;253(4):699–703.
Garciacaballero M, Valle M, Martinez-Moreno JM, et al. Resolution of diabetes mellitus and metabolic syndrome in normal weight 24-29 BMI patients with One Anastomosis Gastric Bypass. Nutr Hosp. 2012;27(2):623–31.
Garciacaballero M, Martinez-Moreno JM, Toval JA, et al. Improvement of C peptide zero BMI 24-34 diabetic patients after tailored one anastomosis gastric bypass (BAGUA). Nutr Hosp. 2013;28 Suppl 2:35–46.
Sauerland S, Angrisani L, Belachew M, et al. Obesity surgery: evidence-based guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc. 2005;19(2):200–21.
Lee WJ, Wang W, Lee YC, et al. Laparoscopic mini-gastric bypass: experience with tailored bypass limb according to body weight. Obes Surg. 2008;18(3):294–9.
Lee WJ, Wang W, Lee YC, et al. Effect of laparoscopic mini-gastric bypass for type 2 diabetes mellitus: comparison of BMI > 35 and <35 kg/m2. J Gastrointest Surg. 2008;12(5):945–52.
Savastano S, Di Somma C, Angrisani L, et al. Growth hormone treatment prevents loss of lean mass after bariatric surgery in morbidly obese patients: results of a pilot, open, prospective, randomized, controlled study. J Clin Endocrinol Metab. 2009;94(3):817–26.
American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;36 Suppl 1:S67–74.
Acknowledgments
We acknowledge every author who collaborates in the paper.
Grant information
Each author gave grants.
Conflict of Interest
M. Garciacaballero: no conflict of interest.
A. Reyes-Ortiz: no conflict of interest.
M. García: no conflict of interest.
J.A. Toval: no conflict of interest.
J. M. Martínez-Moreno: no conflict of interest.
A. García: no conflict of interest.
A. Mínguez: no conflict of interest.
D. Osorio: no conflict of interest.
J.M. Mata: no conflict of interest.
F. Miralles: no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Garciacaballero, M., Reyes-Ortiz, A., García, M. et al. Changes of Body Composition in Patients with BMI 23–50 After Tailored One Anastomosis Gastric Bypass (BAGUA): Influence of Diabetes and Metabolic Syndrome. OBES SURG 24, 2040–2047 (2014). https://doi.org/10.1007/s11695-014-1288-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-014-1288-9