
Abstract
Background
The optimal size of bougie in laparoscopic sleeve gastrectomy (LSG) remains controversial. The aim of this study was to evaluate the first-year outcome of LSG using two different sizes of bougies.
Methods
This study used a single institute retrospective case-control study of two groups of patients. Group A (N = 66) underwent LSG using 42-Fr and group B (N = 54) using 32-Fr bougies. A medication score was applied to assess the change in comorbid conditions.
Results
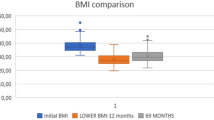
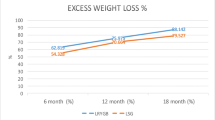
Groups A and B's age (39.5 ± 12 vs. 43.6 ± 12.3 years), weight (119 ± 17 vs. 120 ± 20), and BMI (42.8 ± 3.8 vs. 43.6 ± 6.9 kg/m2), respectively, were comparable (p = NS). Comorbid conditions were type 2 diabetes (T2DM) in 19 (29 %) vs. 23 (43 %) patients, hypertension in 22 (33 %) vs. 18 (33 %) patients, and gastroesophageal reflux (GERD) in 28 (42 %) vs. 10 (19 %) patients, respectively. At 1 year, group A vs. B BMI was (29.4 ± 5 vs. 30 ± 5 kg/m2) and excess weight loss was 67 vs. 65 %, respectively (p = NS). Postoperatively, T2DM (79 vs. 83 %), hypertension (82 vs. 61 %), and GERD (82 vs. 60 %) (p = NS), respectively, in groups A vs. B did not require previous medications anymore. Complications were comparable.
Conclusions
Our data suggest that using a 42-Fr or 32-Fr bougie does not influence LSG first-year weight loss or resolution of comorbid conditions. Long-term data is needed to conclude this issue.

Similar content being viewed by others

References
Rosenthal RJ et al. International Sleeve Gastrectomy. Expert Panel Consensus Statement: best practice guidelines based on experience of >12,000 cases. Surg Obes Relat Dis. 2012;8(1):8–19.
Atkins ER, Preen DB, Jarman C, et al. Improved obesity reduction and co-morbidity resolution in patients treated with 40-French bougie versus 50-French bougie four years after laparoscopic sleeve gastrectomy. Analysis of 294 patients. Obes Surg. 2012;22(1):97–104.
Yuval JB, Mintz Y, Cohen MJ, et al. The effects of bougie caliber on leaks and excess weight loss following laparoscopic sleeve gastrectomy. Is there an ideal bougie size? Obes Surg. 2013;23(10):1685–91.
Lazzati A, Guy-Lachuer R, Delaunay V et al. Bariatric surgery trends in France: 2005-2011. Surg Obes Relat Dis. 2013;S1550–7289(13):00253–0. doi:10.1016/j.soard.2013.07.015.
Parikh M, Issa R, McCrillis A, et al. Surgical strategies that may decrease leak after laparoscopic sleeve gastrectomy: a systematic review and meta-analysis of 9991 cases. Ann Surg. 2013;257(2):231–7.
Schauer PR, Kashyap SR, Wolski K, et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Engl J Med. 2012;366(17):1567–76.
Peterli R, Borbély Y, Kern B, et al. Early results of the Swiss Multicentre Bypass or Sleeve Study (SM-BOSS): a prospective randomized trial comparing laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass. Ann Surg. 2013;258(5):690–5.
Conflict of Interest
Hadar Spivak, Mosh Rubin, Eran Sadot, Esther Pollack, Anya Feigin, and David Goitein have no conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Spivak, H., Rubin, M., Sadot, E. et al. Laparoscopic Sleeve Gastrectomy Using 42-French Versus 32-French Bougie: The First-Year Outcome. OBES SURG 24, 1090–1093 (2014). https://doi.org/10.1007/s11695-014-1199-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-014-1199-9