
Abstract
Introduction
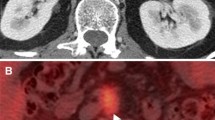
Pancreatic cancer recurrence is often difficult to detect by conventional imaging. Our aim was to evaluate the impact of fluorodeoxyglucose-positron emission tomography (FDG-PET) in the diagnosis of recurrent pancreatic cancer.
Methods
One-hundred thirty-eight patients were followed after resection for pancreatic cancer. Sixty-six underwent only CT and were excluded. Seventy-two patients also had FDG-PET. Recurrent patients were divided in two groups: group-1, CT positive and group 2, CT non diagnostic, FDG-PET positive. Characteristics and survival curves of the two groups were compared. Significance was set at p < 0.05.
Results
Overall, tumors recurred in 63 of 72 (87.5%) patients; two patients had a second cancer resected, thanks to FDG-PET. Tumor relapse was detected by CT in 35 patients and by FDG-PET in 61. Prognostic factors were similar in groups 1 and 2. Five out of 35 group 1 patients underwent surgery (two R0, two bypass, and one exploratory). Ten out of 28 group 2 patients underwent surgery (four R0, two R2, two bypass, and two exploratory). FDG-PET influenced treatment strategies in 32 of 72 patients (44.4%). Group 2 patients survived longer (P = 0.09), but the difference was not significant. Disease-free survival was similar in groups 1 and 2.
Conclusion
Tumor relapse is detected earlier by FDG-PET than by CT. FDG-PET can help select the best candidates for surgical exploration, although the real benefit is still to be defined. It influences treatment strategies in a significant percentage of patients. An earlier diagnosis did not influence survival due to the lack of effective therapies.





Similar content being viewed by others


References
Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics 2009. CA Cancer J Clin 2009;59:225–249.
Bilimoria KY, Bentrem DJ, Ko CY, Tomlinson JS, Stewart AK, Winchester DP, Talamonti MS. Multimodality therapy for pancreatic cancer in the U.S.. Cancer 2007;110:1227–1234.
Ferrone CR, Brennan MF, Gonen M, Coit DG, Fong Y, Chung S, Tang L, Klimstra D, Allen PJ. Pancreatic adenocarcinoma: the actual 5-year survivors. J Gastrointest Surg 2008;12:701–706.
Schnelldorfer T, Ware AL, Sarr MG, Smyrk TC, Zhang L, Qin R, Gullerud RE, Donohue JH, Nagorney DM, Farnell MB. Long-term survival after pancreatoduodenectomy for pancreatic adenocarcinoma. Is cure possible? Ann Surg 2008;247:456–462.
Sperti C, Pasquali C, Piccoli A, Pedrazzoli S. Recurrence after resection for ductal adenocarcinoma of the pancreas. World J Surg 1997;21:195–200.
Kim JK, Ha HK, Han DJ, Auh YH. CT analysis of postoperative tumor recurrence patterns in periampullary cancer. Abdom Imaging 2003;28:384–391.
Shimada K, Sakamoto Y, Sano T, Kosuge T. The Role of paraaortic lymph node involvement on early recurrence and survival after macroscopic curative resection with extended lymphadenectomy for pancreatic carcinoma. J Am Coll Surg 2006;203:345–352.
Park JS, Yoon DS, Kim KS, Choi JS, Lee WJ, Chi HS, Kim BR. Factors influencing recurrence after curative resection for ampulla of Vater carcinoma. J Surg Oncol 2007;95:286–290.
Raut CP, Tseng JF, Sun CC, Wang H, Wolff RA, Crane CH, Hwang R, Vauthey JN, Abdalla EK, Lee JE, Pisters PWT, Evans DB. Impact of resection status on pattern of failure and survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. Ann Surg 2007;246:52–60.
Kinsella TJ, Seo Y, Willis J, Stellato TA, Siegel CT, Harpp D, Willson JK, Gibbons J, Sanabria JR, Hardacre JM, Schulak JP. The impact of resection margin status and postoperative Ca19–9 levels on survival and pattern of recurrence after postoperative high-dose radiotherapy with 5-F-U-based concurrent chemotherapy for resectable pancreatic cancer. Am J Clin Oncol 2008;31:446–453.
Van den broeck A, Sergeant G, Ectors N, Van Steenbergen W, Aerts R, Topal B. Patterns of recurrence after curative resection of pancreatic ductal adenocarcinoma. Eur J Surg Oncol 2009;35:600–604. doi:10.1016/j.ejso.2008.12.006.
Menke-Pluymers MB, Klinkenbijl JHG, Tjioe M, Jeekel J. Treatment of locoregional recurrence after intentional curative resection of pancreatic cancer. Hepatogastroenterology 1992;39:429–432.
Westerdahl J, Andrén-Sandberg A, Ihse I. Recurrence of exocrine pancreatic cancer—local or hepatic? Hepatogastroenterology 1993;40:384–387.
Sunamura M, Egawa S, Shibuya K, Shimamura H, Takeda K, Kobari M, Matsuno S. Therapeutic strategy for the recurrence of pancreatic cancer following pancreatectomy. Nippon Geka Gakkai Zasshi 1999;100:200–205.
Tamm EP, Silverman PM, Charnsangavej C, Evans DB. Diagnosis, staging, and surveillance of pancreatic cancer. AJR 2003;180:1311–1320.
Ishigami K, Yoshimitsu K, Irie H, Tajima T, Asayama Y, Hirakawa M, Kakihara D, Shioyama Y, Nishihara Y, Yamaguchi K, Honda H. Significance of mesenteric lymphadenopathy after pancreaticoduodenectomy for periampullary carcinomas: evaluation with serial MDCT studies. Eur J Radiol 2007;61:491–498.
Wilkowski R, Thoma M, Bruns C, Dühmke E, Heinemann V. Combined chemoradiotherapy for isolated local recurrence after primary resection of pancreatic cancer. JOP 2006;7:34–40.
Horiuchi H, Uchida S, Hisaka T, Ishikawa H, Sakai T, Kawahara R, Kinoshita H, Shirouzu K. A study of recurrent pancreatic cancer with metastatic liver tumors after pancreatectomy. Gan To Kagaku Ryoho 2005;32:1685–1687.
Inoue K, Kosuge T, Shimada K, Yamamoto J, Takayama T, Ozaki H, Nose H. Repeated radical resection and intraoperative irradiation for recurrent pancreatic ductal adenocarcinoma after pancreatoduodenectomy. Surgery 1995;118:909–911.
Ibusuki M, Hiraoka T, Kanemitsu K, Takamori H, Tsuji T. Complete remission of pancreatic cancer after multiple resections of locally pancreatic recurrent sites and liver metastasis: report of a case. Surg Today 2008;38:563–566.
Nakano H, Asakura T, Koizumi S, Asano T, Watanabe T, Otsubo T, Takizawa K. Second surgery after a pancreaticoduodenectomy in patients with periampullary malignancies. Hepatogastroenterology 2008;55:687–691.
Kleeff J, Reiser C, Hinz U, Bachmann J, Debus J, Jaeger D, Friess H, Büchler MW. Surgery for recurrent pancreatic ductal adenocarcinoma. Ann Surg 2007;245:566–572.
Rose DM, Delbeke D, Beauchamp D, Chapman WC, Sandler MP, Sharp KW, Richards WO, Wright JK, Frexes ME, Pinson CW, Leach SD. 18-Fluorodeoxyglucose positron emission tomography in the management of suspected pancreatic cancer. Ann Surg 1998;229:729–738.
Franke C, Klapdor R, Meyerhoff K, Schauman M. 18-FDG positron emission tomography of the pancreas: diagnostic benefit in the follow-up of pancreatic carcinoma. Anticancer Res 1999;19:2437–2442.
Jadvar H, Fischman AJ. Evaluation of pancreatic carcinoma with FDG PET. Abdom Imaging 2001;26:254–259.
Ruf J, Lopez Hänninen E, Oettle H, Plotkin M, Pelzer U, Stroszczynski C, Felix R, Amthauer H. Detection of recurrent pancreatic cancer: comparison of FDG-PET with CT/MRI. Pancreatology 2005;5:266–272.
Pedrazzoli S, Beger HG, Obertop H, Andrén-Sandberg A, Fernández-Cruz L, Henne-Bruns D, Lüttges J, Neoptolemos JP. A surgical and pathological based classification of resective treatment of pancreatic cancer. Summary of an international workshop on surgical procedures in pancreatic cancer. Dig Surg 1999;16:337–345.
Sobin LH, Wittekind C. UICC: TNM classification of malignant tumors. 6th ed. New York: Wiley, 2002.
Sperti C, Bissoli S, Pasquali C, Frison L, Liessi G, Chierichetti F, Pedrazzoli S. 18-Fluorodeoxyglucose positron emission tomography enhances computed tomography diagnosis of malignant intraductal papillary mucinous neoplasms of the pancreas. Ann Surg 2007;246:932–939.
Sperti C, Pasquali C, Chierichetti F, Ferronato A, Decet G, Pedrazzoli S. 18-Fluorodeoxyglucose positron emission tomography in predicting survival of patients with pancreatic carcinoma. J Gastrointest Surg 2003;7:953–960.
Wakabayashi H, Nishiyama Y, Otani T, Sano T, Yachida S, Okano K, Izuishi K, Suzuki Y. Role of 18F-fluorodeoxyglucose positron emission tomography imaging in surgery for pancreatic cancer. World J Gastroenterol 2008;14:64–69.
Jeong JH, Jung SH, Costantino JP. Nonparametric inference of median residual life function. Biometrics 2008;64:157–163.
Verslype C, Van Cutsem E, Dicato M, Cascinu S, Cunningham D, Diaz-Rubio E, Glimelius B, Haller D, Haustermans K, Heinemann V, Hoff P, Johnston PG, Kerr D, Labianca R, Louvet C, Minsky B, Moore M, Nordlinger B, Pedrazzoli S, Roth A, Rothenberg M, Rougier P, Schmoll HJ, Tabernero J, Tempero M, van de Velde C, Van Laethem JL, Zalcberg J. The management of pancreatic cancer. Current expert opinion and recommendations derived from the 8th World Congress on Gastrointestinal Cancer, Barcelona, 2006. Ann Oncol 2007;18(S7):vii1–vii10.
Israel O, Kuten A. Early detection of cancer recurrence: 18F-FDG PET/CT can make a difference in diagnosis and patient care. J Nucl Med 2007;48:28S–35S.
Sobhani I, Tiret E, Lebtahi R, Aparicio T, Itti E, Montravers F, Vaylet C, Rougier P, André T, Gornet JM, Cherqui D, Delbaldo C, Panis Y, Talbot JN, Meignan M, Le Guludec D. Early detection of recurrence by 18FDG-PET in the follow-up of patients with colorectal cancer. Br J Cancer 2008;98:875–880.
Sun L, Su XH, Guan YS, Pan WM, Luo ZM, Wei JH, Wu H. Clinical role of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in post-operative follow-up of gastric cancer: initial results. World J Gastroenterol 2008;14:4627–4632.
Casneuf V, Delrue L, Kelles A, Van Damme N, Van Huysse J, Berrevoet F, De Vos M, Duyck P, Peeters M. Is combined 18F-fluorodeoxyglucose-positron emission tomography/computed tomography superior to positron emission tomography or computed tomography alone for diagnosis, staging and restaging of pancreatic lesions? Acta Gastroenterol Belg 2007;70:331–338.
Hillner BE, Siegel BA, Liu D, Shields AF, Gareen IF, Hanna L, Stine SH, Coleman RE. Impact of positron emission tomography/computed tomography and positron emission tomography (PET) alone in expected management of patients with cancer: initial results from the National Oncologic PET Registry. J Clin Oncology 2008;26:2155–2161.
Acknowledgement
The authors gratefully acknowledge Mario Gruppo for the statistical analysis, Tania Lazzarin for helping with the manuscript, and Simona Callegari for helping with data collection. This study was supported in part by grants from the Italian Ministry for the University, Scientific and Technological Research (MURST), project 2005060715_001.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sperti, C., Pasquali, C., Bissoli, S. et al. Tumor Relapse after Pancreatic Cancer Resection is Detected Earlier by 18-FDG PET than by CT. J Gastrointest Surg 14, 131–140 (2010). https://doi.org/10.1007/s11605-009-1010-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-009-1010-8