
Abstract
Purpose
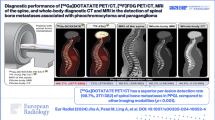
The roles of different cross-sectional imaging in evaluating the recurrence of pancreatic adenocarcinoma are not well established. We evaluated the utility of 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) and contrast-enhanced computed tomography (CECT) in the diagnosis of recurrent pancreatic adenocarcinoma in conjunction with the tumor marker CA 19-9.
Methods
We retrospectively reviewed the records of patients who underwent CECT and FDG PET/CT along with serum CA 19-9 measurement as a follow-up or on a clinical suspicion of recurrent disease after initial surgery for pancreatic adenocarcinoma. Two observers blinded to the other imaging modality results retrospectively reviewed and interpreted the images in consensus using a three-point scale (negative, equivocal, or positive). Pathologic analysis by biopsy or further clinical and radiologic follow-up determined the true status of the suspected recurrences. The imaging results were compared with CA 19-9 levels and true disease status.
Results
Thirty-nine patients were included in the study. Thirty-three patients (85%) had proven recurrent cancer and six patients (15%) had no evidence of disease. Twenty-four patients had elevated CA 19-9 and 15 patients had normal CA 19-9. Sensitivity, specificity, and accuracy for recurrence were 90.9%, 100.0%, and 92.3% for PET/CT and 72.2%, 66.6%, and 71.7% for CECT, respectively. Sensitivity for locoregional recurrence was 94.4% for PET/CT but only 61.1% for CECT. PET/CT detected recurrence in 12 patients who had normal levels of CA 19-9. PET/CT showed lesions not visible on CECT in five (15%) patients. Although the sensitivity and specificity of PET/CT were higher than those of CECT, they were not statistically significant (p = 0.489 and p = 0.1489, respectively).
Conclusion
FDG PET/CT has a high sensitivity for pancreatic cancer recurrence. Normal CA 19-9 does not necessarily exclude these recurrences. FDG PET/CT is useful when CECT is equivocal and can detect recurrence in patients with normal CA 19-9.




Similar content being viewed by others


References
Jemal A, Siegel R, Xu J, Ward E (2010) Cancer statistics, 2010. CA 60:277–300
Barugola G, Falconi M, Bettini R, et al. (2007) The determinant factors of recurrence following resection for ductal pancreatic cancer. JOP 8:132–140
Sperti C, Pasquali C, Piccoli A, Pedrazzoli S (1997) Recurrence after resection for ductal adenocarcinoma of the pancreas. World J Surg 21:195–200
Kim JK, Ha HK, Han DJ, Auh YH (2003) CT analysis of postoperative tumor recurrence patterns in periampullary cancer. Abdom Imaging 28:384–391
Strobel O, Hartwig W, Hackert T, et al. (2013) Re-resection for isolated local recurrence of pancreatic cancer is feasible, safe, and associated with encouraging survival. Ann Surg Oncol 20:964–972
Miyazaki M, Yoshitomi H, Shimizu H, et al. (2014) Repeat pancreatectomy for pancreatic ductal cancer recurrence in the remnant pancreas after initial pancreatectomy: is it worthwhile? Surgery 155:58–66
Thomas RM, Truty MJ, Nogueras-Gonzalez GM, et al. (2012) Selective reoperation for locally recurrent or metastatic pancreatic ductal adenocarcinoma following primary pancreatic resection. J Gastrointest Surg 16:1696–1704
Wilkowski R, Thoma M, Bruns C, Duhmke E, Heinemann V (2006) Combined chemoradiotherapy for isolated local recurrence after primary resection of pancreatic cancer. JOP 7:34–40
Habermehl D, Brecht IC, Bergmann F, et al. (2013) Chemoradiation in patients with isolated recurrent pancreatic cancer—therapeutical efficacy and probability of re-resection. Radiat Oncol 8:27
Horiuchi H, Uchida S, Hisaka T, et al. (2005) A study of recurrent pancreatic cancer with metastatic liver tumors after pancreatectomy. Gan to kagaku ryoho. Cancer Chemother 32:1685–1687
Safi F, Roscher R, Beger HG (1989) Tumor markers in pancreatic cancer. Sensitivity and specificity of CA 19-9. Hepatogastroenterology 36:419–423
Park JK, Paik WH, Ryu JK, et al. (2013) Clinical significance and revisiting the meaning of CA 19-9 blood level before and after the treatment of pancreatic ductal adenocarcinoma: analysis of 1,446 patients from the pancreatic cancer cohort in a single institution. PLoS ONE 8:e78977
Kitajima K, Suzuki K, Nakamoto Y, et al. (2010) Low-dose non-enhanced CT versus full-dose contrast-enhanced CT in integrated PET/CT studies for the diagnosis of uterine cancer recurrence. Eur J Nucl Med Mol Imaging 37:1490–1498
Frohlich A, Diederichs CG, Staib L, et al. (1999) Detection of liver metastases from pancreatic cancer using FDG PET. J Nucl Med 40:250–255
Montgomery RC, Hoffman JP, Riley LB, et al. (1997) Prediction of recurrence and survival by post-resection CA 19-9 values in patients with adenocarcinoma of the pancreas. Ann Surg Oncol 4:551–556
Bertino G, Ardiri AM, Calvagno GS, et al. (2013) Carbohydrate 19.9 antigen serum levels in liver disease. BioMed Res Int 2013:531640
Maestranzi S, Przemioslo R, Mitchell H, Sherwood RA (1998) The effect of benign and malignant liver disease on the tumour markers CA19-9 and CEA. Ann Clin Biochem 35(Pt 1):99–103
Parra JL, Kaplan S, Barkin JS (2005) Elevated CA 19-9 caused by Hashimoto’s thyroiditis: review of the benign causes of increased CA 19-9 level. Dig Dis Sci 50:694–695
Osswald BR, Klee FE, Wysocki S (1993) The reliability of highly elevated CA 19-9 levels. Dis Mark 11:275–278
Kannagi R (2007) Carbohydrate antigen sialyl Lewis a—its pathophysiological significance and induction mechanism in cancer progression. Chang Gung Med J 30:189–209
Lamerz R (1999) Role of tumour markers, cytogenetics. Ann Oncol 10(Suppl 4):145–149
Malesci A, Tommasini MA, Bonato C, et al. (1987) Determination of CA 19-9 antigen in serum and pancreatic juice for differential diagnosis of pancreatic adenocarcinoma from chronic pancreatitis. Gastroenterology 92:60–67
Locker GY, Hamilton S, Harris J, et al. (2006) ASCO 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer. J Clin Oncol 24:5313–5327
Tian F, Appert HE, Myles J, Howard JM (1992) Prognostic value of serum CA 19-9 levels in pancreatic adenocarcinoma. Ann Surg 215:350–355
Tong Y, Song Z, Zhu W (2013) Study of an elevated carbohydrate antigen 19-9 concentration in a large health check-up cohort in China. Clin Chem Lab Med 51:1459–1466
Waanders E, van Keimpema L, Brouwer JT, et al. (2009) Carbohydrate antigen 19-9 is extremely elevated in polycystic liver disease. Liver Int 29:1389–1395
Ozkan E, Soydal C, Araz M, Kir KM, Ibis E (2012) The role of 18F-FDG PET/CT in detecting colorectal cancer recurrence in patients with elevated CEA levels. Nucl Med Commun 33:395–402
Gade M, Kubik M, Fisker RV, Thorlacius-Ussing O, Petersen LJ (2015) Diagnostic value of (18)F-FDG PET/CT as first choice in the detection of recurrent colorectal cancer due to rising CEA. Cancer Imaging 15:11
Bhosale P, Peungjesada S, Wei W, et al. (2010) Clinical utility of positron emission tomography/computed tomography in the evaluation of suspected recurrent ovarian cancer in the setting of normal CA-125 levels. Int J Gynecol Cancer 20:936–944
Casneuf V, Delrue L, Kelles A, et al. (2007) Is combined 18F-fluorodeoxyglucose-positron emission tomography/computed tomography superior to positron emission tomography or computed tomography alone for diagnosis, staging and restaging of pancreatic lesions? Acta Gastroenterol Belg 70:331–338
Sperti C, Pasquali C, Bissoli S, et al. (2010) Tumor relapse after pancreatic cancer resection is detected earlier by 18-FDG PET than by CT. J Gastrointest Surg 14:131–140
Heye T, Zausig N, Klauss M, et al. (2011) CT diagnosis of recurrence after pancreatic cancer: is there a pattern? World J Gastroenterol 17:1126–1134
Hishinuma S, Ogata Y, Tomikawa M, et al. (2006) Patterns of recurrence after curative resection of pancreatic cancer, based on autopsy findings. J Gastrointest Surg 10:511–518
Ruf J, Hanninen EL, Oettle H, et al. (2005) Detection of recurrent pancreatic cancer: comparison of FDG-PET with CT/MRI. Pancreatology 5:266–272
Kitajima K, Murakami K, Yamasaki E, et al. (2010) Performance of integrated FDG-PET/contrast-enhanced CT in the diagnosis of recurrent pancreatic cancer: comparison with integrated FDG-PET/non-contrast-enhanced CT and enhanced CT. Mol Imaging Biol 12:452–459
Menke-Pluymers MB, Klinkenbijl JH, Tjioe M, Jeekel J (1992) Treatment of locoregional recurrence after intentional curative resection of pancreatic cancer. Hepato Gastroenterol 39:429–432
Acknowledgments
The University of Texas is supported in part by the National Institutes of Health through Cancer Center Support Grant P30CA016672.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
Institutional review board authorization was obtained.
Informed consent
Since this is a retrospective study, no informed consent was obtained.
Research involving animal and human rights
No animals were harmed during the study as these were human subjects.
Rights and permissions
About this article

Cite this article
Rayamajhi, S., Balachandran, A., Katz, M. et al. Utility of (18) F-FDG PET/CT and CECT in conjunction with serum CA 19-9 for detecting recurrent pancreatic adenocarcinoma. Abdom Radiol 43, 505–513 (2018). https://doi.org/10.1007/s00261-017-1316-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-017-1316-z