
Abstract
Purpose
The estimated annual incidence of pulmonary embolism (PE) is between 69 to 205 cases per 100,000 persons-years. New imaging studies have been developed during the past decade. Chest CTPA, especially multidetector CT, has proven to be superior or equal to PA angiography, even detecting smaller filling defects. We reviewed the differences in opinion to the diagnosis of PE between chest radiologists (CR) who interpret CTPA and interventional radiologists (IR) who perform PA angiography and what they consider the “gold standard” for the diagnosis of PE.
Methods
Two surveys were designed, one for chest radiologists and one for interventional radiologists. An e-mail survey was sent to the members of the Society of Thoracic Radiology and the Society of Interventional Radiologists.
Results
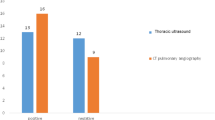
IR with < 10 years since finishing training were less likely to consider CTPA the gold standard, OR 0.45 (0.2–0.9). CR with < 10 years since finishing training were more likely to consider CTPA the gold standard, OR 2.0 (1.1–3.9). Most IR performed < 5 PA angiographies in the last 2 years (69%). CR considered CTPA the gold standard for the diagnosis of PE, OR 3.3 (1.8–6.1). Binary logistic regression analysis for both groups demonstrated that the only variable associated with CTPA as gold standard for the diagnosis of PE was being a chest radiologist.
Conclusion
The majority of the radiologists surveyed indicated that CTPA is the new reference standard for the diagnosis of pulmonary embolism. We agree with this statement based on the evidence available at this time.
Similar content being viewed by others


References
Silverstein MD, Heit JA, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ 3rd (1998) Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med 158(6): 585–593
White RH (2003) The epidemiology of venous thromboembolism. Circulation 107(23 Suppl 1): I4–8. doi:10.1161/01.CIR.0000078468.11849.66107/23_suppl_1/I-4
Dalen JE, Alpert JS (1975) Natural history of pulmonary embolism. Prog Cardiovasc Dis 17(4): 259–270
Silverstein MD, Jea H (1998) Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med 158: 585–593
Carson JL, Kelley MA, Duff A, Weg JG, Fulkerson WJ, Palevsky HI, Schwartz JS, Thompson BT, Popovich J Jr, Hobbins TE et al (1992) The clinical course of pulmonary embolism. N Engl J Med 326(19): 1240–1245
Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (pioped).The pioped investigators (1990). JAMA 263(20):2753–2759
Knottnerus JA, van Weel C, Muris JW (2002) Evaluation of diagnostic procedures. BMJ 324(7335): 477–480
Mills SR, Jackson DC, Older RA, Heaston DK, Moore AV (1980) The incidence, etiologies, and avoidance of complications of pulmonary angiography in a large series. Radiology 136(2): 295–299
Stein PD, Athanasoulis C, Alavi A, Greenspan RH, Hales CA, Saltzman HA, Vreim CE, Terrin ML, Weg JG (1992) Complications and validity of pulmonary angiography in acute pulmonary embolism. Circulation 85(2): 462–468
Qanadli SD, Hajjam ME, Mesurolle B, Barre O, Bruckert F, Joseph T, Mignon F, Vieillard-Baron A, Dubourg O, Lacombe P (2000) Pulmonary embolism detection: prospective evaluation of dual-section helical ct versus selective pulmonary arteriography in 157 patients. Radiology 217(2): 447–455
Winer-Muram HT, Rydberg J, Johnson MS, Tarver RD, Williams MD, Shah H, Namyslowski J, Conces D, Jennings SG, Ying J, Trerotola SO, Kopecky KK (2004) Suspected acute pulmonary embolism: evaluation with multi-detector row ct versus digital subtraction pulmonary arteriography. Radiology 233(3): 806–815
Remy-Jardin M, Remy J, Deschildre F, Artaud D, Beregi JP, Hossein-Foucher C, Marchandise X, Duhamel A (1996) Diagnosis of pulmonary embolism with spiral ct: comparison with pulmonary angiography and scintigraphy. Radiology 200(3): 699–706
Raptopoulos V, Boiselle PM (2001) Multi-detector row spiral ct pulmonary angiography: comparison with single-detector row spiral ct. Radiology 221(3): 606–613
Baile EM, King GG, Muller NL, D’Yachkova Y, Coche EE, Pare PD, Mayo JR (2000) Spiral computed tomography is comparable to angiography for the diagnosis of pulmonary embolism. Am J Respir Crit Care Med 161(3 Pt 1): 1010–1015
Schoepf UJ, Holzknecht N, Helmberger TK, Crispin A, Hong C, Becker CR, Reiser MF (2002) Subsegmental pulmonary emboli: improved detection with thin-collimation multi-detector row spiral ct. Radiology 222(2): 483–490
van Strijen MJ, de Monye W, Schiereck J, Kieft GJ, Prins MH, Huisman MV, Pattynama PM (2003) Single-detector helical computed tomography as the primary diagnostic test in suspected pulmonary embolism: a multicenter clinical management study of 510 patients. Ann Intern Med 138(4): 307–314
de Monye W, van Strijen MJ, Huisman MV, Kieft GJ, Pattynama PM (2000) Suspected pulmonary embolism: prevalence and anatomic distribution in 487 consecutive patients. Advances in new technologies evaluating the localisation of pulmonary embolism (antelope) group. Radiology 215(1): 184–188
Coche E, Vynckier S, Octave-Prignot M (2006) Pulmonary embolism: radiation dose with multi-detector row ct and digital angiography for diagnosis. Radiology 240(3): 690–697
Richman PB, Courtney DM, Friese J, Matthews J, Field A, Petri R, Kline JA (2004) Prevalence and significance of nonthromboembolic findings on chest computed tomography angiography performed to rule out pulmonary embolism: a multicenter study of 1,025 emergency department patients. Acad Emerg Med 11(6): 642–647
Mettler FA Jr, Bhargavan M, Thomadsen BR, Gilley DB, Lipoti JA, Mahesh M, McCrohan J, Yoshizumi TT (2008) Nuclear medicine exposure in the united states, 2005-2007: preliminary results. Semin Nucl Med 38(5): 384–391. doi:S0001-2998(08)00071-8[pii]10.1053/j.semnuclmed.2008.05.004
Groves AM, Yates SJ, Win T, Kayani I, Gallagher FA, Syed R, Bomanji J, Ell PJ (2006) Ct pulmonary angiography versus ventilation-perfusion scintigraphy in pregnancy: implications from a uk survey of doctors’ knowledge of radiation exposure. Radiology 240(3): 765–770. doi:240/3/765[pii]10.1148/radiol.2403050910
Sodickson A, Baeyens PF, Andriole KP, Prevedello LM, Nawfel RD, Hanson R, Khorasani R (2009) Recurrent ct, cumulative radiation exposure, and associated radiation-induced cancer risks from ct of adults. Radiology 251(1): 175–184. doi:251/1/175[pii]10.1148/radiol.2511081296
Remy-Jardin M, Remy J, Wattinne L, Giraud F (1992) Central pulmonary thromboembolism: diagnosis with spiral volumetric ct with the single-breath-hold technique–comparison with pulmonary angiography. Radiology 185(2): 381–387
Goodman LR, Curtin JJ, Mewissen MW, Foley WD, Lipchik RJ, Crain MR, Sagar KB, Collier BD (1995) Detection of pulmonary embolism in patients with unresolved clinical and scintigraphic diagnosis: helical ct versus angiography. AJR 164(6): 1369–1374
Stein PD, Fowler SE, Goodman LR, Gottschalk A, Hales CA, Hull RD, Leeper KV Jr, Popovich J Jr, Quinn DA, Sos TA, Sostman HD, Tapson VF, Wakefield TW, Weg JG, Woodard PK (2006) Multidetector computed tomography for acute pulmonary embolism. N Engl J Med 354(22): 2317–2327
Tillie-Leblond I, Mastora I, Radenne F, Paillard S, Tonnel AB, Remy J, Remy-Jardin M (2002) Risk of pulmonary embolism after a negative spiral ct angiogram in patients with pulmonary disease: 1-year clinical follow-up study. Radiology 223(2): 461–467
Donato AA, Scheirer JJ, Atwell MS, Gramp J, Duszak R Jr (2003) Clinical outcomes in patients with suspected acute pulmonary embolism and negative helical computed tomographic results in whom anticoagulation was withheld. Arch Intern Med 163(17): 2033–2038
Krestan CR, Klein N, Fleischmann D, Kaneider A, Novotny C, Kreuzer S, Riedl C, Minar E, Janata K, Herold CJ (2004) Value of negative spiral ct angiography in patients with suspected acute pe: analysis of pe occurrence and outcome. Eur Radiol 14(1): 93–98
Prologo JD, Gilkeson RC, Diaz M, Cummings M (2005) The effect of single-detector ct versus mdct on clinical outcomes in patients with suspected acute pulmonary embolism and negative results on ct pulmonary angiography. AJR 184(4): 1231–1235
Stein PD, Woodard PK, Weg JG, Wakefield TW, Tapson VF, Sostman HD, Sos TA, Quinn DA, Leeper KV Jr, Hull RD, Hales CA, Gottschalk A, Goodman LR, Fowler SE, Buckley JD (2007) Diagnostic pathways in acute pulmonary embolism: recommendations of the pioped ii investigators. Radiology 242(1): 15–21. doi:242/1/15[pii]10.1148/radiol.2421060971
Russo V, Piva T, Lovato L, Fattori R, Gavelli G (2005) Multidetector ct: a new gold standard in the diagnosis of pulmonary embolism? State of the art and diagnostic algorithms. Radiol Med 109(1–2):49–61; quiz 43–62
Stein PD, Woodard PK, Weg JG, Wakefield TW, Tapson VF, Sostman HD, Sos TA, Quinn DA, Leeper KV Jr, Hull RD, Hales CA, Gottschalk A, Goodman LR, Fowler SE, Buckley JD (2006) Diagnostic pathways in acute pulmonary embolism: recommendations of the pioped ii investigators. Am J Med 119(12): 1048–1055
Wells PS, Anderson DR, Rodger M, Stiell I, Dreyer JF, Barnes D, Forgie M, Kovacs G, Ward J, Kovacs MJ (2001) Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Ann Intern Med 135(2): 98–107
Wolf SJ, McCubbin TR, Feldhaus KM, Faragher JP, Adcock DM (2004) Prospective validation of wells criteria in the evaluation of patients with suspected pulmonary embolism. Ann Emerg Med 44(5): 503–510
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Material
The Below is the Electronic Supplementary Material.
Rights and permissions
About this article
Cite this article
Estrada-Y-Martin, R.M., Oldham, S.A. CTPA as the gold standard for the diagnosis of pulmonary embolism. Int J CARS 6, 557–563 (2011). https://doi.org/10.1007/s11548-010-0526-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11548-010-0526-4