
Abstract
Purpose
This study evaluated the incremental value and cost-effectiveness ratio of introducing coronary angiography (CA) with multidetector computed tomography (MDCT-CA) in the diagnostic management of patients with suspected coronary artery disease (CAD) compared with the traditional diagnostic workup.
Material and methods
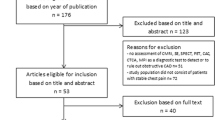
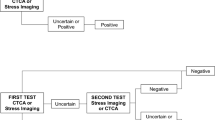
Five hundred and fifty consecutive patients who underwent MDCT-CA between January 2009 and June 2011 were considered. Patients with atypical chest pain and suspected obstructive CAD were directed to one of two diagnostic pathways: the traditional protocol (examination, stress test, CA) and the current protocol (examination, stress test, MDCT-CA, and CA, if necessary). The costs of each protocol and for the individual method were calculated. Based on the results, the cost-effectiveness ratio of the two diagnostic pathways was compared. A third, modified, diagnostic pathway has been proposed with its relative cost-effectiveness ratio (examination, MDCT-CA, stress test, and CA, if necessary).
Results
Stress test vs. MDCT-CA had an accuracy of 66%, a sensitivity and specificity of 21% and 87%, respectively, and a positive (PPV) and negative (NPV) predictive value of 40% and 70%, respectively. Comparison between conventional CA (CCA) and MDCT-CA showed a sensitivity and specificity of 92% and 89%, respectively, a PPV and NPV of 89%, and an accuracy of 92%. The traditional protocol has higher costs than the second protocol: 1,645 euro against 322 euro (mean), but it shows a better cost-effectiveness ratio. The new proposed protocol has lower costs, mean 261 euro, with a better costeffectiveness ratio than the traditional protocol.
Conclusions
The diagnostic protocol for patients with suspected CAD has been modified by the introduction of MDCT-CA. Our study confirms the greater diagnostic performance of MDCT-CA compared with stress test and its similar accuracy to CCA. The use of MDCT-CA to select patients for CCA has a favourable cost-effectiveness profile.
Riassunto
Obiettivo
Scopo del presente lavoro è stato valutare il valore incrementale dell’introduzione della angiografia coronarica mediante tomografia computerizzata multistrato (AC-TCMS) nella gestione diagnostica del paziente con sospetta malattia coronarica (CAD) rispetto al tradizionale workup diagnostico in termini di rapporto costo/efficacia.
Materiali e metodi
Sono stati considerati 550 pazienti consecutivi sottoposti ad AC-TCMS tra gennaio 2009 e giugno 2011. Sono stati considerati due percorsi diagnostici per pazienti con dolore toracico atipico e sospetta coronaropatia ostruttiva: il protocollo tradizionale (visita, stress test, coronarografia) e il protocollo attuale, (visita, stress test, AC-TCMS ed eventuale coronarografia). è stato calcolato il costo di ogni protocollo come la somma dei costi delle singole metodiche. Sulla base dei risultati i due percorsi diagnostici sono stati confrontati dal punto di vista del rapporto costo/efficacia. è stato proposto un terzo percorso diagnostico modificato con relativo rapporto costo/efficacia (visita, AC-TCMS, stress test, eventuale coronarografia).
Risultati
Lo stress test nei confronti dell’AC-TCMS ha attenuto valori di accuratezza del 66% con sensibilità e specificità del 21% e 87% e valore predittivo positivo (VPP) e valore predittivo negativo (VPN) di 40% e 70%. Il confronto tra ACC e AC-TCMS ha rilevato una sensibilità e specificità pari a 92% e 89%, un VPP e VPN pari a 89% per un’accuratezza complessiva del 92%. Il protocollo tradizionale è risultato avere costi più elevati rispetto a quello modificato dalla AC-TCMS, 1645 euro contro 322 euro (media), ma dimostra un miglior rapporto costo/ efficacia. Il nuovo protocollo proposto risulta avere costi minori, 261 euro in media, con un miglior rapporto costo/ efficacia, rispetto al protocollo tradizionale.
Conclusioni
Il protocollo diagnostico di un paziente con sospetta CAD ha subito variazioni con l’introduzione dell’AC-TCMS. Il nostro studio conferma una maggior performance diagnostica dell’AC-TCMS nei confronti del test da sforzo ed un’accuratezza simile a quella della coronarografia. Dai nostri dati, l’utilizzazione di un protocollo che prevede l’AC-TCMS come spartiacque principale per i pazienti da inviare alla coronarografia, risulta vantaggioso in termini di costo e di efficacia diagnostica.
Similar content being viewed by others

References/Bibliografia
Cademartiri F, Aldrovandi A, Palumbo A et al (2007) Multislice computed tomography coronary angiography: clinical applications. Minerva Cardioangiol 55:647–658
Cademartiri F, La Grutta L, Palumbo A et al (2007) Non-invasive visualization of coronary atherosclerosis: state-ofart. J Cardiovasc Med (Hagerstown) 8:129–137
Cademartiri F, La Grutta L, Palumbo AA et al (2006) Coronary plaque imaging with multislice computed tomography: technique and clinical applications. Eur Radiol 16(Suppl 7):M44–M53
Cademartiri F, Maffei E, Notarangelo F et al (2008) 64-slice computed tomography coronary angiography: diagnostic accuracy in the real world. Radiol Med 113:163–180
Cademartiri F, Maffei E, Palumbo A et al (2007) Diagnostic accuracy of 64-slice computed tomography coronary angiography in patients with low-to-intermediate risk. Radiol Med 112:969–981
Achenbach S, Giesler T, Ropers D et al (2001) Detection of coronary artery stenoses by contrast-enhanced, retrospectively electrocardiographically-gated, multislice spiral computed tomography. Circulation 103:2535–2538
Achenbach S, Ulzheimer S, Baum U et al (2000) Noninvasive coronary angiography by retrospectively ECGgated multislice spiral CT. Circulation 102:2823–2828
Schroeder S, Achenbach S, Bengel F et al (2008) Cardiac computed tomography: indications, applications, limitations, and training requirements: report of a Writing Group deployed by the Working Group Nuclear Cardiology and Cardiac CT of the European Society of Cardiology and the European Council of Nuclear Cardiology. Eur Heart J 29:531–556
Nieman K, Galema T, Weustink A et al (2009) Computed tomography versus exercise electrocardiography in patients with stable chest complaints: real-world experiences from a fast-track chest pain clinic. Heart 95:1669–1675
Cademartiri F, La Grutta L, Palumbo A et al (2009) Computed tomography coronary angiography vs. stress ECG in patients with stable angina. Radiol Med 114:513–523
Dewey M, Dubel HP, Schink T et al (2007) Head-to-head comparison of multislice computed tomography and exercise electrocardiography for diagnosis of coronary artery disease. Eur Heart J 28:2485–2490
Cademartiri F, Luccichenti G, Gualerzi M et al (2005) Intravenous contrast material administration in multislice computed tomography coronary angiography. Acta Biomed 76:86–94
Malago R, D’Onofrio M, Baglio I et al (2009) Choice strategy of different dose-saving protocols in 64-slice MDCT coronary angiography. Radiol Med 114:1196–1213
Maffei E, Martini C, De Crescenzo S et al (2010) Low dose CT of the heart: a quantum leap into a new era of cardiovascular imaging. Radiol Med 115:1179–1207
Detre KM, Wright E, Murphy ML, Takaro T (1975) Observer agreement in evaluating coronary angiograms. Circulation 52:979–986
Stacul F, Sironi D, Grisi G et al (2009) 64-Slice CT coronary angiography versus conventional coronary angiography: activity-based cost analysis. Radiol Med 114:239–252
Faccioli N, D’Onofrio M, Comai A, Cugini C (2007) Contrast-enhanced ultrasonography in the characterization of benign focal liver lesions: activitybased cost analysis. Radiol Med 112:810–820
Patterson RE, Eisner RL, Horowitz SF (1995) Comparison of costeffectiveness and utility of exercise ECG, single photon emission computed tomography, positron emission tomography, and coronary angiography for diagnosis of coronary artery disease. Circulation 91:54–65
Cademartiri F, Maffei E, Mollet NR (2008) Is dual-source CT coronary angiography ready for the real world? Eur Heart J 29:701–703
Maffei E, Palumbo A, Martini C et al (2010) Stress-ECG vs. CT coronary angiography for the diagnosis of coronary artery disease: a “real-world” experience. Radiol Med 115:354–367
Maffei E, Martini C, Tedeschi C et al (2011) Diagnostic accuracy of 64-slice computed tomography coronary angiography in a large population of patients without revascularisation: registry data in NSTEMI acute coronary syndrome and influence of gender and risk factors. Radiol Med 116:1014–1026
Maffei E, Palumbo A, Martini C et al (2011) Diagnostic accuracy of 64-slice computed tomography coronary angiography in a large population of patients without revascularisation: registry data and review of multicentre trials. Radiol Med 115:368–384
Maffei E, Palumbo A, Martini C et al (2011) Computed tomography coronary angiography in asymptomatic patients. Radiol Med 116:1161–1173
Meijboom WB, van Mieghem CA, Mollet NR et al (2007) 64-slice computed tomography coronary angiography in patients with high, intermediate, or low pretest probability of significant coronary artery disease. J Am Coll Cardiol 50:1469–1475
Meijboom WB, Weustink AC, Pugliese F et al (2007) Comparison of diagnostic accuracy of 64-slice computed tomography coronary angiography in women versus men with angina pectoris. Am J Cardiol 100:1532–1537
Pugliese F, Mollet NR, Hunink MG et al (2008) Diagnostic performance of coronary CT angiography by using different generations of multisection scanners: single-center experience. Radiology 246:384–393
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Malagò, R., Pezzato, A., Barbiani, C. et al. Role of MDCT coronary angiography in the clinical setting: economic implications. Radiol med 118, 1294–1308 (2013). https://doi.org/10.1007/s11547-013-0933-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-013-0933-z