
Abstract
Purpose
This paper aims to provide the tools for a complete anatomical evaluation of the coronary tree using 64-slice computed tomography (CT) and evaluate the prevalence of anatomical variants and anomalies in a population of 202 consecutive patients.
Materials and methods
Two hundred and two patients with suspected coronary artery disease underwent 64-slice CT with a standard protocol. Two observers working in consensus evaluated and collected the data regarding anatomical variants and anomalies of the coronary vessels.
Results
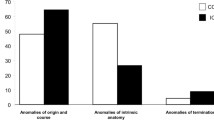
In the 202 consecutive patients, the prevalence of anatomical variants was: left dominant circulation (7%), absent left main (5%), presence of intermediate branch (17%), aortic origin of conus branch (13%) and circumflex origin of sinus node branch (15%). Coronary anomalies (origin and course, intrinsic and termination) showed an overall prevalence of 25%.
Conclusions
CT is the ideal method for the three-dimensional evaluation of the coronary tree. Anatomical variants and anomalies of the coronary arteries are quite common and should be known and recognised promptly by the operators.
Riassunto
Obiettivo
Fornire gli strumenti per una completa valutazione anatomica del circolo coronarico mediante TC a 64 strati e valutare la prevalenza di varianti ed anomalie in una popolazione di 202 pazienti consecutivi.
Materiali e metodi
Duecentodue pazienti con sospetta malattia coronarica sono stati sottoposti a TC delle coronarie a 64 strati con protocollo standard. Due osservatori in consenso hanno valutato la presenza di varianti anatomiche e anomalie dei vasi coronarici.
Risultati
Nei 202 pazienti consecutivi arruolati per lo studio la prevalenza delle varianti anatomiche è risultata: dominanza sinistra (7%), tronco comune assente (5%), presenza di ramo intermedio (17%), origine aortica del ramo del cono (13%), origine dalla circonflessa dell’arteria del nodo del seno (15%). Le anomalie coronariche di origine e decorso, intrinseche e di terminazione hanno mostrato una prevalenza complessiva del 25%.
Conclusioni
La TC è uno strumento ideale per la valutazione tridimensionale del circolo coronarico. Le varianti e le anomalie coronariche sono un reperto molto comune che deve quindi essere riconosciuto agevolmente dall’operatore.
Similar content being viewed by others


References/Bibliografia
Luccichenti G, Cademartiri F, Romana Pezzella F et al (2005) 3D reconstruction techniques made easy: know-how and pictures. Eur Radiol 15:2146–2156
Hendel RC, Patel MR, Kramer CM et al (2006) ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol 48:1475–1497
Duran C, Kantarci M, Durur Subasi I, Gulbaran M et al (2006) Remarkable anatomic anomalies of coronary arteries and their clinical importance: a multidetector computed tomography angiographic study. J Comput Assist Tomogr 30:939–948
Cademartiri F, Nieman K, Raaymakers RH et al (2003) Non-invasive demonstration of coronary artery anomaly performed using 16-slice multidetector spiral computed tomography. Ital Heart J 4:56–59
Dodd JD, Ferencik M, Liberthson RR, Cury RC et al (2007) Congenital anomalies of coronary artery origin in adults: 64-MDCT appearance. AJR Am J Roentgenol 188:138–146
van Ooijen PM, Ho KY, Dorgelo J, Oudkerk M (2003) Coronary artery imaging with multidetector CT: visualization issues. Radiographics 23:e16
Mahesh M (2002) Search for isotropic resolution in CT from conventional through multiple-row detector. Radiographics 22:949–962
Kalender WA, Seissler W, Klotz E, Vock P (1990) Spiral volumetric CT with single breath-hold technique, continuous transport, and continuous scanner rotation. Radiology 176:181–183
Cademartiri F, Runza G, Belgrano M et al (2005) Introduzione all’imaging coronarico con tecnologia TC a 64 strati. Radiol Med 110:16–41
Sato Y, Shiraga N, Nakajima S et al (1998) Local maximum intensity projection (LMIP): a new rendering method for vascular visualization. J Comput Assist Tomogr 22:912–917
Fishman EK, Magid D, Ney DR et al (1991) Three-dimensional imaging. Radiology 181:321–337
Lu B, Dai R, Bai H et al (2000) Evaluation of electron beam tomographic coronary arteriography with three-dimensional reconstruction in healthy subjects. Angiology 51:895–904
Achenbach S, Ropers D, Regenfus M et al (2000) Diagnostic value of 2- and 3-dimensional image reconstruction techniques for the detection of coronary artery stenoses by contrast-enhanced electron-beam CT. J Am Coll Cardiol 35[Suppl A]:416
Wildermuth S, Leschka S, Duru F, Alkadhi H (2005) 3-D CT for cardiovascular treatment planning. Eur Radiol 15[Suppl 4]:D110–D115
Alegria JR, Herrmann J, Holmes DR et al (2005) Myocardial bridging. European Heart Journal 26:1159–1168
Austen WG, Edwards JE, Frye L et al (1975) A reporting system on patients evaluated for coronary artery disease: report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 51:5–40
Detre KM, Wright E, Murphy ML et al (1975) Observer agreement in evaluating coronary angiograms. Circulation 52:979–986
Alderman E, Stedius M (1992) The angiographic definitions of the Bypass Angioplasty Revascularization Investigation study (BARI). Coron Artery Dis 3:1189–1207
Pannu HK, Jacobs JE, Lai S et al (2006) Coronary CT angiography with 64-MDCT: assessment of vessel visibility. AJR Am J Roentgenol 187:119–126
Angelini P, Velasco JA, Flamm S (2002) Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation 105:2449–2454
Scanlon PJ, Faxon DP, Audet AM et al (1999) ACC/AHA guidelines for coronary angiography. A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Coronary Angiography). Developed in collaboration with the Society for Cardiac Angiography and Interventions. J Am Coll Cardiol 33:1756–1824
Cademartiri F, Marano R, Luccichenti G et al (2004) Anatomia normale del circolo coronarico con tomografia computerizzata multistrato a 16 canali Radiol Med 107:11–23
Baltaxe HA, Wixson D (1977) The incidence of congenital anomalies of the coronary arteries in the adult population. Radiology 122:47–52
Click RL, Holmes DR, Vlietstra RE et al (1989) Anomalous coronary arteries: location, degree of atherosclerosis and effect on survival-a report from the Coronary Artery Surgery Study. J Am Coll Cardiol 13:531–537
Yamanaka O, Hobbs RE (1990) Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 21:28–40
Rigatelli G (2003) Coronary artery anomalies: what we know and what we have to learn. A proposal for a new clinical classification. Ital Heart J 4:305–310
Mohlenkamp S, Hort W, Ge J et al (2002) Update on myocardial bridging. Circulation 106:2616–2622
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cademartiri, F., Malagò, R., Grutta, L.L. et al. Coronary variants and anomalies: Methodology of visualisation with 64-slice CT and prevalence in 202 consecutive patients. Radiol med 112, 1117–1131 (2007). https://doi.org/10.1007/s11547-007-0210-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-007-0210-0